

Shedding Part 4 - Evidence of Placental and Breast Milk Transmission of Covid mRNA Vaccine Components

The first three posts (Part 1, Part 2, Part 3) in this series provided evidence of the following:
The FDA and the EMA define the mRNA vaccines as gene therapies.
The FDA requires that gene therapy products undergo human shedding studies given the known risks of shedding
One nanoparticle gene therapy (Luxterna), already on the market, warns that the product can be excreted in tears and nasal discharge
All three vaccine components (mrNA, the lipid nanoparticle, and the spike protein) distribute widely in the human body (contrary to promises of remaining localized in the arm) and for prolonged periods.
Numerous studies have demonstrated that synthetic LNP’s containing genetic material or drugs can be absorbed by various routes including intranasal, transcutaneous, transfollicular, transdermal and inhalation via the lungs.
LNPs retain their biologic activity after being absorbed no matter what route is used.
Now we will move towards assembling evidence of transmission of Covid mRNA vaccine components which then cause illness in others.
The title of this review paper is concerning: “Toxicity of Nanoparticles on the Reproductive System in Animal Models: A Review.” This paragraph raises serious questions:
Nanoparticles (NPs) are associated with different disorders in animals, including pulmonary injury, hepatotoxicity, immuno-nanotoxicity neurotoxicity, renal toxicity, and irreversible testis damage (Derfus et al., 2004; Chou et al., 2008; Lin et al., 2008; Schipper et al., 2008; Wu et al., 2011; Bartneck et al., 2012; Vance et al., 2015).
Similarly, NPs present a potential threat to the susceptible female population, and their toxicity has been studied in different models of female reproductive health (Tsuchiya et al., 1996; Wang et al., 2011). Both short- and long-term toxicities in animals and humans have been documented. Additionally, several reports demonstrate the biological effects of NPs on isolated physiological systems, such as organs, biomolecules, and primary cells. Overall, such studies have raised as many questions as they have answered, and it is clear that more studies are needed to determine the mechanisms by which NPs affect particular organ systems. NPs can also cross the biological barriers shielding various parts of the human body, such as the blood-testes barrier and enter the testes in animal models (Araujo et al., 1999).
Trans-placental Transmission/Shedding
First, lets start with asking whether a vaccinated mother can transmit spike or mRNA to a developing fetus in the womb, i.e “trans-placentally.” Animal studies clearly indicate that nanoparticles can transit through ordinary placental transcellular transport. In that paper, they wrote:
So, from the above, they found that nanoparticles under 240 nanometers can pass readily to the placenta? Lets again review the size of the Pfizer and Moderna lipidnanoparticles (LNP’s). Chat GPT (sorry) states “These LNPs generally fall within a range of approximately 80 to 200 nanometers in diameter.” However, another paper reported that the LNP’s range from 100 to 400, however, that still leaves a significant proportion being small enough to cross to the fetus via the placenta.
The above study must be interpreted in the context of the evidence I presented in Part 2 whereby all vaccine components can be detected in the blood with studies reporting various time periods of one week, 14 days, 4 months, and up to 187 days (or longer). Thus, based on the study above and the fact that the vaccine products enter and remain in the bloodstream, trans-placental transmission must be occurring.
Now, to be fair, PEG-coated LNPs (like in the vaccines) are reported to have less diffusion across the placental barrier than liposome-based formulations, but are still able to deliver some of their cargo to the fetus.
To wit, in one mouse study, they developed a PEG-ylated LNP similar to the COVID mRNA vaccines that could get to the uterus as a therapeutic delivery mechanism. Apparently they succeeded. The study conclusion: “These LNPs may provide a platform for in utero mRNA delivery for protein replacement and gene editing.”
But even if PEG limits the crossing of the placenta, that just means it would limit the transmission of the synthetic LNP’s, not the natural exosomes which contain spike or free spike (which we also know is in the blood).
Now although all the animal papers emphasize that it is difficult to extrapolate to humans, these data cannot rule out that the components and products of the mRNA vaccines are capable of reaching the fetus of a vaccinated mother during pregnancy.
So, is there data showing risks to fetuses in pregnancy?
