

How the FDA Buried the Dangers of Antidepressants
The previous struggles with the FDA have so much to teach us about how the FDA has handled the COVID-19 vaccines.

I stopped working as a system doctor for several reasons, one of which is that I was horrified at what was being done to patients. From before and since that time, I’ve discovered how many medications have created profound consequences for many I’ve crossed paths with.
When my friend and colleague “A Midwestern Doctor” (AMD) wrote a recent deeply referenced post about how SSRI antidepressants can cause homicidal psychosis, I was shocked. Not so much at the knowledge of the link between the two, something that I had been aware of, but I was stunned to discover just how much evidence there is substantiating that link.
AMD argues the most important lesson to take from this catastrophe is not the dangers of these drugs, but rather how the FDA was complicit in this disaster. It’s a fact of life that corporations and individuals will always lie for their own benefit, and it is for that reason that we have regulators in place to prevent them from causing too much damage. Regulatory capture describes a state where the regulator has been bought out by the parties it is supposed to police, and we are thus left in a situation where no one remains to protect us from unchecked greed.
We have seen this throughout COVID-19, where, after running a Disinformation campaign against the use of effective repurposed drugs like hydroxychloroquine and ivermectin, a dubious vaccine was approved without most of the necessary data to approve it. Then, as soon as the vaccines entered the market, the captured FDA was deluged with an unprecedented number of reports of severe complications from the drugs, and instead of doing its job pretended those complications did not exist and pushed the vaccine onto the entire population.
What happened with the SSRIs is equally appalling and demonstrates a degree of government malfeasance and regulatory capture I would never have believed was possible had I not seen it happen with my own eyes throughout COVID-19. Exactly how the FDA worked for decades to protect the SSRIs from repeated attempts to restrict their use by citizens, Congressmen, and even its own staff provides pivotal lessons for the enormous task in front of us.
I am proud to host this post, written by A Midwestern Doctor from the Substack “The Forgotten Side of Medicine.”
In the first part of this series (which must be read before this part), I argued that selective serotonin reuptake inhibitors (SSRI antidepressants) provide minimal benefit (only a minority of users benefit from the drugs), and frequently cause significant harm. The side effects vary greatly, and I’ve lost count of just how many people I know who have been severely harmed by these drugs. By the same token, I believe they have seriously damaged the fabric of American society:
Shortly after I published this article, Kim Witczak reached out to me to share a variety of things I did not previously know about these drugs. Witczak, who lost her husband to a tragic SSRI suicide, was one of the leading activists who worked tirelessly through the courts and political process to get warning labels placed on the SSRIs after the heart-wrenching death of her husband. For that reason, I revised the above article after it was originally published to include information she shared with me and realized that this article on the FDA’s malfeasance needed to be updated since there was a great deal I had not mentioned that needed be shared.
.
Widespread Medical Injuries
The medical field’s business model requires the gaslighting of patients it injures so that the public doesn’t stop buying its products—you are always fighting an uphill battle to have an injury recognized. Since a foundational tenet of medical gaslighting is to insist that the patient’s injury arose from a pre-existing medical condition (e.g., all your issues are just from anxiety), if the medical injury causes neurologic damage which in turn creates psychiatric issues, it is often a lost cause to convince the doctor that their treatment created those issues.
In some ways, I believe allopathic (conventional) medicine is extraordinarily advanced, but in other ways, it is very primitive. One of its major problems compared to many other systems that have existed throughout history, is that it fundamentally does not grasp the nature of the human mind, or how the mind affects the body and spirit (conversely, I consider this to be one of the most fascinating subjects in medicine).
I believe that this issue fundamentally arises because so much of medicine is about having a standardized box you can quickly fit patients into, do something for, and then move on to the next one (after all how else could we justify charging so much for such a brief visit). Because the mind is such a dynamic and vibrant organism, doing something simplistic like this metaphorically kills it—but since the entire history of Western medicine has been about controlling nature, it is not surprising how often it also tries to dominate the human mind. Although many severe side effects follow SSRI administration, one of the reactions that most upsets me (due to how common it is) is the degree to which SSRIs dampen the vibrancy of the human mind and spirit—something I am sure many of you can relate to.
Frequently when I talk with people who, to varying degrees, have lost their minds from psychiatric medications, it is both fascinating and horrifying how many different ways that the drugs can damage and alter people’s minds. For example, one common SSRI side effect I’ve heard of (which lasts long after the drugs are discontinued) is brain zaps, where as the name implies, people feel electrical flashes travel through their brains, and quite a few people have told me that these zaps prevented them being able to put together many of the thoughts they had previously had no trouble with.
Sadly, while the psychiatric field recognizes that this issue exists, it’s viewed as an enigma and has had no effect on curbing the prescription of these drugs. This is astounding when you think about it.
Similarly, loss of libido is a significant complication of the SSRIs (and one that often lasts long after the drugs are discontinued) I frequently hear people I know complain about. In one large study of the five most commonly used SSRIs, Peter Gøtzsche calculated the weighted average of the data, he concluded that of those on SSRIs:
57% experienced decreased libido
57% experienced delayed orgasm or ejaculation
46% experienced no orgasm or ejaculation
31% experienced erectile dysfunction or decreased vaginal lubrication.
Given that 40% of those on the medications considered this side effect unacceptable, it is a particularly cruel complication as it is almost guaranteed to make you depressed and the stated purpose of these drugs is to treat depression (which more often than not they don’t). While this has not affected the psychiatric profession’s prescribing or promotion of these drugs, it has been indirectly acknowledged as SSRIs are sometimes prescribed for premature ejaculation.
One of the important things to understand about toxins is that their side effects distribute on a bell curve, which means that their most severe effects are much rarer than their moderate or minor effects. Conversely, this means that if you see very worrisome side effects from a pharmaceutical, this indicates that a much broader swath of side effects lies hidden under the surface.
Now, let’s consider the case of the COVID-19 vaccines—they have caused a large number of people to die suddenly, including young athletes, which is such a distinctive and catastrophic event that the general public is beginning to recognize it, and no amount of propaganda can close their eyes. However, the vaccinated dead are not the only victims, and Ed Dowd’s team has done a lot of work to try to quantify the magnitude of the issue our country is facing:

Note: I reviewed Ed Dowd’s report for the next article I am working on, and the saddest part about it is that I believe its estimates of the costs of the vaccine injuries were actually too conservative.
