

The Existing Evidence Base For Chlorine Dioxide In Treating Human Diseases
I am interrupting my series on the persecutions of pioneers of oxidative therapies to present a comprehensive compilation of the currently published and censored evidence for chlorine dioxide.

TABLE OF CONTENTS
Barriers To Doing Clinical Research Trials With Chlorine Dioxide
What Is The Difference Between Chlorite And Chlorine Dioxide?
Evidence For Chlorine Dioxide Against Viral Infections:In-Vivo Studies
Evidence For Topical Chlorine Dioxide In Skin, Wound, And Mucosal Infections
Evidence For Orally Ingested Chlorine Dioxide In Human Illnesses
BARRIERS TO RESEARCH
I am again pointing out that my intent with these posts is to open up research into chlorine dioxide rather than recommend or promote its use at this time. To the best of my knowledge of the existing literature, this is the first review that compiled all of the peer-reviewed and published trials and studies which used chlorine dioxide in treatment, and at the end, I also review the retracted and/or censored studies that have been done to date.
Currently, it is extremely difficult, if not impossible, to rigorously assess the efficacy of widely available, orally ingestable forms of chlorine dioxide in our modern scientific climate. However, no restrictions have been placed on doing studies of its equivalent, chlorite, which has patented formulations which have been studied within numerous double-blind RCT’s as you will see below).
This uncomfortable fact is due to the globally coordinated barriers to both performing and publishing research of its efficacy in treating human diseases. I believe that in my last two posts of a historical account by a retired translational scientist that had high level security clearances in the latter half of the 20th century (here and here), the reasons for that should now be obvious.
If you didn’t read those posts, I will spell it out for you, again. The barriers are due to chlorine dioxide’s threat to the massive markets of modern pharmaceutical products.
To wit, when the topic of oral ingestion of chlorine dioxide is addressed, numerous copycat bulletins are posted by regulatory agencies such as the FDA, TGA, , PAHO/WHO, SWISSMEDIC and other health authorities that advise against its use by falsely alleging that it is toxic and/or dangerous to ingest, describing it as "bleach," "bleach-like," or a "poison." See examples of the coordinated fear-mongering:

I won’t deny the fact that it can be used as a bleaching agent in industrial applications at 5000 mg/L, however the oral doses used therapeutically (160mg/L) fall far lower than the minimal level (210mg/L) that has been determined by the EPA to cause an adverse effect (I extensively detailed its safety in this prior post). As a result, for decades, millions around the world have used it safely (and discreetly) to treat illnesses via topical, oral, and even intravenous administration. Regulatory agencies around the world all willfully deny this reality.
That is, until the revolutionary passing of a law in Bolivia in 2020, allowing for the widespread manufacture and distribution of oral chlorine dioxide solution to treat Covid. In my first post on chlorine dioxide, I provided an enormous amount of documentation that Bolivian military forces and universities, right after the law was passed, began manufacturing and distributing it to Bolivians. This program led to Bolivia having the best outcomes in all of South America despite the strenuous objections in media interviews and press releases by their health ministry). Power to the people.
To give another real-world example of the impacts of regulatory agency behavior towards chlorine dioxide, in this peer-reviewed and published study, "Determination of the Efficacy of Oral Chlorine Dioxide in the Treatment of COVID-19," the authors reported that they could only recruit 40 patients into their trial due to the following reasons:
“The same protocol was presented in eleven American countries and in Spain for approval. Unfortunately, drug control entities in all countries generated warnings and even bans on its use for human consumption that made it difficult for ethics committees to approve the protocol. Although a multi-country, multi-center study was planned, numerous ethics committees from other countries denied approval for patients there to participate.”
Further, for those who have read my previous posts on chlorine dioxide, you should now be aware of the history of those who tried to promote, research, or treat patients with orally ingested oxidative therapies like chlorine dioxide or Homozon. Their efforts led to repeated deportations, imprisonments, and assassinations (some of which you have yet to learn about as they will be detailed in upcoming posts on the plight of more modern practitioners). If you are interested to learn about them as well, please subscribe.
Beyond the regulatory agency barriers, chlorine dioxide research also gets suppressed by medical journals that are captained by what my highly published friend and colleague, Dr. Flavio Cadegiani, calls “The Editorial Mafia.” See my prior post where I provided extensive evidence of the obstructionist behaviors by the highest impact journals in regards to Flavio’s high-quality trials of proxalutamide during Covid. In that same vein, I will detail below a number of chlorine dioxide studies that have been retracted and/or “scrubbed” from the internet.