Unsurprisingly and unfortunately, the answer is a resounding yes. Let’s start, again, with this document obtained by FOIA from Pfizer and their (P)FDA:
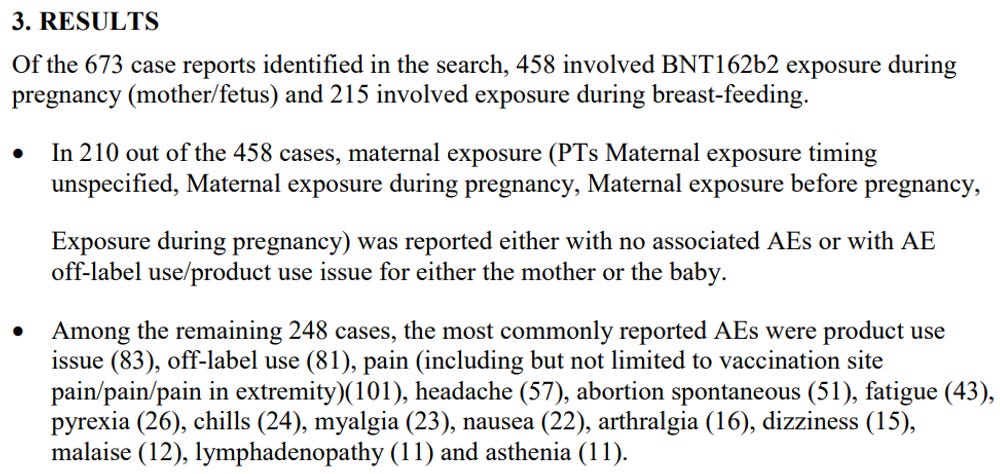
To summarize the above, Pfizer received 458 reports of mothers “exposed’ (what an odd word) to the vaccine while pregnant. In 248 (54%) reports, an adverse event was reported.
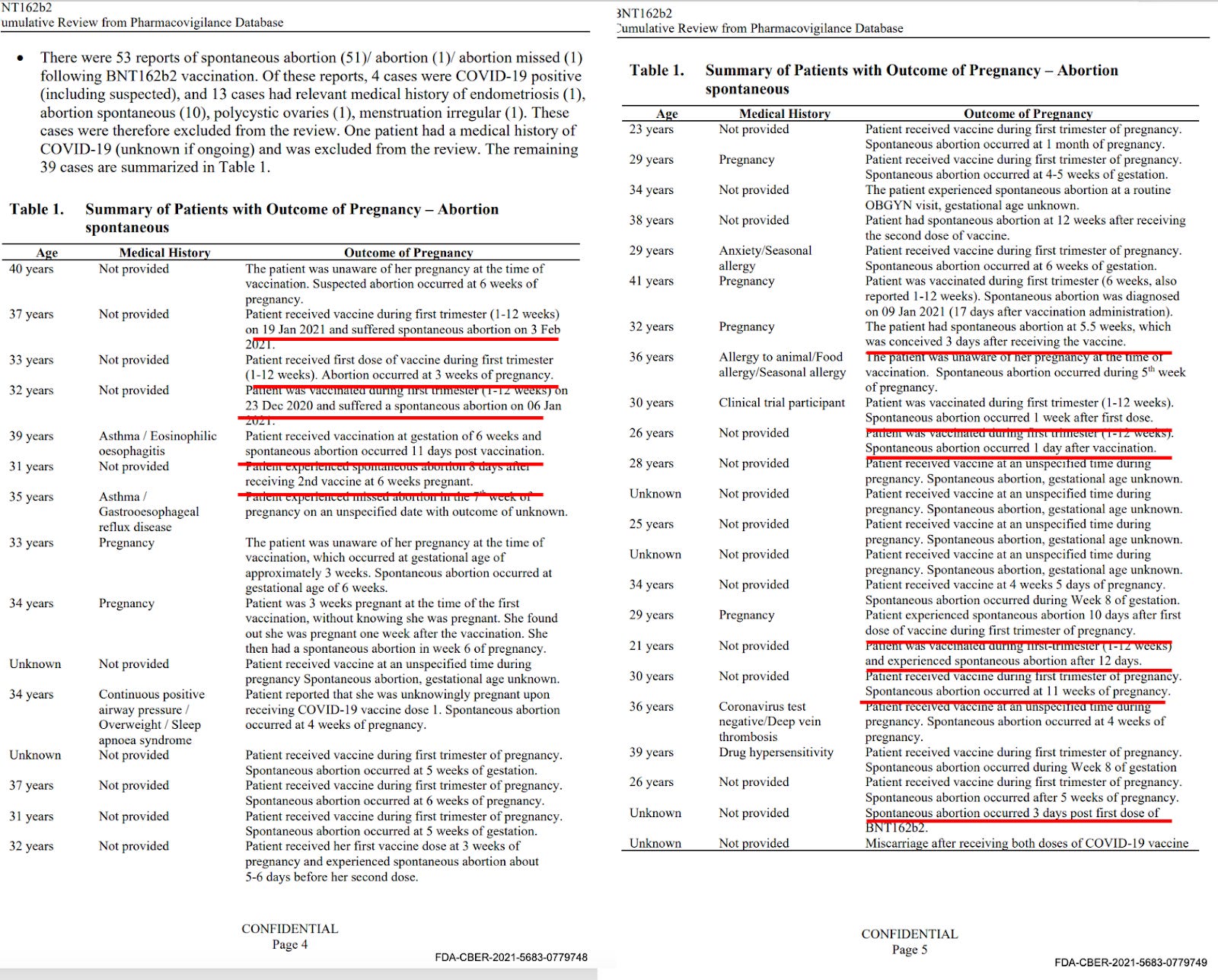
53 of the 248 adverse events involved spontaneous abortion, which they then “excluded” 17 due to having comorbidities or history of spontaneous abortion (not cool but whatever). This left them with 39 of the 248 adverse events (8.5%) resulting in spontaneous abortion. Now, although this rate of spontaneous abortion is consistent with traditional rates in pregnancy, the temporal association with vaccination in many of the reports is, to me as a clinician, highly concerning.
