

The Horse Dewormer PR Campaign And My Defense Of Dr. Charles Hoffe Against The BC College of Physicians and Surgeons
The Canadian government severely restricted access to ivermectin by its citizens. Dr. Hoffe thus felt it appropriate for Canadians to obtain veterinary sources of ivermectin. I defend that view.

In my book The War on Ivermectin, Chapter 33 is titled “The Horse Dewormer PR Campaign.” In that chapter, I document the timeline and synchronized coordination between Federal public health agencies and corporate controlled media in their launch of a massive public relations campaign trying to get people and physicians to stop using ivermectin.
I maintain that the campaign was started on Aug 21, 2021 by a snarky FDA tweet aimed at all Americans (I didn’t know public health agencies were supposed to be snarky but whatever):

I will detail the timeline of the next steps of the campaign but first, I think it is important to know what triggered its launch. A week prior to the (P)FDA tweet, a report from the IQVIA National Prescription Audit Weekly (NPA Weekly) database revealed that ivermectin prescriptions were skyrocketing in the U.S:
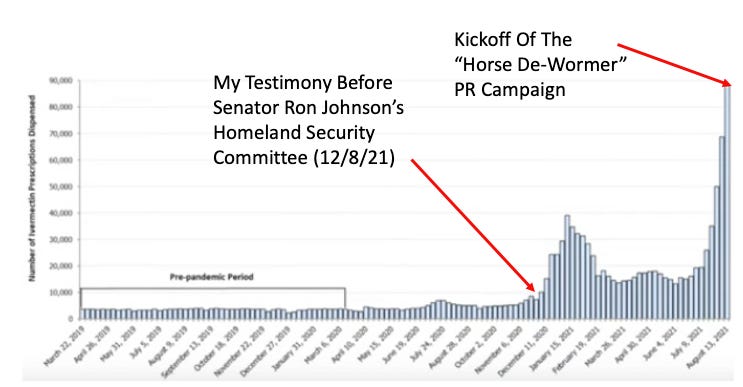
*As per this paper: Data are from the IQVIA National Prescription Audit Weekly (NPA Weekly) database. NPA Weekly collects data from a sample of approximately 48,900 US retail pharmacies, representing 92% of all retail prescription activity.
So after the FDA tweet went viral (largely because no-one had ever heard of a public health agency being snarky on Twitter before), the CDC jumped in five days later (Aug. 26, 2021) when they issued a bulletin to every State Health Department warning them of an alarming increase in overdoses and poisonings related to ivermectin. The 50 state Departments of Health then forwarded the bulletin to the inbox of every licensed doctor in the U.S within 24 hours:
Problem: the CDC bulletin was full of lies and misrepresentations as discovered by my investigative journalist colleagues Mary Beth Pfeiffer and Linda Bonvie in the below post:

Although the CDC’s mendacity rivaled the FDA’s snarkiness, neither came close to what Fauci did next. Three days after the CDC memo, he was trotted out on national TV with CNN’s Jake Tapper to discuss the topic of ivermectin. Fauci had his talking points firmly committed to memory because, if you watch the interview here (44 seconds long), he rather clumsily says essentially the same “talking point” twice as below:

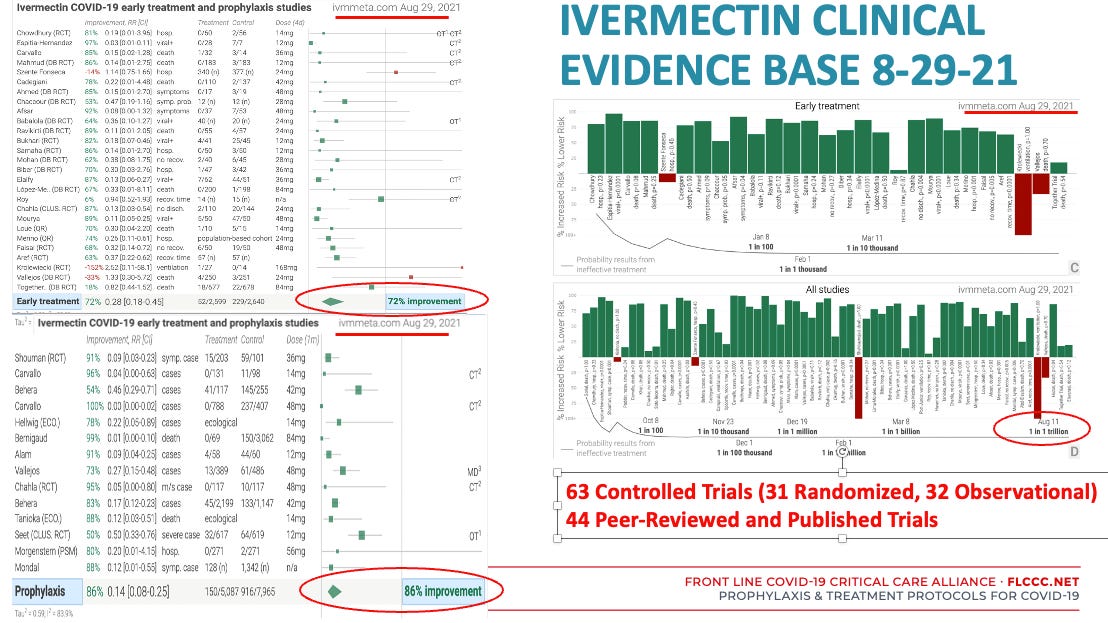
Not-so-fun-fact: the below shows the existing evidence base for ivermectin on the day Fauci went on CNN:
Then three days after Fauci’s lies on national television (isn’t it curious these first “actions” were spaced apart by three days?), three professional societies (the American Medical Association, The American Pharmacists Association, and the American Society of Hospital Pharmacists) issued a bulletin “calling for an immediate end to prescribing, dispensing, and using ivermectin to prevent or treat Covid-19 outside clinical trials.”

Wow, the health system was having a hissy fit weren’t they? Why did they never do this when oxycontin was slaying hundreds of thousands over the past decade?
Now here is where I need to introduce the massive PR firm Weber Shandwick:
Weber Shandwick, interestingly, worked simultaneously for the CDC, Pfizer, and Moderna. Thus, I maintain that, two days after the CDC memo, it was Weber Shandwick that planted an absurd and easily disprovable (and also viral) “click bait” story in Rolling Stone that many of you may remember:

Although nothing about this is funny, but you do have to laugh at the absurd images that comes to my mind as I read that headline. I am forced to picture people waiting in lines holding their hands over a gushing belly shot, blood dripping on their shoes while ivermectin overdose patients are wheeled past them in gurneys. Too funny. But it gets even funnier. This is the picture that accompanied the Rolling Stones tweet about the article:

So people are wearing winter coats and hats and shivering with arms crossed… in early September in Oklahoma? Clown world. I think Weber Shandwick needs to up their game.
Anyway, the next day the hospital where this supposedly occurred put a statement on their website that the doctor quoted in the article had not worked there for many months and that they had not had a single ivermectin overdose. Remember the line "a lie can travel halfway across the world before the truth can get its pants on?"
Despite the brazen and easily debunked story, Rolling Stone… never retracted the article. Wait what? Instead, they changed the headline to the below absurdity:

The “new” article was filled with the lies the CDC was telling the previous week about how dangerous ivermectin is (for those not in the know, ivermectin is literally one of, if not THE safest FDA approved medicine in history). Check out this table by Professor Paul Marik which I updated last week:
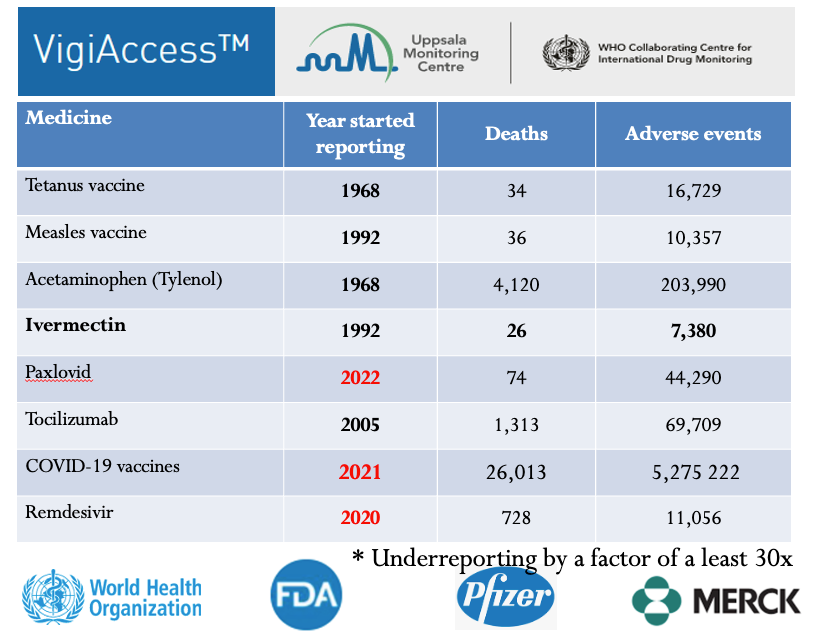
**My next post will detail the astonishing safety record of ivermectin in support of another statement that Dr. Hoffe made.
Now that “the Science” established by the CDC, (P)FDA and Dr. Fauci was so clearly established, i.e. that ivermectin was meant for horses and is ineffective and dangerous, the media went nuts. Major corporate controlled media outlets blared false and derogatory headlines for weeks, using all sources and forms of mass media. The late night talk show hosts really had a field day with endless jokes about ivermectin and the quack, fringe, anti-vax doctors and patients using it:
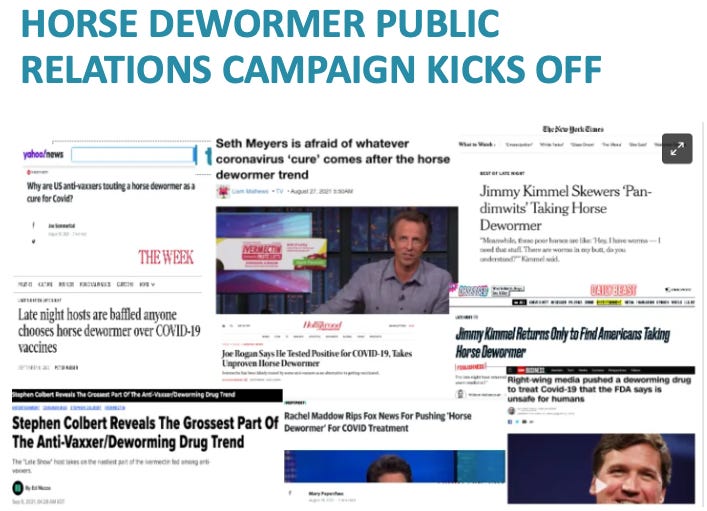
My favorite headline from the above was about how Jimmy Kimmel returned from his summer vacation “to find Americans taking horse dewormer.” Hilarious.
What wasn’t funny is that, despite him being a comedian, Joe Rogan decided to get Covid right in the middle of this hellish propaganda campaign. He then publicly mentioned in a widely circulated video that one of the numerous therapies he took was ivermectin (Hey Joe, I am proud of you and your doctor for using a combination of synergistic therapies!):

As you can see above, he then became the poster boy for the newly stoked anti-ivermectin mania. I love the phrase in the headline “unproven horse dewormer.” Redundancy has its strengths I suppose.
The CDC memo and the FDA tweet and the media blitz basically triggered a situation where many Americans were suddenly being deprived access to ivermectin. Very soon nearly every retail corporate pharmacist in the country stopped filling, and almost all the large hospital systems removed it from their formulary.
To wit, at that time I was working in the ICU at a hospital in central Wisconsin (Aspirus Wausau). Right in the middle of the PR campaign, the Chief Medical Officer came and found me and told me that the Pharmacy and Therapeutics Committee was meeting to discuss whether ivermectin should still be on the formulary. Knowing that I was literally one of the world experts in the use of ivermectin in Covid, he invited me to debate the hospital’s infectious disease pharmacist/clown at the upcoming monthly meeting.
I detailed that debate in this post below:

The short version of that debate story is that even though I felt I won the debate, the committee decided to remove ivermectin from the formulary and I was no longer able to treat my dying Covid patients in the ICU with it. Didn’t really matter because I was let go shortly after. Good times.
However, unlike in Canada, where the government and its regulatory bodies threatened punishments to the physicians and pharmacists, we in the U.S were much more fortunate for one reason: we had a system of independant compounding pharmacies which had long tired of corrupt governmental over-reach and corruption and near uniformly filled ivermectin prescriptions.
We early treatment doctors simply built lists of “safe haven” pharmacies. However, in Europe, just like in Canada, even when there were compounding pharmacies, the pharmacists did not fill. It was so bad that in Switzerland for instance, one Swiss physician told me the only way to get ivermectin was off the black market where the price for a single 12 mg tablet was as much as 50 euro. This, to me, is the most convincing evidence of ivermectin’s efficacy. Who would pay 50 euro for a tiny tablet that didn’t work?
Now, let’s get to the point of this post which is my defense of Dr. Hoffe’s statement that, because the government in Canada so severely restricted access to the medicine, he thought it reasonable to use liquid veterinary versions.
** To readers, know that I devoted an immense amount of effort in compiling this report. I plan to do the same pro-bono for any doctor who needs it, even though each case requires an independent report that takes hours. If you appreciate what I am doing for doctors, support in the form of paid subscriptions would be greatly appreciated.
DR. HOFFE’S STATEMENT REGARDING ACCESS TO IVERMECTIN:
Statement (e). In an interview presented by Quo Vadis (“QV TV”), video of which was posted online on or around October 2021, at 02:30:58 - 02:31:39, in response to the question, “what is the best approach with a doctor that is pro-vax uh, or will not prescribe ivermectin?”, Dr. Hoffe stated:
“Yeah well now, no doctors are allowed to prescribe ivermectin in BC or Alberta. If you can find somebody [inaudible] in another province, they might, but most doctors will not because they’re afraid of getting investigated by their college.” Someone in the audience asked, “how do we buy it then?”. Dr. Hoffe stated, “[inaudible] you can go to a feed store that sells stuff for livestock and tell them you’ve got a herd of sheep and you need ivermectin [laughter from the audience]. Someone from the audience stated, “that’s a serious question”. Dr. Hoffe stated, “Yeah, no, and I’m being serious. That’s a serious [inaudible] you literally, the government is forcing people to use veterinary products”.
The accuracy and soundness of Dr. Hoffe’s statement regarding access to ivermectin can only be understood in the context of the Disinformation campaign I described at the beginning of this report.
I am a physician who has treated over a 1,000 Covid patients with ivermectin since October 2020 and am regularly in communication with a network of ivermectin experts and researchers globally. I can attest that the ability of patients in many countries to access ivermectin became increasingly difficult over time.
In the United States, I observed an abrupt change in my ability to prescribe ivermectin through retail pharmacies whereby suddenly pharmacists all over the country began to refuse to fill valid prescriptions. This change was most pronounced immediately following what I call “the Horse Dewormer PR Campaign” which began in late August of 2021 (Chapter 33, the “War on Ivermectin,” Exhibit C). That sequence of actions and events led to the publication on Sept. 1, 2021 of a joint statement by the American Medical Association, the American Pharmacists Association, and the American Society of Health-System Pharmacists whereby they “strongly oppose the ordering, prescribing, or dispensing of ivermectin to prevent or treat COVID-19 outside of a clinical trial.”
Other countries and regions, like in BC and Alberta went further by threatening the licenses of physicians who prescribed ivermectin. Such actions effectively restricted the ability of acutely ill Covid patients to access what I have shown in the earlier section of this report to be a life-saving drug. Physicians who were aware of the vast extent of data proving its life-saving efficacy were thus placed put into a difficult ethical situation given that, as Dr. Hoffe correctly mentions, their governing bodies caused this “blockade” to happen.
Given that the Hippocratic Oath to which we physicians abide includes the statement, “I will do no harm or injustice to them (patients),” such a mandate left few options for an ethical physician to navigate in the situation of a restriction of access to human forms of ivermectin.
Know that Dr. Hoffe’s statement was made in October of 2021, prior to the availability of paxlovid or molnupiravir, thus it must be understood that there was no other easily accessible treatment options (i.e. monoclonal antibodies) available with demonstrated efficacy. So, a physician faced with caring for a patient with a potentially life-threatening illness without timely access to monoclonal antibodies (i.e. must be given within 5 days from first symptoms) and with the knowledge of the superiority of ivermectin’s efficacy would be left with only one option: they could simply offer supportive care only and hope deterioration and death would not occur, or they could attempt to gain access to a veterinary version of a life-saving therapy for their patient.