In addition, strongly worded editorials have been published in journals which repeatedly and aggressively amplify health agency warnings against the use of oral chlorine dioxide, such as in this review published in the journal Cureus in 2022:

The war on safe, cheap, repurposed therapies has no bounds.
WHAT IS THE DIFFERENCE BETWEEN CHLORITE AND CHLORINE DIOXIDE?
In the below, I will argue that clinically and physiologically, there is no difference at all.
In my research group on chlorine dioxide, the one advanced applied chemist, Tom Henshaw, maintains that, chemically, most ingested chlorine dioxide is rapidly converted into chlorite (a weaker and slower oxidizing agent) and it is largely chlorite that gets absorbed into the human body and subsequently excreted.
Recall that chlorite is chlorine dioxide’s pre-cursor as well as its main metabolite (they switch back and forth depending on pH level and the presence of reducing agents). Recall that it was just oral sodium chlorite drops that were given to Jim Humble and which he used to treat his first two malaria patients back in 1996.
Further, the CDC published a review of chlorine dioxide’s safety in water purification which was titled “Toxicological Profile Of Chlorine Dioxide And Chlorite.” Throughout the document their equivalency was clear given chlorine dioxide, as they stated “rapidly turns into chlorite after entering the human body via drinking water.”
The two hypotheses we have about chlorite is that either;
1) chlorite is actually the therapeutically active agent rather than chlorine dioxide or,
2) chlorite, when entering into or exposed to acidic micro-environments in the body (such as in areas of ischemia, cancer, infection, or inflammation), gets “re-converted” into chlorine dioxide and that is where “the magic happens.”
To reconcile the two hypotheses would require sophisticated analytic equipment with precise physiologic sampling of fluids and tissues. To my knowledge, no such study is happening or has happened. However, I maintain that, based on the above, and until it can be definitively answered, the efficacy of chlorite should be considered equivalent to chlorine dioxide and vice versa.
Here I must give a huge amount of credit to my Spanish colleague Jorge Gaupp and his team that “discovered” an evidence base of chlorite studies which used intravenous formulations in numerous randomized, double-blind, placebo controlled trials that were published in the peer-reviewed literature.
In the conclusion of the above review of the literature by Gaupp et al, they write:
After reviewing all published information to date, we conclude that:
a) although there is a lack of published clinical trials using chlorine dioxide, other chlorite publications should be considered to be studying chlorine dioxide, and vice versa;
b) conducting additional preclinical studies with chlorine dioxide will complement previous chlorite studies;
c) although chlorite treatments via oral administration have recently been prohibited due to uncontrolled self-medication, supervised controlled doses of oral and intravenous chlorite have been shown to be beneficial in a wide variety of published clinical trials in humans.
Shocker: to date, they have not been able to publish their review (likely because of the sentences bolded above).
It should come as no surprise that I believe the reason why there is robust evidence for chlorite is that pharmaceutical companies have patented two intravenous formulations of it and have named the compounds WF10 and NPOO1. By doing this, it allowed them to sail through research ethics committees (IRB), regulatory agencies, and “Editorial Mafia” barriers. Nice trick. But we busted you. What a world.
Recent text from Jorge Gaupp to the chlorine dioxide research group I am a part of:
“I live in Spain, here we presented a clinical trial with chlorine dioxide solution for approval and it was rejected. It happened the same to other colleagues. Spanish drug administration is impossible”
Gaupp et al. discovered that WF10 and NP001 trials have been done in diseases such as advanced AIDS, ALS, radiation cystitis, and diabetic wounds. However, in not one of those ALS publications does the word “chlorine dioxide” appear (except in one paper where it appears in the title of two citations in the bibliography). Hmm.
I will cover the trials in ALS below, but, spoiler alert, the company that owns the patented chlorite formulation NPOO1 (Neuvivo) just applied for FDA approval for its use in ALS. Check out this article summarizing the findings from the trials published in the best selling newsletter called “ALS News Today” just 6 weeks ago:

Further, in this transcript of an interview with NPR, the interviewer and the investigator share that the company is ready to initiate Phase II studies of chlorite in Huntington's, Alzheimer's disease, Parkinsons, muscular dystrophy, frontotemporal dementia, and vascular dementia.
Whoa. Chlorine dioxide (err, I mean chlorite) is entering our therapeutic armentarium! Albeit and unsurprisingly, likely at great cost and complexity (i.e requiring IV administration, physician prescription, and administration). Still, cool stuff.
But imagine if the knowledge got out that you could take chlorine dioxide/chlorite orally at home and at the onset of illness instead? (I trust that Neuvivo will not come after me for that statement - again reminding everyone I am not suicidal. Am not so worried because Neuvivo, for now, is “small Pharma,” not “Big Pharma” (revenue was just $697,000 last year).