For instance, there are an uncomfortable amount of spontaneous abortion reports within 1-10 days of the vaccine, and then a large number where the temporal association is left quite vague, i.e. “received vaccination in first trimester and abortion occurred at 6 weeks.” This suggests vaccination occurred right before the spontaneous abortion (given that the average time that women realize they are pregnant is at 5.5 weeks from conception). Take some time to peruse the below list of events:
But beyond this Pfizer data, is there any other evidence of the reproductive harms of the mRNA vaccines?
There is actually a mountain of data to contend with.
One team of researchers performed a survey study after one of them observed “my period after dose one was one of the heaviest I remember having ever in my life.” So she and a colleague elicited reports of menstrual abnormalities from Covid vaccinated women. They were quickly deluged with 140,000 reports. Published in Science, they found that 42% of women reported menstrual abnormalities related to the vaccine. 42%. Let that sink in
It was so troubling, it brought out a team of credentialed fact checkers as in this article from the “Science Media Center”:

They assembled a team of “experts” with quotes similar to this one below, all trying to dismiss the importance of the study:
Dr Michelle Wise, Senior Lecturer, Department of Obstetrics and Gynaecology, University of Auckland, comments:
“Unfortunately, this is not high quality research and I would not put a lot of credence on its findings. In the introduction, they call it an exploratory study, and that is all it is, they are exploring the effect of the vaccine on menses. It is a descriptive study, where they describe a large case series of almost 40,000 people who got the vaccine, and the key finding was that you were equally likely to have no change in your next period as you were to have a heavier next period.
No comment.
Now, although not published, I have been informed by a colleague in communication with an anonymous whistleblower working at a fertility clinic that they have been seeing not only large declines in successful fertilization but also “strange embryos” forming.
The national expert on the risks of the mRNA vaccines in pregnancy is Jim Thorpe, a friend, colleague, and highly accomplished national expert in maternal-fetal medicine. He is also one of the only Ob-Gyn’s in the country who immediately spoke out publicly against the CDC’s decision to recommend injecting pregnant women with mRNA vaccines. A recent quote of his is a particularly sobering reminder of how unprecedented the actions of public health agencies were in regards to pregnant women:
“the CDC is breaking the “golden rule” of pregnancy. “The golden rule of pregnancy is you don’t ever, ever use a novel substance in pregnancy, ever,” he said. “And you don’t have to be a physician or nurse, you don’t have to have any education, to know that.”
He, like me, also lost his job due to his common sense advocacy. The American Board of Ob-Gyn even tried to go after him but now is backing off since the publication of his study finding unprecedented signals of harm from the Covid mRNA vaccines.
In that study, Thorp et al analyzed the VAERS database using a CDC established method for detecting vaccine danger signals called “the proportional reporting ratio” (PRR). The PRR is calculated by comparing Covid mRNA vaccine adverse event report rates compared to the influenza vaccine adverse event report rates (i.e. the flu vaccine is used as the baseline standard for “safety”). The CDC states that a PRR of two or greater is a safety signal “that requires further study.”
The two figures below show the PRR’s for eleven pregnancy related outcomes. The first on the left calculates it by number of doses given and the second to the right by number of persons vaccinated. Note how “off the charts” the PRR’s are. Depending on comparator method, having “abnormal menses” ranges from an RR of 298 to 4927 (i.e. well over the threshold of 2). With miscarriages, the PRR ranges from 15-57.