Severe Effects of SSRIs
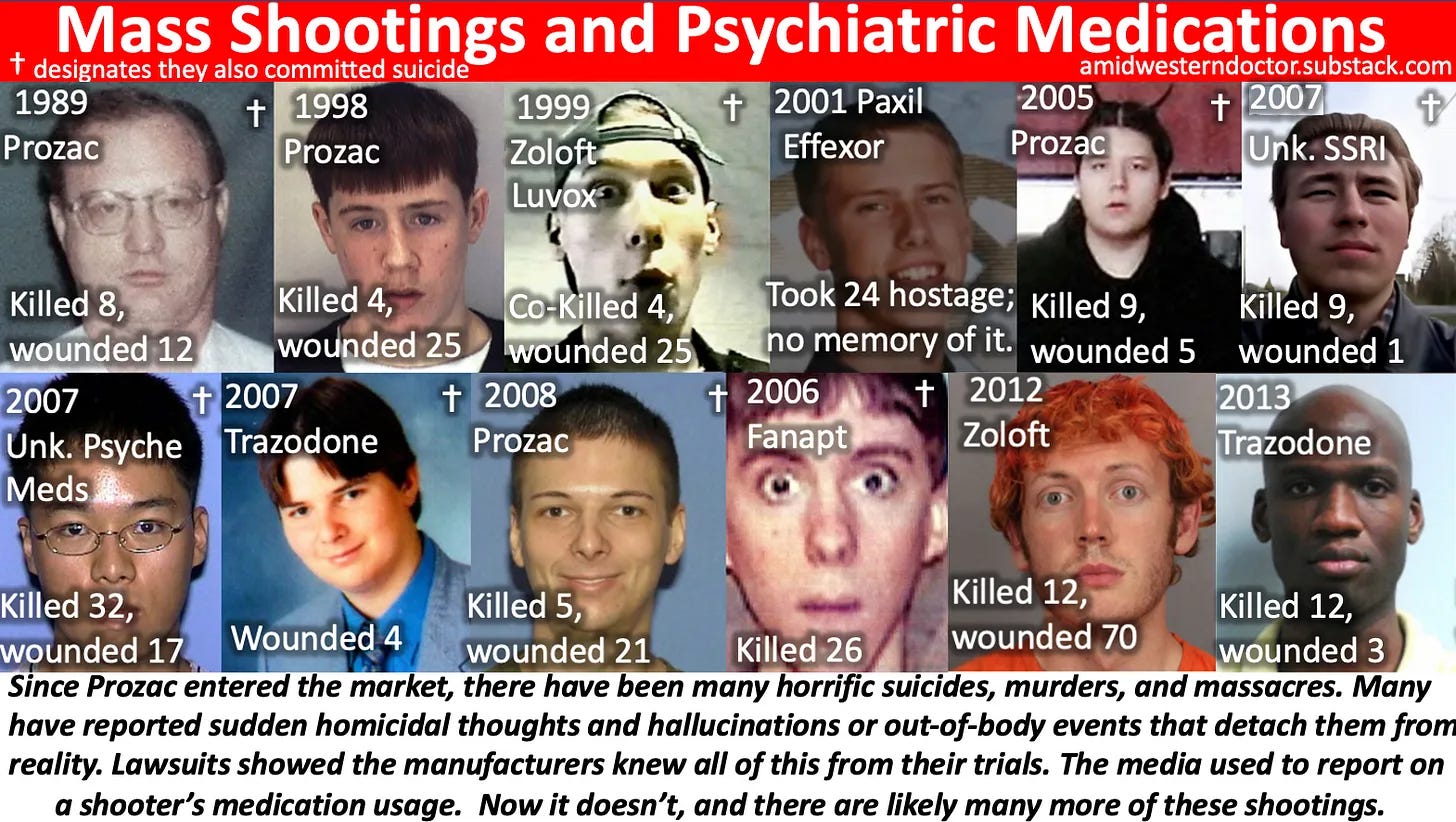
In the case of the SSRI antidepressants (henceforth SNRIs—serotonin and norepinephrine reuptake inhibitors--will also be referred to as SSRIs), they also had an unambiguous, tragic side effect. They would cause people who took them to develop violent and homicidal tendencies, which frequently resulted in suicides, or otherwise normal people committing horrific murders, at times on those closest to them. This was well known by the pharmaceutical companies, as lawsuits had forced them to reveal clinical trial data that showed that these violent tendencies had been observed in the clinical trials.
Many individuals who have committed unspeakable acts have shared similar experiences such as the following:
•Reporting out-of-body experiences where they felt as though they were observing themselves from above and did not have any control over what was happening.
•Hearing voices tell them to kill themselves or others.
•Having an immense writhing irritation within their body (known as akathisia) which they would do anything to make stop.
•Having vivid nightmares.
•Losing track of what was happening around them.
That’s pretty scary and deeply unsetting when you think about it. One of the best accounts I have heard that illustrates how all of this can happen came from a very sweet and loving child who almost became a mass shooter. In his account, he touches on many of the above points:
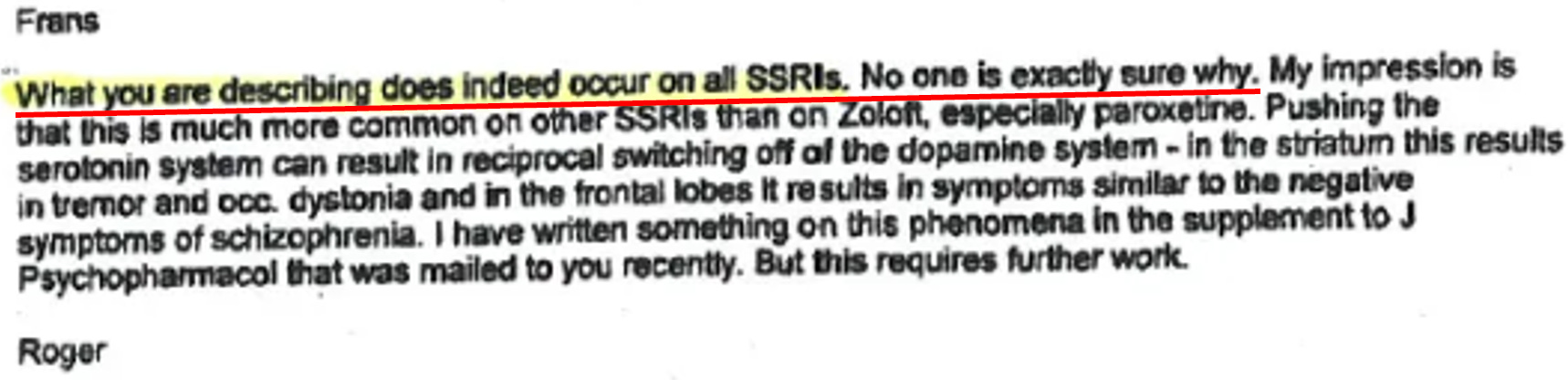
As you might suspect, we still don’t know why this happens. Consider this correspondence between a clinical investigator for Zoloft, and his contact at Pfizer:

I have often wondered exactly how common these troubling behaviors are. On a population level, there is a consistent association of SSRI usage leading to an increase in Bipolar I (which results in more aggression), which is somehow rationalized by the psychiatric profession as the pre-existing condition being unmasked by the SSRI rather than the SSRI causing it.