EVIDENCE FOR THE EFFICACY OF INTRAVENOUS CHLORITE FORMULATIONS
ADVANCED AIDS
Back in 1998, in a double-blind trial, 10 patients received IV chlorite (WF10) in cycles over 3 months and were compared to 9 control patients. Check it out: in the treated patients, all white cells and lymphocytes increased while all values continued to decrease in the control group. No treated patient ever got hospitalized and none got PCP pneumonia while 5 controls were hospitalized and 4 got PCP pneumonia. Finally, and most importantly, over a 9 month follow-up, six of the control group patients died while only one treated patient died.
RADIATION CYSTITIS
In 2004, a multi-center two-arm open label trial included 100 women with cervical cancer who were suffering late hemorrhagic radiation cystitis (i.e. bleeding bladders). WF10 was infused for 5 days in a row every 3 weeks for 2 cycles. Complete resolution was achieved in 74% of treated patients vs 64% of controls. Although that outcome was not statistically significant, 77% of controls experienced a recurrence compared to 47% of treated patients (p=.01). This also led to significantly less use of antibiotics as well as antispasmodics. Nice result but, again, I would have given them daily oral chlorine dioxide instead :).
RADIATION MUCOSITIS
One study included 13 patients with head and neck cancer that had suffered oro-pharyngeal complications of radiation (a nasty and unfortunate complication which often leads to the inability to eat, swallow or talk and thus sometimes requires placement of a feeding tube). They found that WF10 led to statistically significant reductions in radiation mucositis and swallowing difficulty in the treated patients.
AMYOTROPHIC LATERAL SCLEROSIS
Know that one of the main reasons they studied chlorite in ALS is because ALS disease progression is associated with activation of two different subtypes of monocyte/macrophages (immune cells which cause inflammation) and which chlorite/chlorine dioxide strongly inhibits.
2014 - Phase 1 trial of different IV doses of NP001 chlorite found that up to 3.2mg/kg was safe and that it led to a significant reductions in one type of monocyte in peripheral blood at all doses used and after only a single infusion. Further they found that the higher the monocyte activation, the greater the response. In the other subtype of monocyte, there was again a dose dependent effect - higher the dose, the greater the decrease.
2015 - Phase II randomized, double-blind, placebo controlled trial of NP001 (chlorite) given IV. They enrolled 136 patients with ALS <3 years. The patients were given 2mg/kg, which for a 70 kg male, would equate to 140 mg dose which is about the daily total dose of oral chlorine dioxide that is used in popular therapeutic regimens (however IV bioavailability is much higher, I am pointing this out to again establish how safe oral dosing is). Further, in this trial they give it in a single infusion instead of breaking it up into smaller doses taken frequently throughout the day as is typically done in oral dosing protocols with MMS or CDS (the two most popular chlorine dioxide formulations).
Although, “no significant slowing or decline” was observed, in a separate planned post-hoc subgroup analysis of the study published here, they found that in the patients with greater inflammation:
More than 2 times as many patients on high-dose NP001 (25%) did not progress during 6 months of treatment compared with those on placebo (11%). The arresting of progression of ALS symptoms by NP001 in a subset of patients with marked neuroinflammation, as observed here, will represent a novel therapeutic approach for patients with ALS, if confirmed.
2024 - A retrospective observational controlled trial of 268 patients who had participated in the 1mg/kg or 2mg/kg treatment trials of NP001 and who had “received at least one dose,” something which is called an “intention to treat analyses.” Meaning, they did not just include patients who had completed the trials but the larger number who had simply started it. The median overall survival (OS) was 4.8 months longer in the treated group. Among patients aged ≤ 65 years, the median OS for the 2 mg/kg NP001 group was 3.3 years vs. 2.4 years in the placebo group). No differences were observed in the 1 mg/kg NP001 group or in patients aged > 65 years. So at higher doses and in younger patients, they survived a year longer. In ALS? Wow.
EVIDENCE FOR CHLORITE IN NON-HEALING DIABETIC WOUNDS
In a randomized, double blind, controlled trial of 38 patients with “therapeutically resistant wounds” that the majority of patients had for over a year, they found that:
“The differences in therapeutic efficiency were so large that, in spite of the relatively small patient samples (21 vs. 17) it was possible to verify the superiority of a method for wound treatment in a randomized double blind clinical trial.”
In this case series, 12 patients with severe ulcers complicated by gangrenous toes and osteomyelitis were treated with WF10. Eight had been referred for below the knee amputation. None of the individuals ended up requiring amputation. 8 of the 12 patients achieved “complete healing” and 3 more achieved “significant improvement.”