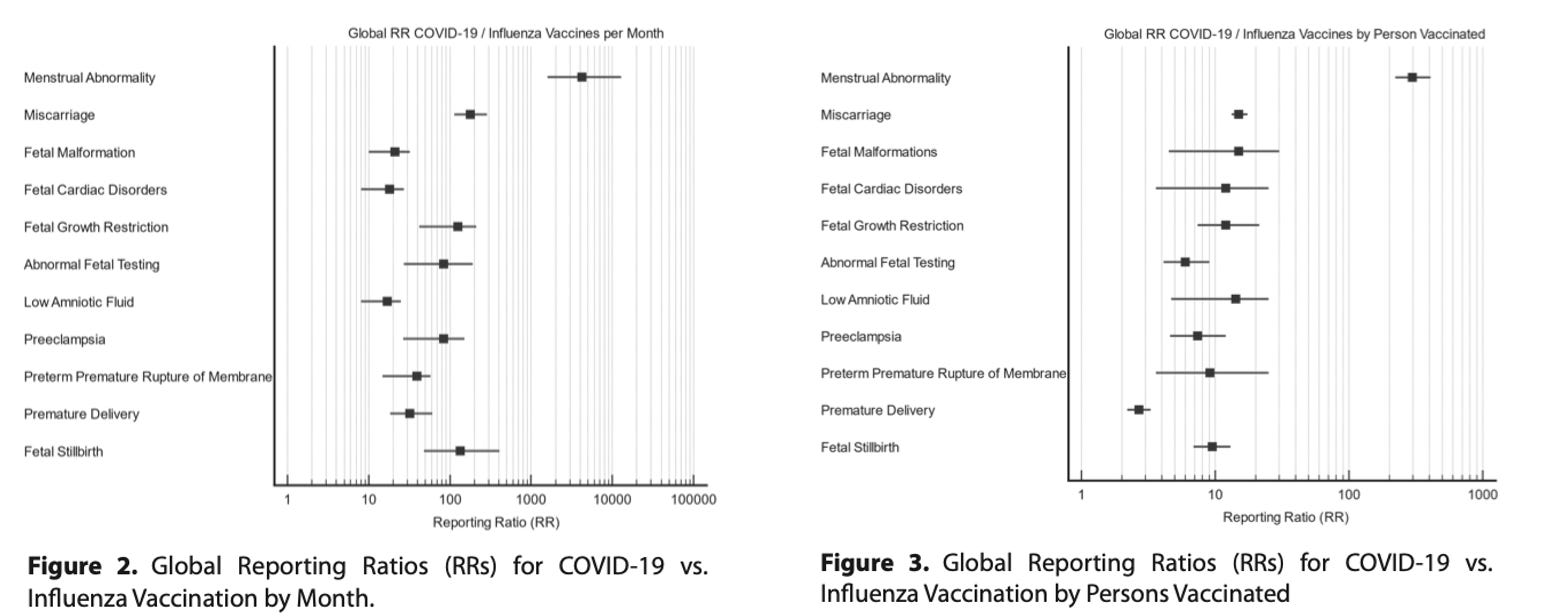
Note the conclusion by his team of authors: “These results necessitate a worldwide moratorium on the use of COVID-19 vaccines in pregnancy.”
The finding of PRR’s far exceeding 2 for every pregnancy related outcome should have, per the CDC’s words, “warranted further study.” So maybe they should have immediately stopped recommending them to pregnant women while they did that?
Apparently not. Fierce, unstoppable regulatory capture on display again as recently as a month ago:
Recall that Thorp is an actively practicing maternal fetal medicine specialist and has seen firsthand the toxicity in pregnancy. In an article from the Defender, Thorpe is quoted as saying
“The mRNA COVID-19 vaccines are the deadliest drug in the history of medicine, whether you call it a vaccine, a drug, a gene medicine, a medical intervention, whatever you call it. And they knew it. The CDC knew it. HHS knew it. Pfizer knew it and tried to bury the data, which showed 1,223 deaths from its vaccine in the first 10 weeks, for 75 years.”
Finally, the investigative journalist Mary Beth Pfeiffer (and my sometime Op-Ed writing partner here and here) reported on suddenly dropping birth rates across many European countries timed 9 months after the ramping up of their respective vaccine campaigns.
But again, although it is abundantly clear how toxic the mRNA vaccine is to pregnant women, I cannot definitively state that it is solely from transmission of vaccine contents or spike product to the fetus. The reason for this uncertainty is that there are several other pathologic mechanisms which could explain these outcomes like hypercoagulable blood/”microclotting,” endothelial damage, autoimmune responses, hyperinflammation to name just a few of the many identified mechanisms of injury in the new, as yet unrecognized field of “spikeopathy.”
Breast Milk Transmission/Shedding
So, although the devastating outcomes in pregnancy are not definitive proof of shedding/transmission, when we start to look at reports of infants and babies falling ill after breast feeding, the reality of the transmission of gene therapy products from mother to baby via breast milk is easier to identify.
This study found that the vaccine mRNA was found in the milk of 1/10 women studied (4/40) in the first week after vaccination with mRNA vaccine (either after dose 1 or dose 2). Amounts can reach 2 ng/mL of milk.
Although the authors did not think this represented a “significant” amount, in Banoun’s masterful review paper on shedding, she explains:
This amount may seem small compared to the 30 micrograms of mRNA injected with the vaccine, but it can be enough to produce a significant amount of spike.