On an individual level, I have crossed paths with a few people who have witnessed the grisly deaths that SSRIs can cause, but relatively speaking those are just a fraction of the vaccine deaths I’ve come across. Conversely, many friends who have been on the SSRI drugs have reported some of the effects listed above, and in many cases described these experiences as if there was literally a demon trying to possess them.
The major problem with this dynamic is that while SSRI suicides and homicides are rarer than sudden COVID-19 vaccine deaths, the medical profession is in much greater denial about the SSRI casualties. As a result, when individuals on SSRIs begin exhibiting these psychotic tendencies, the most common response (besides doing nothing) is to raise the dose of their SSRI or change to another SSRI. This often has catastrophic outcomes, as the worst thing you can do with an SSRI is abruptly change the dose or change to another SSRI. Similarly, many critical warning signs are missed by responsible mental health care providers time and time again (including for many mass shooters).
One reader shared a story with me that helps to illustrate how aggressively some psychiatrists will push these drugs, even when there are many signs they are only causing harm. Sadder still, the courts (who lack any understanding of this subject except that the “psychiatrist” is an expert in the area) will typically side with the psychiatrist and forcefully medicate individuals, while their significant others do not want the drugs because they can see the harm being caused to their loved one.
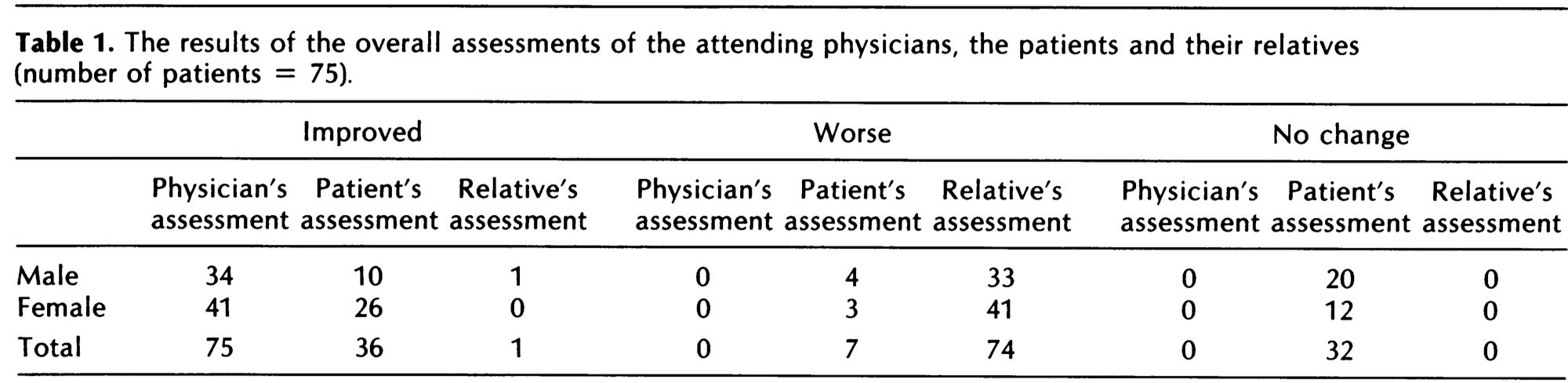
A 1982 study (which could probably never be published in today’s society) examining the effects of blood pressure drugs on a patient’s quality of life cuts to the core of this problem within medicine:
Note: although blood pressure medications can sometimes create significant issues (many observed by relatives are listed within the full study), I consider them relatively benign compared to psychiatric medications. I thus suspect that the magnitude of harm that physicians instead interpret as a benefit is even worse there.
Why Are These Drugs on the Market?
As consumer lawsuits have shown, there were a lot of really concerning data in the clinical trials for the SSRIs. Not surprisingly, the moment the SSRIs hit the market, the FDA was deluged by complaints of severe unprecedented reactions from the drugs (sound familiar?). This should raise some major questions--why on earth was nothing ever done about it at the time, and why are there now more SSRIs on the market than we can count?
Anyone who has studied the economics of the pharmaceutical industry should understand that it primarily depends upon recurring revenue from products that have a large number of customers and high sales margins. My hypothesis is that the more lucrative a drug (or drug class) is, the harder the industry will fight to protect it.
Psychiatric medications are one of the most profitable drug franchises, making approximately 40 billion dollars a year (which also includes the psychiatric medications that “treat” the complications of SSRIs). It is thus, not surprising that very powerful interests will use every tool available to them to protect this franchise, which is particularly problematic, because they provide a significant amount of the funding that the federal regulators and politicians depend upon. This issue sadly extends far beyond the FDA, as how corruption has also been institutionalized within the NIH and within the CDC.
With all this in mind, let's now examine the sad tale of how SSRIs became one of the most profitable drugs in existence.
Note: One of the best books I have found on this entire subject is Deadly Psychiatry and Organized Denial. The title is aptly named and illustrates the fact that the psychiatric field comes up with an endless list of rationalizations to dismiss the harms of their drugs, aggressively attacks anyone who claims that they exist, and continually gaslights patients who are harmed by them (often instead arguing that the harm is a sign that they are mentally ill and require the drugs). Like the first part of the series, a significant portion of this article was sourced from that book.
John Virapen
One of the pharmaceutical executives directly involved in obtaining the approval for the original SSRI antidepressant, Prozac, developed a great deal of guilt for what he was complicit in once a large number of SSRI-linked deaths occurred. John Virapen, along with Peter Rost are the only pharmaceutical executives I know of who have become whistleblowers and shared the intimate details of how these companies actually operate. Although the events Virapen alleged seem hard to believe, other whistleblowers have also made similar observations to Virapen (the accounts of the Pfizer whistleblowers can be found in this article and this article).
John Virapen chronicled the events in which he was complicit in “Side Effects: Death—Confessions of a Pharma Insider.” These included outrageous acts of bribery to get his drugs approved, and photographing physicians with prostitutes provided by Eli Lilly so that they could be blackmailed into serving Eli Lilly. For those interested, this is a brief talk that Virapen gave about his experiences. I greatly appreciate the fact he used candid language rather than euphemisms like almost everyone else does:
At the start of the saga, Lilly was in dire financial straits and the company’s survival hinged on the approval of Prozac. Prozac had initially been proposed as a treatment for weight loss (as this side effect of Prozac had been observed in treatment subjects), but Lilly subsequently concluded it would be easier to get approval for treating depression and then get a post-marketing approval for the treatment of weight loss.
As Prozac took off, it became clear that depression was a much better market, and the obesity aspect was forgotten. Lilly then used a common industry tactic and worked tirelessly to expand the definition of depression so that everyone could become eligible for the drug and aggressively marketed this need for happiness to the public, before long, transforming depression from a rare to a common condition. For those wishing to learn more, Peter Gøtzsche has extensively documented how this fraud transpired and both this brief documentary and this article show how depression became popularized in Japan so that treatments for it could be sold.