Further, WF10 gradually reduced the HbA1c ( a marker of severity of diabetes) values from a high-risk range (9.1 ± 1.6%) into a low-risk range in all patients but one. The values remained low over at least 8 to 12 weeks after the administration of WF10. So, it cures diabetes too?
In this double blind placebo controlled RCT, the treated patients received IV infusions of WF10. After 9 weeks, treated patients had statistically significant reductions in wound severity scores, infection, inflammation, and necrotic tissue with increases in granulation tissue observed.
In a controlled trial of 29 patients with poorly healing wounds, TCDO (i.e. WF10) impregnated dressings led to less purulence with more granulation and epithelialization (skin covering).
In this prospective, open-label trial of 129 patients with diabetic foot ulcers (DFU) that included patients that had neuropathic, ischemic, or severely infected DFU’s, all neuropathic ulcers achieved either a good or fair outcome (81% good outcome), as did 49% and 81% of ischemic and severely infected ulcers respectively. Minor amputations were necessary for 14 patients (11%), but no major amputation was required. One hundred and one patients (78 %) received only 1 cycle of WF10.
In this prospective, interventional, pretest-posttest study, 40 DFU patients with HbA1c > 8.5 % were treated with standard therapy plus five weekly infusions of the chlorite-based drug WF10. In 38 treated patients WF10 decreased the HbA1c value from 10.48 at baseline to 8.06 at Week 8 and the Wound Severity Score went from 8.0 to 1.4 (both p < 0.0001) at Week 12. No serious side effect of WF10 was observed.
Conclusion:

EEVIDENCE FOR CHLORINE DIOXIDE AS A BROAD ANTI-MICROBIAL
OK, now, lets switch to studies of chlorine dioxide. The list of organisms susceptible to killing by chlorine dioxide outside the body include the near entirety of pathogenic (i.e. “disease causing”) viruses, bacteria, fungi and parasites.
In-Vitro Studies
Below is a lengthy albeit incomplete list of the many studies demonstrating in vitro (in a test-tube) and/or in-vivo (in animals) efficacy against a wide variety of viruses and bacteria and fungi. For those of you in the vaccine industry, note the studies of its efficacy against polio, HPV, flu, measles, Herpes, and HepB (Yes, I went there folks:).
Typhoid, Norovirus, Hepatitis C, Hepatitis B, HPV, HIV, Herpes, Measles,Influenza A Virus, E.Coli, Listeria, Rotavirus, Mycobacterium Avium, Hepatitis A Virus, staph aureus, and hospital pathogens like Acinetobacter baumannii, Escherichia coli, Enterococcus faecalis, Mycobacterium smegmatis, and Staphylococcus aureus.
This article from a military journal describes how chlorine dioxide even kills Ebola.
The EPA spent $27 million disinfecting the Senate buildings after the 2001 Anthrax scare… using chlorine dioxide.
One company restored an entire restaurant infested with mold after Hurricane Katrina by fumigating it with chlorine dioxide.
In this 2010 study, concentrations ranging from 1 to 100 ppm inactivated ≥ 99.9% of 8 different viruses with a 15 sec treatment. The antiviral activity of chlorine dioxide was approximately 10 times higher than that of “sodium hypochlorite,” (standard bleach.)
To wit, in this study of its anti-microbial efficacy, they call it “the ideal biocide,” openly investigating why “the solution that kills microbes rapidly does not cause any harm to humans or to animals.” Further, from their conclusion:
“bacteria are not able to develop resistance against chlorine dioxide as it reacts with biological thiols which play a vital role in all living organisms.” Whoa.
This fact supports the assertion made in my prior post by the famous Soviet defector and bioweaponeer, Vladmir Pasechnik, who, in 1985, reportedly claimed that chlorine dioxide was “the ultimate antidote to all bioweapons.”
However, “some” resistance (thus likely requiring higher doses) has been found with cryptosporidium oocysts, some mycobacteria, and some non-enveloped viruses like norovirus and certain enteroviruses.
Know that our native microbiome should be largely unaffected by weaker oxidizing agents like chlorine dioxide because our native bacteria secrete lots of “protectants,” i.e. enzymes which neutralize reactive oxygen species before they can start destructive chain reactions as well as anti-oxidants which scavenge the free radicals generated. They also produce “reducing agents” within the cell like NADPH.
Despite this assertion, the effects of chlorine dioxide on the microbiome in humans has not been well studied (which is a central point of this series in that I am trying to open up research into the compound).