Indeed, an infant makes several feedings per day, for approximately 240 to 360 mL per day and a total over a week of 1680 to 2,520 mL in the first week. The newborn, weighing between 2 and 5 kg, could therefore be exposed to a dose of 5 μg of mRNA in its first week. This seems disproportionate compared to the 10 μg injected into children aged 5 to 11 years who weigh approximately 18 to 35 kg respectively [39]. The method used in the latter study is more sensitive than that of Golan et al. who did not find mRNA in milk [40].
This study in the Lancet reported on the breast milk of 11 women who were vaccinated with mRNA within 6 months of delivery. They found trace amounts of mRNA in 7 samples from 5 different participants at various times up to 48 hours post vaccination. The vaccine mRNA appeared in higher concentrations in the extracellular vesicles (i.e. exosomes/nanoparticles) than in whole milk. Uh oh.
Their conclusion: “Our findings demonstrate that the COVID-19 vaccine mRNA is not confined to the injection site but spreads systemically and is packaged into breast milk extracellular vesicles.”
Another study found PEG (a component of the mRNA vaccine) as well as Covid vaccine mRNA in breast milk as shown below.
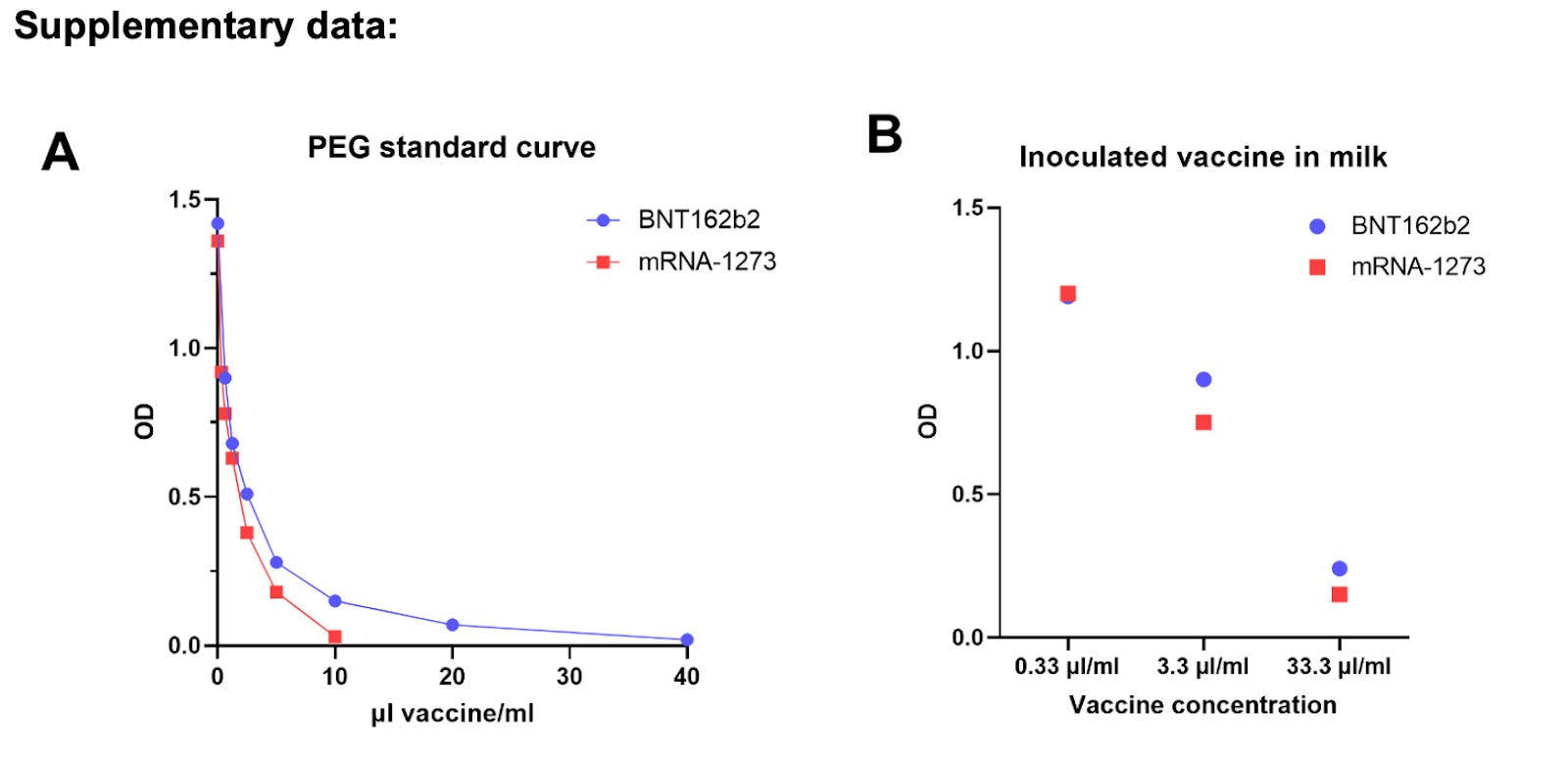
Note they say “Of note, PEGylated proteins concentration is higher in mRNA-1273 compared to BNT-162b2 which also stand in line with mRNA concentration in each vaccine (ready for administration vaccines were used).” So, a dose-response relationship was found which is particularly damning - the more you give, the more you get (in breast milk).