Unfortunately, while the marketing machine had no difficulties creating a demand for Prozac, the initial data made it abundantly clear that the first SSRI, Prozac, was dangerous and ineffective. Lilly settled on the strategy of obtaining regulatory approval in Sweden, and using this approval as a precedent to obtain approval in other countries. Virapen was assigned to this task and told by his superiors that if he failed, his career was over. Virapen, unfortunately, discovered that whenever he provided Lilly’s clinical trial data to experts, they had trouble believing he was actually seeking regulatory approval, as Prozac’s trial data was just that bad.
Sweden (following their regulatory procedures) elected to allow an outside independent expert to make the final determination on whether Prozac should be approved or not. The identity of this expert witness was concealed, but Virapen was able to determine that it was Anders Forsman, a forensic psychiatrist and member of the legal council on the Swedish National Board of Health. After meeting with Virapen, Forsman proposed an untraceable bribe. Then, upon receiving payment, wrote a glowing letter in support of Prozac, fully reversing his position on Prozac (he had ridiculed it two weeks before) and guided Virapen through re-writing the trial to conceal the 5 attempted (4 of which were successful) SSRI suicides in Lilly’s trial.
Forsman’s expert opinion resulted in Prozac being partially approved and formally priced for reinbursement in Sweden, which was used as a precedent to market it around the world at that same lucrative price. Virapen noted that during this time, German drug regulators who had clearly and unambiguously stated that Prozac was “totally unsuitable for the treatment of depression” suddenly reversed their position, leading Virapen to suspect that similar under-the-table activity must have occurred in Germany. David Healey, a doctor and director of the North Wales School of psychological medicine, likewise concluded that the German approval was due to “unorthodox lobbying methods exercised on independent members of the regulatory authorities.”
Not long after saving Eli Lilly, Virapen was fired. Virapen believes he was fired because he was a man of color in an otherwise Caucasian company (he was told this by his supervisor). Gøtzsche, a leading expert in pharmaceutical research fraud and meta-analyses, on the other hand, attributed this to typical organized crime tactics where Lilly sought to conceal their illegal activity by firing Virapen and his two assistants to bribe Forsman (because immediately afterwards, none of them were permitted to access their offices, and thus could not obtain any of the files that proved that this bribery occurred). Fortunately, as happened with Peter Rost, this unjust firing eventually motivated Virapen to become an invaluable whistleblower.
Research Fraud:
Both Gøtzsche and Virapen repeatedly emphasized how the trials for Prozac (and subsequent SSRIs) were deliberately designed to conceal their adverse events. Despite this fraud being clearly visible to outside investigators, it was ignored by the drug regulators (with the exception of the Germans who later capitulated to Lilly). It was also often allowed to stand in a court of law, where the purported absence of adverse events in industry trials was used to argue that there was no evidence that the alleged injuries could be linked to the SSRI (the most revolting thing is that the industry even wrote misleading manuals to help prosecutors convict peaceful people on SSRIs who committed these murders).
Over time, however, as the “inexplicable” suicides and grisly murders resulting from the influence of SSRIs mounted, courts ruled against SSRI manufacturers and forced them to reveal concealed industry documents that clearly showed significant adverse events had occurred and the same horrific events the public was witnessing had been detected in the clinical trials for their drugs. It should be noted that while these tactics were pioneered by Lilly, other SSRI manufacturers, including Pfizer, used identical approaches. The key methods were as follows:
1—Whenever severe adverse events occurred, they were relabeled with benign and innocuous terms. Forsman pioneered this approach in Prozac’s original trial, changing “Five had hallucinations and tried to commit suicide, which four of the test subjects succeeded in doing” to “Five of the other test subjects had miscellaneous effects.”
Private internal documents showed that Lilly also wanted to remove all instances of “suicide” from their database, and relabeled suicides reported by investigating doctors as “overdoses.” When independent investigators later examined UK regulator data, they found many other SSRI manufacturers had copied this terminology for concealing SSRI suicides. Likewise, private memos from Lilly revealed that Lilly instructed “suicidal ideation” to be coded as “depression.”
To further illustrate the point, a 1985 in-house analysis of placebo-controlled trials for Prozac found 12 suicide attempts on Prozac versus one each on a placebo and a tricyclic antidepressant, but after the blind was broken, six of the suicide attempts were removed from the dataset.
This tactic is commonly used in drug trials, and before COVID, I was the most familiar with this happening throughout the Gardasil vaccine trials. With the COVID vaccines, the most well-known example of this occurred with a participant in Pfizer’s trial, Maddie de Garay who developed profound permanent neurologic disability from the second vaccine, which was then coded as “functional abdominal pain.”
2—The design of SSRI trials (which utilize a lead-in period) makes it possible to deliberately exclude patients from their trials who improve during the placebo’s lead-in period (oftentimes the social support from being part of a trial is sufficient to improve depression). Worse still, it excludes patients who experience significant side effects from the drugs during the lead-in period (whereas in real life they do not get filtered and thus compromise many of the severe reactions we are told do not exist because they did not occur in the trials). This type of patient filtering is typical for SSRI trials (three-quarters of the SSRI trials have an initial placebo lead-in period of 1-2 weeks).
This is somewhat analogous to individuals with pre-existing autoimmune conditions being excluded from the COVID vaccine trials, which was critical for the vaccine approval, because between 1 in 3 to 1 in 5 of these patients appeared to have developed exacerbations of their autoimmune condition, which would have prevented the vaccines from being deemed “safe” enough to approve. However, while all of these pharmaceuticals were never tested for safety in the highest-risk groups, once they entered the market, they were immediately aggressively marketed to them.
3—Suicides that occurred outside the trial period in the placebo group were added to the adverse events experienced in the placebo trials to reduce the apparent increase in suicides in the treatment group during the trial period. Documents released through lawsuits show GlaxoSmithKline, Eli Lilly, and Pfizer engaged in this conduct. For example, David Healy noted in 2002 that, based on data he had obtained from the FDA, two suicides and three suicide attempts that were ascribed to the placebo group in a Paxil trial had occurred in the lead-in period, before the patients were randomized.
This is somewhat analogous to Pfizer’s vaccine researchers (as detailed in whistleblower reports verified by the British Medical Journal) being unblinded and selectively using PCR testing for placebo subjects (this may also explain why a much larger difference was found in the vaccine “preventing” minor COVID-related symptoms than in severe COVID complications, as the former are much easier to fabricate with PCR tests, which have a high false positive rate).