As a U.S citizen, I was in a much better position than Dr. Hoffe in that I found that our system of independent, small business, compounding pharmacies with rare exceptions, routinely filled my valid prescriptions.. Many of us early treatment experts began circulating lists of “safe pharmacies” that would fill our prescriptions and would not report us to regulatory bodies. Dr. Hoffe did not have that option.
In my book, The War on Ivermectin, Chapter 43, “Testimonials,” I included several testimonials sent to me of patients who rapidly recovered after taking animal versions of ivermectin, and further testimonials by family members who “snuck in” animal versions to treat patients in hospitals who also reported significant recoveries.
Further, although we know that animal sources of ivermectin are not manufactured to the same quality standard as human versions, I am aware of only a handful of reports of adverse events related to use of animal versions, and they generally involve miscalculating doses, however I am not aware of any data showing that the human version was then better tolerated. Adverse effects can happen with the human version as well.
One fact to be aware of is that the liquid formulations of animal ivermectin that Hoffe was referring to generally contain only three ingredients –1% ivermectin, 40% glycerin formal, and propylene glycol.
Glycerin formal has excellent performance and is harmless to human body and has no toxic and side effects. Propylene glycol is considered generally safe by US and European authorities. There is only one documented case of propylene glycol toxicity that was caused by excessive alcohol intake. Despite this knowledge, I agree that none of the animal products are manufactured to human standards nor are they tested in humans. Thus, there is a theoretical risk of harm to a human from using an animal product. However, I would maintain that the risk is likely a trivial one based on my knowledge of many physicians across the world who reported to me that they were forced to rely on prescribing animal versions due to lack of access to human version, and along with the many patients who reported to me that they prophylaxed with ivermectin on a weekly or biweekly basis throughout the pandemic with liquid ivermectin. I have even used it myself without incident.
Know that physicians, when making treatment decisions, must balance the risks and benefits of a particular treatment as well as a consideration of alternatives to the treatment. In the situation of having the responsibility to care for a patient with a potentially life-threatening disease, in a situation where your governmental regulatory agencies have restricted access to a very safe, life-saving treatment, I find it not only practical but admirable that a physician would attempt to guide patients with a route to accessing a medicine that could save their lives.
This is a challenging ethical situation with no easy answers. Although I am glad I personally never had to recommend someone use an animal version of ivermectin, had I been in a situation like Dr. Hoffe and other doctors that were in British Columbia, I personally would not have hesitated to recommend patients to get access to the animal version.
It is the least worst option in my opinion. I have seen too many people die or become disabled from Covid infections. I know of no deaths or disability resulting from ivermectin. I remind the reader and the College that this situation was not created by Dr. Hoffe. He simply attempted to provide the most sound guidance on how to navigate this situation. I again lay blame at the feet of the pharmaceutical industry and public health agencies and professional societies who consistently chose not to critically or expertly assess the evidence for ivermectin like I have done above. It is they who should be litigated against and punished. Not Dr. Hoffe.
P.S If you appreciate what I am doing for doctors, support in the form of paid subscriptions would be greatly appreciated (am currently in deep on another defense of a doctor being persecuted by the Washington Medical Board)..
P.P.S Our 3rd Annual FLCCC. Medical Conference is coming up! Come on down to Phoenix, I cannot tell you how not only informative they are, but also how spiritually and socially restorative as the community has some of the best people ever in it.

Gather with like-minded people from across the world, learn from leading medical experts and health freedom advocates, meet healthcare professionals, and take charge of your health and well-being!
-Also proud to report that my book has gained Best Seller status on and off in several countries and is climbing up the U.S Amazon rankings, If any of you have bought and read the book, please leave a review on Amazon? Thanks! Link:

I took ivermectin prophylactically back at the height of the pandemic, and never caught Covid, even though my vaccinated husband had it. While I no longer take it orally, ivermectin continues to play a daily role in my health. I have suffered from rosacea for years and never had any success with any of the standard treatments. Now there is a topical prescription cream called Soolantra that contains ivermectin as the active ingredient. It truly has been a game changer for me. My skin has been completely clear and free of the sores that used to haunt me. People regularly comment on how beautiful my skin is, compliments I’m not used to receiving! I give all the thanks to ivermectin and readily tell people. Ivermectin is truly a miracle drug!
My dad was hospitalized with Covid in August 2021 and was denied IVM and HCQ because the doctors insisted that there was no supporting evidence and it was not “protocol”. These doctors had a moral obligation to be current on their medical knowledge or at least intellectually open to investigating alternative treatments. Their willful blindness caused so many unnecessary deaths.