Despite this, like in the paper above, they say without explaining what should be considered significant, “PEGylated proteins were not found at significant levels in milk after vaccination.”
The one reassurance here is that in the first study, no Covid vaccine mRNA was found in breast milk after 48 hours from the jab. However, it would have been nice for American mothers to know this before being told to get vaccinated, i.e. they could have been instructed to take the first couple of days off of breastfeeding (easier said than done I am told). Instead, the CDC continues to recommend offering the COVID-19 mRNA vaccines to breastfeeding individuals.
So, we know mRNA can be transmitted to breastfed babies in breast milk. I used to dismiss the importance of this finding by reasoning that the stomach acid of the baby would destroy the mRNA it and render it inert. But then I found these papers (here, here, and here), one of which stated:
It has been known for some years that mRNA encapsulated in extracellular vesicles is protected from gastric juices and can transfect intestinal cells. A recent review by Melnik and Schmitz confirms that milk EVs survive the extreme conditions of the gastrointestinal tract, are internalized by endocytosis, are bioavailable, reach the bloodstream, and penetrate peripheral tissue cells. Beyond integration into the genome, other concerns should arise such as provoking an “immunogenic” reaction to mRNA.
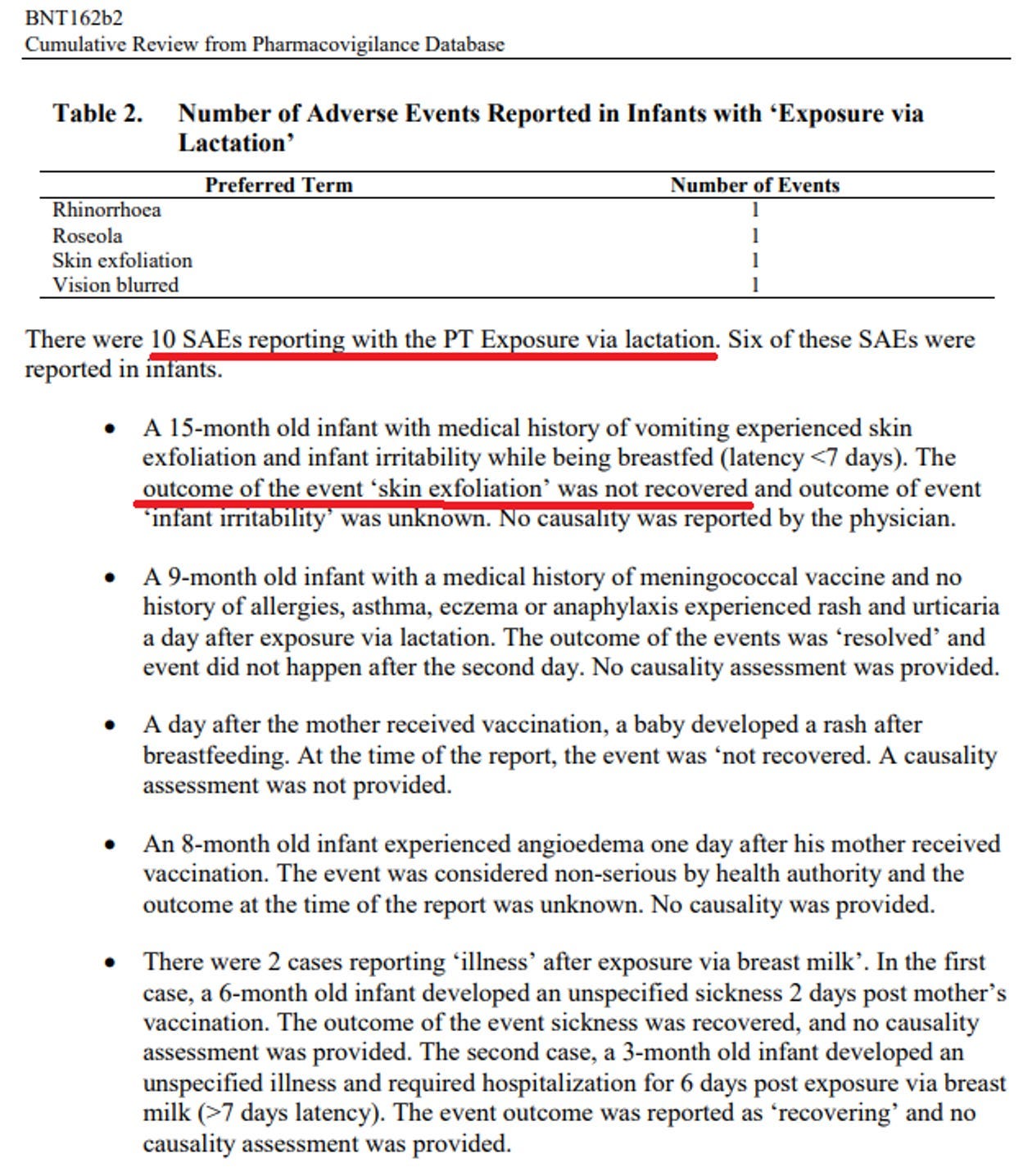
Clinical evidence suggesting that the mRNA and/or spike in breast milk can survive in the stomach and cause illness in the baby lies in the below list from an eight-page confidential document of reports made to Pfizer by lactating women who were vaccinated. Pfizer was aware of and tracking adverse events in babies “exposed” to the mother’s vaccination via breast milk.