4—The specific criteria used for determining an improvement in depression was highly subjective, and it was, for this reason, that Germany originally refused to approve Prozac (similarly, have you noticed how hard it's been to pin down how the COVID-19 vaccines are supposed to benefit us?). The subjectivity of what constitutes depression has resulted in a significant discrepancy between the benefits psychiatrists perceive, and what their patients experience (as the above 1982 study shows, doctors tend to greatly overestimate the actual benefits of their drugs relative to the patient’s and their family’s experiences). Given that “mental health” is entirely in the mind of the patient, it is insidious that psychiatrists can be the arbiters of the benefits of these drugs, and we routinely see countless cases where psychiatrists are in a position of power and patients are then forcefully medicated.
To this point, Gøtzsche cites an analysis of a prescription database that showed that after only two months, 50% of the patients had stopped taking their SSRIs, which is irreconcilable with psychiatrists believing that SSRIs work in 70-80% of patients. A meta-analysis of 8 SSRI trials for depression likewise found an effect size of 0.25 was reported by observing psychiatrists, whereas no effect (effect size 0.05) was reported by patients. A Cochrane review had similar findings, with the effect size of SSRI treatment being 0.29 when evaluated by psychiatrists, and 0.06 when reported by patients. All of this is somewhat analogous to the Pfizer vaccine trial, where, as detailed by a whistleblower, participants were unblinded, and vaccine recipients were often not PCR tested once they developed COVID-related symptoms—hence leading to the vaccines performing dramatically differently from what was promised once they entered the market.
5—The most significant side effects from SSRIs arise from abruptly withdrawing from the medications. As many of the placebo participants in these trials were already on an SSRI, by placing them on a placebo, they experienced severe withdrawal symptoms (thereby making them appear to do worse than the treatment group). To be very clear—patients were deliberately harmed in these trials to make the company’s SSRI look less harmful by comparison.
Furthermore, the trials were timed to only monitor side effects from discontinuation of an SSRI for a very brief amount of time (typically a day). This resulted in many withdrawal symptoms occurring when data was no longer collected (SSRIs are known to increase the risk of suicide for weeks after withdrawal).
This is somewhat analogous to each of the COVID vaccine manufacturers terminating their long-term placebo control trials once they got an emergency use authorization (each vaccine’s EUA was originally conditional upon long-term studies of the vaccine being conducted) but because “the vaccines are so safe and effective,” it was decided it was unethical not to allow participants to receive the vaccine, and the placebo arm of the COVID vaccine trials (which could have revealed all the severe long term complications of the vaccines) was canceled. In both cases, data on the long-term consequences of the drugs can never be collected, and the “absence of that evidence” is repeatedly utilized to erroneously argue the “evidence of absence” in court.
6—Many of the activating syndromes for which SSRIs are prescribed (i.e., Bipolar Disorder, Akathisia, Suicide, and Hostile Psychosis) could be mitigated with benzodiazepines (these function as sedating agents). By incorporating benzodiazepines into the experimental design of these drug trials, it was made possible to conceal the adverse events created by the SSRIs (by one estimate 84% of SSRI trials used benzodiazepines as part of the protocol, and 3 of the 4 trials used by the FDA to approve Prozac included a benzodiazepine in the protocol). This is not known by most practicing physicians. In most cases, where these symptoms are recognized, they will be erroneously viewed as under-dosing of the SSRI, and doctors instead will simply prescribe a higher SSRI dose or a harmful antipsychotic drug.
7—SSRI suicides are always attributed to “pre-existing” depression, which is then used to argue that suicide meant that more SSRIs rather than fewer SSRIs should be given. In detailed review on the subject of depression and suicide, only 26% of those who commit suicide had been diagnosed with depression before the suicide, which makes it quite tenuous to argue that all of those deaths could have occurred from untreated depression. Similarly, to defend against all the mental illnesses which follows psychiatric medications, the profession argues that SSRIs do not cause those mental illnesses, but rather simply “unmask” ones that were already there.
All of this is analogous to COVID vaccine injuries initially being blamed on catching the COVID virus itself (I personally know of numerous cases of fatalities immediately following vaccination in a previously asymptomatic patient that were erroneously coded as COVID-19 deaths)—which is, of course, used to claim that the death could have been prevented if we had vaccinated earlier and thus we must do even more to push the vaccines on the population. Now, these effects are instead being attributed to long COVID syndrome (as the conditions are similar, and long COVID replaces the vaccine's responsibility in the illness)—in fact, one of the early ways the vaccine was marketed was to treat long COVID, which, in all but one case I have observed, the vaccine instead made worse.
One of the most common severe side effects I’ve seen from the COVID-19 vaccines (and is one of the most frequently reported causes of death in VAERS) is severe COVID-19 immediately following vaccination. Although this is understandably difficult to prove (as it could be argued that there was a coincidence, and these events instead proved a life would have been saved if they vaccinated earlier), I suspected a causal relationship was present because:
•Some of the people my friends knew which this happened to were completely healthy beforehand, and their decline from COVID-19 following vaccination was rapid.
•The Gardasil vaccine was known for doing something similar (if you had pre-existing HPV-16 or 18 infections, your risk of developing a cancerous lesion was increased by 44.6% following vaccination). As you might imagine, even though Merck’s clinical data which they sent the FDA showed this, the infection was never tested for prior to vaccination, much in the same way with COVID-19. We easily could test for the disease prior to vaccination, but almost never do, as doing so would be tacit admission the vaccine is not 100% safe and effective and thus reduce vaccination rates.
Since that time, I have come across additional things supporting this causative link. Specifically:
•I’ve encountered cases of people who had a positive PCR test (with minor symptoms) who became extremely ill with COVID following vaccination.
•I know of a case of someone who is a hermit (and only ever left his house to interact with his parents a few times a month) catching COVID immediately after visiting his parents, who had just received the vaccine.
•A few people have told me they felt a minor dormant COVID-19 infection flared and became much worse immediately after vaccination.
So given all of this, you must at this point be curious how something as shocking as the SSRIs got through the FDA.
George H.W. Bush
There is a lot of dark history to the Bush family. The Bush dynasty was founded by Prescott Bush, who built his family fortune by collaborating with the Nazis directly against the wishes of the US government (The Guardian, for example, confirms it here). His son, George H.W. Bush had the unique accomplishment of being the only CIA chief to later become president, and during his brief tenure was responsible for numerous crimes against humanity in South America. After leaving the CIA once Carter became president, Bush (senior) served as a board member for Eli Lilly. He then joined the Reagan Administration as Vice President, where he helped to push through the catastrophic decision for the FDA to approve aspartame for consumer use (aspartame was so dangerous even the FDA did not want to approve it).
After succeeding Ronald Reagan as President, Bush chose Dan Quayle as his Vice President:
In Talking Back to Prozac (1994), I pointed out that Prozac was approved under the first Bush administration and that George Bush had been a member of the board of directors of Eli Lilly, the manufacturer of Prozac. I also pointed out that Vice President Dan Quayle was from Indiana, the home state and international headquarters for Eli Lilly. At the time the FDA was approving Prozac, Quayle employed former Eli Lilly personnel on his own staff, and Quayle had considerable leverage over the FDA as the chair of a special committee that was investigating its operations. I questioned whether the FDA might have rejected Prozac and that the entire SSRI onslaught might never have gotten started if the president and vice president of the United States had not been so closely affiliated with Eli Lilly.
Bush’s son, George W. Bush likewise followed in his father’s footsteps and appointed Eli Lilly executives to senior positions within his administration. He also inserted a provision into the Patriot Act to exempt vaccine manufacturers, including Eli Lilly, from liability for thimerosal (Mercury) within vaccinations.
In summary, Bush profoundly changed the FDA’s regulatory competency. Consider this example detailed by John Virapen that occurred a few years before Bush became president. In 1980, Eli Lilly applied for the approval of benoxaprofen, and aggressively promoted this new blockbuster medication. Not long after being approved, in 1982, benoxaprofen was taken off the market after being linked to a small number of deaths, and Eli Lilly underwent a lengthy investigation conducted by the Justice Department, where it was concluded that Lilly intentionally covered up the deaths caused by their drug. Benoxaprofen is banned, but nothing has been done for the SSRIs.
Prozac and the FDA
The FDA’s treatment of SSRIs is the only instance I know of besides the COVID vaccines where the agency has not only ignored, but actively tried to conceal a horrific number of adverse events for a pharmaceutical receiving widespread protest from the public. This was most likely heavily influenced by the Bush Administration being in bed with the Eli Lilly company. As such, it is insightful to see how this has played out over decades, as we ponder how the FDA will handle the COVID vaccines and what we need to do to address this mess.
First, consider the FDA’s behavior when Bush was not yet the president:
Initially, the FDA was skeptical and noted serious flaws in Lilly’s trials. An FDA officer wrote in 1984 that patients who didn’t do well after two weeks had their blinding broken, and if they were on placebo, they were switched to fluoxetine (resulting in six weeks of fluoxetine being compared to two weeks on placebo). An FDA review also discovered that 25% of the patients had taken an additional drug, and when the FDA in 1985 removed patients on other drugs from Lilly’s trials, there was no significant effect of fluoxetine. By adding benzodiazepines, Lilly broke the rules for its trials but didn’t inform the FDA, and when the FDA later learned about it, the agency permitted it and thereby broke its own rules. The public and the doctors were never informed about this ruse.
Prozac was ultimately approved in December 1987, and as detailed in the previous section, 3 of the 4 studies that this approval was based upon, used benzodiazepines to conceal the psychotic syndromes created by the SSRI drugs.
Once Prozac entered the market in 1988, adverse event reports began to accumulate, and by 1991, Prozac had one of the highest rates of adverse events ever reported to FAERS (similar to VAERS but for other pharmaceutical injuries). As there was less regulatory capture at the time, these red flags were sufficient to convene a hearing on the SSRIs (whereas today, this still has not happened for the COVID-19 vaccines).
A hearing was convened where many witnesses told stories about out-of-character suicides and homicides. The advisory committee members, many of whom had financial ties to pharmaceutical companies producing SSRIs, ignored those reports and unanimously rejected the following proposal: “There is credible evidence to support a conclusion that antidepressant drugs cause the emergence and/or the intensification of suicidality and/or other violent behaviors.”
Note: Buying out committees is a standard industry practice (see here and here). To further illustrate the illegitimacy of these committees (who are entrusted to decide much of public policy), consider this report from Witczak:
Fast forward, after Pfizer settled the Chantix lawsuits Pfizer went to the FDA to ask to have the black box neuropsychiatric warning removed from their drug label. By this time, I was the Consumer Representative on the FDA Psychopharmacologic Drugs Advisory Committee. We were going to review Pfizer’s new EAGLE study. I was really looking forward to being part of this committee and had many questions to ask about the safety, the lawsuits, the internal company documents discovered and reviewed by experts, and most importantly, the victims. After all, Pfizer just settled the lawsuits for almost $300 million and silenced everyone. One would think the FDA committee would want to have all information including what was discovered in lawsuits involving 2700+ victims before making any decisions to remove the warnings.
A few days before the FDA Advisory Committee, I received an email from the FDA that they wanted to talk with me about the upcoming advisory committee meeting. Someone (cough Pfizer) brought it to their attention that I had an “intellectual bias” and shouldn’t serve on the committee. The roomful of FDA staffers told me that I was being recused from serving on this meeting. I told them if they think safety is an intellectual bias (or a point of view), I will always have one.
Much to their surprise, I said I would still like to address the committee and speak during the open public hearing. I ended up flying out a few days later on my own time and dime to make sure my comments and questions were asked even though they wouldn’t be part of the official public record of this meeting.
Ultimately, in an unprecedented move, the FDA removed this serious black box warning that involved violence, hallucinations, suicide, and other psychiatric side effects. To this day, this story has never really been told by the media. These side effects didn’t suddenly go away. Just the FDA black box warnings.
Lawsuits revealing private internal Lilly documents showed that Lilly had repeatedly failed to report adverse events from their SSRIs, which they were required to report. In 2004, the BMJ received a series of internal documents that showed Lilly had known since 1978 that Prozac can trigger a strange, agitated state of mind that can provoke an unstoppable urge to commit suicide or murder. Separate documents showed that Lilly initially planned to have a warning for Prozac causing psychosis in the USA package insert, but ultimately only did so in Germany, as their regulators, unlike the FDA, required Lilly to insert this warning.
Lilly also chose to commit fraud by not reporting 76 of 97 cases of suicidality from Prozac in a post-marketing surveillance study it submitted to the FDA. Cymbalta, an SNRI frequently marketed for treating chronic pain, was found by Lilly to cause severe withdrawals once discontinued in half of those who had received it for at least 8 weeks (a sad case from a reader can be found here). Lilly likewise opted not to report this to the FDA (as required by law). In the first quarter of 2012, more reports were submitted to the FDA on serious drug withdrawal effects for Cymbalta than for any other regularly monitored drug, including two opioids.
In 2003, while examining a clinical trial for giving Paxil to children, the FDA noticed that more episodes of “emotional lability” (rapid, often exaggerated changes in mood) were reported in children on Paxil than those on a placebo. The FDA decided to investigate what the actual symptom Paxil’s manufacturer was concealing behind this label, and was informed most cases referred to suicidality. One of the FDA’s safety officers, Andrew Mosholder, a child psychiatrist, further investigated this issue and concluded that 22 studies showed that children given antidepressants were nearly twice as likely to become suicidal as those given placebos.