While medical journal propagandized OB/GYNs all over the world were lecturing their pregnant patients to get the experimental shots, Pfizer was observing what was graded as non-severe adverse events (AEs) in a whopping 20% of the 215 lactating women reporting “exposure” to the vaccine.
The report also documents 10 serious AEs, including facial paralysis (not listed under “serious” interestingly), lymphadenopathy (swelling of lymph nodes that could be associated with cancer), and blurred vision. Note these are all side effects of the vaccines reported by adults. Among infants, reports included skin exfoliation, rashes, swollen skin, and unspecified sickness. That’s a high percentage of serious AEs in babies for any therapy.
More evidence: A study published a year ago in JAMA revealed that 3.5% of women reported a decrease in breast milk supply and 1.2% reported “issues with their breastmilk-fed infant after vaccination.” This latter stat is truly troubling - 1.2% of moms reported a temporal association between vaccination and “issues with their infant.” As I have said throughout my career, mothers (and some fathers) are the best “clinicians” that I have ever seen in that they are highly keen observers and recorders of both the timing, pattern, triggers, and alleviators of their children’s symptoms and illness. Taking a history of illness from a keenly observant mother is a pleasure actually as you can gather all the truly critical information you need to make diagnoses and decide on treatment. But forgive me for I digress.
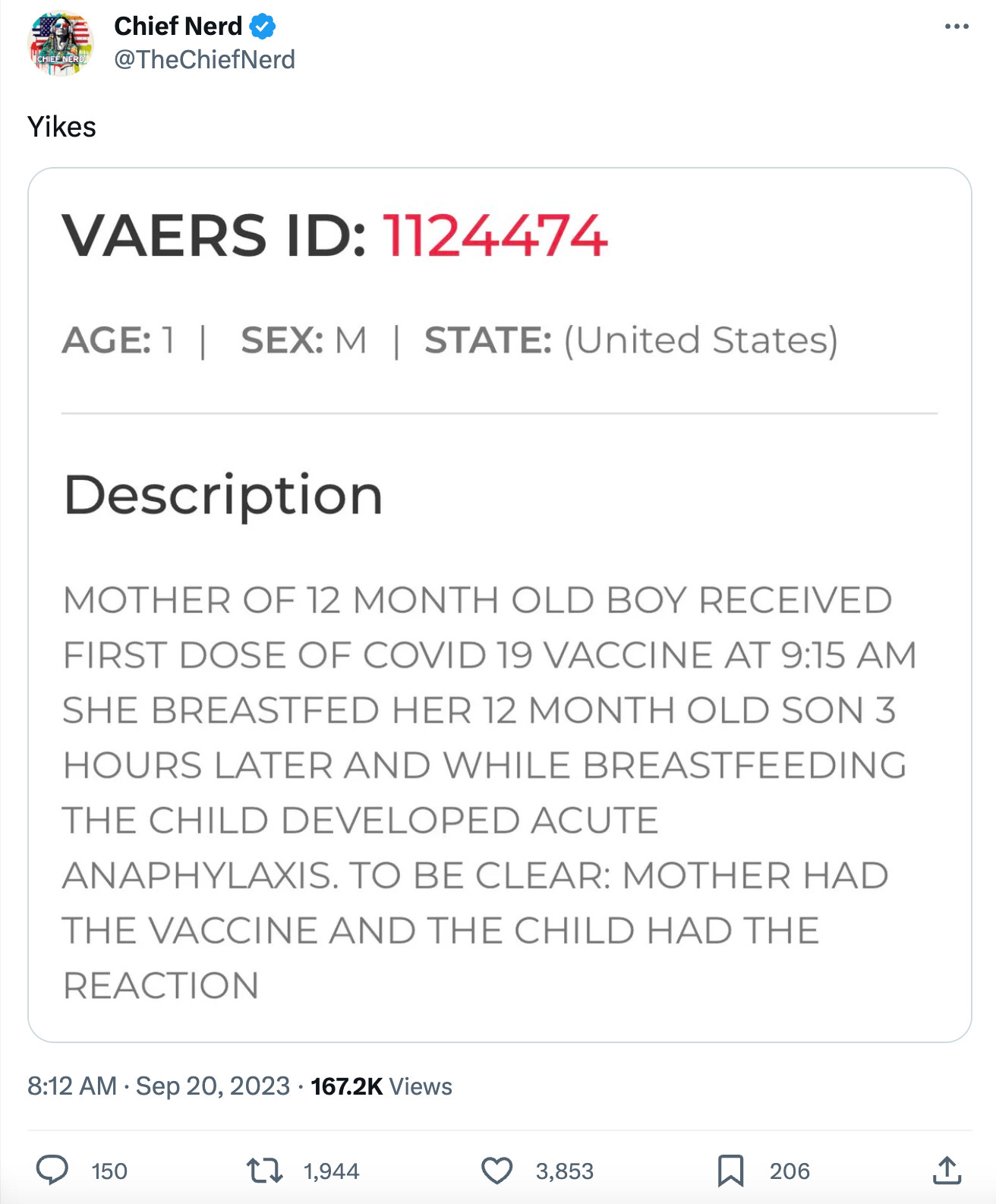
Now, it only leaves the question whether the babies are falling ill from the LNP/mRNA in breast milk or the resulting spike in breast milk. I believe that, in most cases, it is the spike that is being transmitted and causing illness rather than the LNP or modified mRNA given that the symptoms caused are not only common to Long Vax, but to Long Covid as well (the latter syndrome does not involve lipid nano-particles or modified mRNA). However, the well described pro-inflammatory properties of LNP’s suggest that just the LNP’s could cause illness itself.
Here is one vivid VAERS entry which could represent spike or the LNP in breast milk:
Further, the investigative reporter Sonia Elijah combed through the EU’s Periodic Safety Update reports and discovered that Pfizer documented numerous cases of strokes, convulsions, and respiratory failure among nursing babies. Ironically, appallingly, and counterintuitively, Pfizer refused to investigate further because these AEs were automatically dismissed as unrelated to the vaccine. Why? Because Pfizer simply removed them from the analysis!