His superiors at the FDA who had recently hidden Paxil’s tendency to cause suicidality in children predictably disputed his report, and did not allow it to be released to the public or presented at an advisory meeting. A year later in 2004, the report was leaked, and in a very telling move, the FDA chose to conduct a criminal investigation of the leak rather than address the clear safety concerns it raised.
Kim Witczak spearheaded many different initiatives against the SSRIs. For example, she filed a wrongful death, failure to warn lawsuit against Pfizer (which Pfizer responded to by sending investigators around her neighborhood to dig up dirt on her). Her lawsuit was able to obtain many crucial documents from Pfizer proving that they knew how dangerous their SSRI was (including the same out-of-body experiences which her husband had had before killing himself). Her lawsuit eventually provided the ammunition to get a black box warning (easily visible red-alerts the FDA occasionally mandates for pharmaceuticals) placed on the SSRIs. In her efforts, like the committee example above showed, she was provided with a direct view into the corruption within the FDA:
Pfizer used the FDA to intervene in Baum Hedlund’s civil lawsuits. It was discovered that Pfizer paid industry defense lawyer Dan Troy $300k for some legal work shortly before he was appointed FDA Chief Counsel by President Bush. In his new role at the FDA, Dan Troy was the mastermind behind the FDA preemption amicus “friend of the court” brief intervening on behalf of pharmaceutical companies in civil lawsuits. The brief argued that because drug was FDA approved, the lawsuits were “preempted” and should be dismissed.
The brief claimed even if a company wanted to warn consumers, the FDA wouldn’t let them update their warning label if the FDA didn’t agree. Many Zoloft suicide lawsuits were tossed out by judges who believed the FDA was final authority on the drug label. Pfizer even tried arguing the FDA preemption brief in my lawsuit. Not once, but twice. Federal Chief Justice James Rosenbaum disagreed with Pfizer and allowed my lawsuit to proceed.
We worked with NY Representative Maurice Hinchey to help expose the $300k Dan Troy received from Pfizer. Ultimately Dan Troy resigned his FDA Chief Counsel post but not before damage was done. He ultimately went back to work for private industry including becoming global Chief Counsel at GlaxoSmithKline, the maker of Paxil, another SSRI.
In 2004, likely in response to the political pressure resulting from multiple leaked reports and lawsuits, the FDA finally released a black box warning linking SSRIs to increased suicidality in children. Despite knowing about this problem long before the SSRIs came to market, it took over two decades for the FDA to provide this critical black box warning. More importantly, this only happened after massive public pressure, countless lawsuits proving these effects were deliberately concealed by the manufacturers, public hearings, and leaked reports publicly shaming the FDA.
Note: In 2006, the warning was extended to everyone under the age of 25. As this cut off was completely arbitrary, and many of the SSRI suicides occurred in much older individuals, a large press conference was organized the day beforehand so those believing it needed to be applied to all ages could have the time to speak the FDA would not permit them to have during their hearings. Although it did not convince the FDA to change course, next year in 2006, the FDA did and applied the warning to all ages groups.
By 1990, the public was demanding for the FDA to determine if SSRIs were linked to increased suicidality. As the evidence proving this was unambiguous, the FDA deliberately avoided publishing a report on this topic. Sixteen years later, shortly after the FDA was exposed for suppressing the link between suicidality in children and SSRIs, the FDA finally published a meta-analysis addressing this question. The 2006 meta-analysis encompassed 372 placebo-controlled trials of SSRIs (and related drugs) involving 100,000 patients, and showed that up to the age of 40 years of age, SSRIs increased suicidal behavior, while in older patients SSRIs decreased this risk.
A common tactic in the pharmaceutical industry is to hyper-focus on one specific set of side effects so that the other side effects can be covered up. For example, from comparing the incidences of blood clots I hear about to the percentage of people who chose the J&J vaccine, I am relatively certain that the mRNA vaccines are more likely to cause blood clots than the J&J vaccine, but whenever this topic is raised, people default to believing only J&J can cause blood clots since it was linked to a few cases of central venous thrombosis and there was a brief period where the vaccine was suspended by the FDA to assess this risk.
I suspect that the FDA’s long-delayed meta-analysis and the black box warning were a direct response to the leaked report proving an indisputable link between SSRIs and adolescent suicidality that was allowed to shield the other side effects from scrutiny. Sadly, these warnings have done very little to curb the usage of these drugs, as evidenced by how large their market has become.
The FDA’s meta-analysis almost certainly also understated the risk. As detailed throughout this article, the FDA gave the studies they analyzed a free pass on the variety of design flaws that made it easy to conceal the adverse events. In fact, the FDA had reached out to many of the SSRI manufacturers and asked the pharmaceutical company to adjudicate possibly suicide-related adverse events in their trials as they saw fit and send those results to the FDA.
When analyzing the 2006 meta-analysis, Gøtzsche found numerous other signs of deliberate fraud by the FDA (keep in mind that the goal of this study was most likely to conceal the indisputable link between SSRIs and suicide). For example, in many cases (often due to data revealed from litigation), a single study within the meta-analysis was shown to contain more cases of suicide from an SSRI than the 5 suicides the FDA cited as occurring throughout all 372 of these studies. Numerous post-marketing studies have shown that similar underreporting occurred. One analysis of prescriptions written in England when SSRIs first came to market, found that 17 suicides occurred per 10,000 prescriptions for Pfizer’s Zoloft, 24 suicides occurred per 10,000 prescriptions of Prozac, and, 27 suicides occurred per 10,000 prescriptions of Paxil.
From extensively reviewing all the data, Peter Gøtzsche, reached the overall conclusion that there are likely to have been 15 times more suicides on antidepressant drugs than reported by the FDA in its 2006 meta-analysis.
In my personal opinion, when your results are off by an order of magnitude, this can only occur through deliberate fraud. This situation is sadly analogous to the profound harm occurring from the COVID vaccines that the federal regulators and other government officials claim is rare or non-existent. Sadly, like the COVID-19 vaccines, to quote Kim Witczak, the FDA had no interest in investigating any of this:
As the head of FDA division Dr Bob Temple and Dr Tom Laughren told us in a private meeting with them, David Healy and another family, my husband was just an “anecdote“ because it didn’t happen in a double blinded placebo controlled trial [even though lawsuits later showed it did]. I kept telling them to go investigate how my husband went from not sleeping (reason for prescription) to head outside body looking in to hanging in 5 weeks with no depression or history of depression or mental health issues. It was first glimpse that FDA has no desire to investigate and also learned the same people responsible for approving drugs were also responsible for monitoring safety. Obviously, it is out of control with covid vaccines
Are SSRIs always bad?
When I write on this subject, three of the most common comments I receive are:
•I must politely disagree, SSRIs profoundly benefitted me and I never had violent thoughts.
•Thank you for writing about this, SSRIs ruined my life, and I am so happy I got off them (which was often very difficult due to their severe withdrawals).
•Thank you for writing about this; a horrific SSRI suicide or murder occurred in my close circle.
What these responses show is that there is an immense degree of variation in the responses to these drugs (something again also observed with the COVID-19 vaccines). Presently two models have been put forward to explain why individuals have such different responses to the drugs:
The first is that some individuals have a hereditary weakness in their cytochrome P450 detoxification system. As this is responsible for removing SSRIs from the bloodstream, in these individuals, normal doses of SSRIs will result in them developing elevated blood levels of the SSRI that can often be toxic and produce psychosis. Many forensic investigations have confirmed that this occurs.
The second requires you to recognize which metabolic type of depression the patient suffers from. William Walsh, Ph.D., analyzed the blood of thousands of individuals with depression and found five common distinct metabolic patterns emerged. One type, characterized by a deficit in methylation does benefit from SSRIs (and goes a long way toward explaining why some people do well on these medications). However, to quote Walsh:
More than 90% of depressives who experience symptom worsening after antidepressants exhibit a combination of high methyl and low folate levels in blood. Inexpensive lab testing can identify these persons who must avoid SSRI antidepressants. It seems likely that most school shooters had the low folate form of depression and experienced an adverse reaction to antidepressant treatment. These persons respond better to benzodiazepine medications, and also benefit from nutrient therapy to elevate folate levels. This approach is based on biochemical studies of 2,800 persons diagnosed with clinical depression.
This is a problem, because they are assumed to be safe and effective, and anything seen to the contrary is assumed to be a sign of the SSRI dose being too low or a different SSRI being needed (similarly dangerous withdrawal symptoms are never recognized). Because of this widespread denial in the psychiatric field (which is heavily invested in their drugs), these metabolic alterations are never tested for, countless avoidable tragedies occur, and the basic degree of monitoring which should happen for them, does not.
The Ideal Product
Psychiatric medications are an especially challenging area to study because they represent the ideal pharmaceutical product:
•You can diagnose virtually anyone as requiring them.
•It is very easy to emotionally market them (as modern advertising revolves around creating negative emotional states, and all of these drugs are designed to “fix“ negative emotional states).
•Once you start them, they are very difficult to ever stop taking (due to their severe withdrawals and the actual causes of depression never having been addressed).
•They often serve as a sales funnel for further psychiatric medications to treat their psychiatric side effects (such as antipsychotics for iatrogenic bipolar I disorder from SSRIs).
•They allow everyone responsible for creating a profoundly mentally unhealthy society to redirect their responsibility to pre-existing biochemical imbalances in the brain.
•New psychiatric medications are very easy to develop which ensure that patients will always be on expensive proprietary medications.
Note: Many of these points also apply to the COVID vaccinations.
This is a particularly troubling problem because one of the most common consequences of the COVID-19 lockdowns and vaccines has been mental health issues (e.g., an Israeli study found that about 26.4% of individuals with pre-existing anxiety or depression reported an exacerbation from the booster). Psychiatric medications, in turn, will almost certainly be pushed onto even more vulnerable patients as the solution for this catastrophe, rather than addressing the elephant in the room for these vaccines.
Conclusion
To conclude this series, I would like to cite a peer-reviewed Swedish study that looked at information on over 850,000 patients prescribed SSRIs within a national database of all prescribed medications, and compared the rates of violent crimes committed by these individuals when they were and were not taking an SSRI over a 3 year period. This study found that SSRIs increased the rate of violent crimes committed by 43% in those between the ages of 15 and 24 receiving the drugs.
One of the definitions of insanity is doing the same thing over and over and expecting things to change. The fact that people get up in arms about the mass shootings, but almost none of the vocal parties has been willing to propose a solution that could address this issue, in my opinion, indicates that the deaths they profess to care so much about are not a concern to them.
This same dishonesty was seen throughout COVID-19. Lockdown advocates went hysterical about their necessity to save lives (which their lockdowns did not), while simultaneously ignoring their massive costs to the population. Then during the vaccine campaign, they justified violating their fellow citizen's human rights to push the vaccines as a necessary cost for saving lives, yet when evidence showed that they were causing a massive spike in deaths, every life lost stopped mattering at all.
When I ponder how things could have gotten this way, I am reminded of a scene in Idiocracy:
The saddest thing about the SSRI saga is that as inexcusable as it was, things were much less corrupt then than they are now, especially within the federal government. At the time that the public challenged the SSRIs, the media would air stories critical of the malfeasance within the federal government and lawsuits could compel the pharmaceutical companies to disclose the harms they were hiding from the public. Now, all the vaccine manufacturers have protection from liability to prevent those lawsuits, and except for a few commentators on Fox News, no one so much as dares to question the vaccines, or any other pharmaceutical, for that matter.
One comment Kim made on our sad state of affairs really stuck with me:
Note: Renowned journalist Sharyl Atkinson has made an excellent case the prolific censorship we have become accustomed to began during the Obama presidency.
My hope is that the harm of the COVID-19 vaccines is so egregious and unambiguous, and more importantly, has affected so many people, that it will prompt enough public outcry to fix or at least improve this systemic corruption.
I thank you very much for reading this long and challenging article (especially if you shared it with anyone). Lastly, if you are considering stopping an SSRI or SNRI, do not do so without the guidance of a physician familiar with how to prevent withdrawal symptoms.
P.S I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amount of time I spend researching and writing my posts, so again, thanks. - Pierre
P.P.S. I opened a tele-health clinic with a specialized focus on the treatment of both Post-Vaccination injury and Long-Haul Covid syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.P.S. I am so very close to completing my book with the brilliant writer Jenna McCarthy. Pre-order here for:
I I as prescribed Zoloft after I told my doctor I felt anxious due to stressful events in my life and it was affecting me physically. I just wanted to feel better and wasn’t aware of the dangers. I’d hardly ever taken a drug before that. After completing a 4 question survey I got the prescription. The only follow up was every six months or so I had to see the doctor to get a refill. Same questionnaire, which was really vague and anyone wanting drugs would know how to answer it. Zoloft stopped the anxiety but drained every bit of color from my life. After several years I stopped taking it, mostly because I felt such apathy I didn’t want to bother finding a doctor to re-prescribe it. (I’d moved to a different state in the meantime.).
That was the best thing I ever did for myself. It took more than a year but the brain fog gradually left. I had been taking a very low dose, but the effects were profound. I later read of adult snd teen suicides due to this drug. I never felt that way but I can see how this drug might send someone there.
The medical profession doesn’t do enough to screen people who have situational anxiety and find drug-free alternatives.
It's disheartening to see how regulatory capture has influenced the FDA's approach to SSRIs & COVID-19 vaccines. We need transparency & accountability from those safeguarding our health. In the midst of this, alternative treatments like ivermectin have faced hurdles. Check ivermectin4sale.uk for more info & let's advocate for a balanced approach to medicine! 💊👩⚕️🙌