In the words of the Pfizer investigator, these serious AEs were “determined to be non-contributory and were not included in the discussion since these cases involved exposures to the vaccine during the mother’s pregnancy or through breastfeeding.” Absurd:
Pharma and its (P)FDA does what it does and little consequences follow.
Links to all the other posts in this series is after the subscribe button below.
P.S. I just want to say thanks to all my subscribers, especially the paid ones! Your financial support is greatly appreciated as it allows me to devote what is often large amount of time I spend researching and writing my posts, so again, thanks. - Pierre
“Shedding” Part 1- Shedding of Covid mRNA Vaccine Components and Products From The Vaccinated to the Unvaccinated - Part 1
“Shedding” Part 2 - The Bio-Distribution and Excretion Potential of Covid mRNA Vaccine Products
“Shedding” Part 3 - Can You Absorb Lipid Nanoparticles From Being Exposed To a Vaccinated Person?
“Shedding” Part 4 - Evidence of Placental and Breast Milk Transmission of Covid mRNA Vaccine Components
"Shedding" Part 5 - Evidence of Shedding Causing Illness In Others
“Shedding Part 6- Clinical Case Notes Describing Shedding Phenomena Among Leading Edge Clinic Patients
“Shedding” Part 7 - Shedding Via Sexual Intercourse - Clinical Reports
“Shedding” Part 8 - A Deluge of Clinical Reports Pour In
“Shedding” Part 9 - More and More Clinical Case Descriptions of Shedding Pour In
P.P.S - Proud to report that my book is gaining Best Seller status on Amazon in several countries and is climbing up the U.S Amazon rankings… Link:

Dr Thorpe’s comment about the golden rule of never giving a novel product to a pregnant woman… and yet it seems all of the universe lost their minds and complied.
A physician friend of mine - pregnant - got the damn booster recently. Because she was flying overseas. And was scared of getting sick. Asked three OBs about it, and they ALL SAID YES.
I just cannot even begin to formulate words to describe the lunacy and the brainwashing.
Thank you Dr. Kory . I too , as an unjabbed ob/gyn, lost my job. I’m better off. The placental abruptions and second trimester losses , were all getting to me mentally and the residents were too woke for words. I do office work only now and this affords me the opportunity to explain to women, not to take the jab. ACOG still recommends the jabs . (That’s a whole other discussion both medically and legally when discussing “standard of care “) Thanks again , and I direct many to FLCCC . You and Dr. Marik have been awesome 👏🏻.