On that point, although dysbiosis from chlorine dioxide has been found to occur in quails and rats at comparatively higher doses than is used in humans, one study in mice reported minimal effects. My take is that any negative effects are dose dependent. I would counter concerns that these studies raise with the knowledge that many patients with gastrointestinal illnesses (Crohn’s, Ulcerative colitis and the like) have reported profound benefits and recoveries with the use of chlorine dioxide.
Evidence For Chlorine Dioxide Against Viral Infections: In-Vivo Studies
I thought I would include a few in-vivo studies as they are surprisingly few. In-vivo studies can be but are not always predictive of efficacy in humans.
A randomized controlled trial from 2008 found that sixteen days after contracting Influenza A, 70% of control mice died compared to 0% of those treated with chlorine dioxide gas.
In this mouse study, chlorine dioxide gas killed almost all of the bacteria and fungi present while no damage to lung cells, eyes, or other organs was observed.
Know that mastitis (breast infection) is a major problem for dairy cow farmers and in this study, their “teats” (equivalent to our nipples) were dipped into chlorine dioxide to prevent mastitis. They found chlorine dioxide led to a reduced incidence of staph. aureus infection of the udder by over 90%.
EVIDENCE FOR TOPICAL CHLORINE DIOXIDE AGAINST SKIN, WOUND, AND MUCOSAL APPLICATIONS
The most robust published evidence base for chlorine dioxide is for mucosal, skin, and wound applications. The evidence for the efficacy of oral ingestion on other diseases will follow this section.
This should not be surprising given the above results of the intravenous chlorite trials above but also given the numerous products for topical and oral application that are out there, with the most studied and developed being those from Frontier Pharma here (I have no financial conflicts of interest with them but I have to say I have used their products regularly). The acne spray (my teenage daughters love that one), the nasal/sinus spray, and the toothpaste are musts for every medicine cabinet IMO.
Super fun fact: I was “literally” (my teenage daughters favorite word) at the dentist yesterday for a teeth cleaning and she started by taking a sample of matter from between my teeth and below my gums. She then smeared it on a slide and placed it under a microscope which was projected onto a screen on the wall in front of me. As she and I surveyed the slide, she pointed out all the “good” and “bad” bacteria that were there (most were “good”). However, she kept pausing and saying, “normally the bacteria should be moving, yet I cant see any of them moving.” I “literally” had brushed my teeth with Frontier’s chorine dioxide toothpaste right before going there :). When I told her that she said, “What is chlorine dioxide?” I answered that it was a broad spectrum biocide and she said, “Well, I need to look into that and I would like to know which product because I will have to recommend it to some of my patients.” Too funny.
PERI-ORAL AND GENITAL HERPES
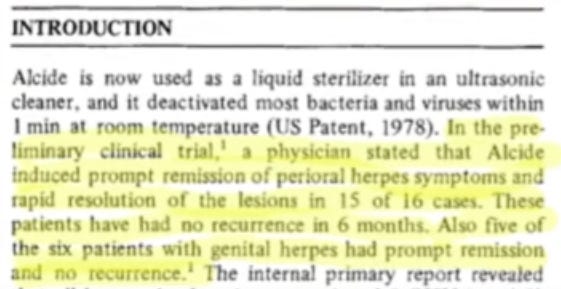
Chlorine dioxide induces prompt remission of both peri-oral and genital herpes:
“Alcide (a patented form of chlorine dioxide) induced prompt remission of peri-oral herpes symptoms and rapid resolution of the lesions in 15 of 16 cases. These patients have had no recurrence in 6 months. Also five of the six patients with genital herpes had prompt remission and no recurrence." Reference: A. R. Shalita, Internal report from Department of Medicine, Division of Dermatology, Downstate Medical Center, State University of New York, May 1, 1979.)
ATROPHIC CANDIDIASIS
In 2004, Mohammed et al performed an open-label study of 30 patients with chronic atrophic candidiasis. Patients rinsed with 0.8% ClO2 mouth rinse (DioxiDent) twice daily for one minute and soaked their dentures overnight in ClO2 for 10 days. They found a significant improvement in clinical appearance (p < 0.001), microbial count (p < 0.001) and the mean clinical score decreased from 2.50 at baseline to 0.17.
HALITOSIS
Two separate meta-analysis of RCTs concluded that daily use of chlorine dioxide mouthwash significantly improved oral malodor parameters without known side effects
ORAL HYGIENE
A systematic review found it effective in reducing plaque and gingival indices.
SINUSITIS
Sinox Pharma conducted a study where patients with mild to severe sinusitis were treated with thee strengths of chlorine dioxide nasal sprays ranging from 3-8ppm, 20-30ppm and 50-75ppm).
All 4 patients with “mild” sinusitis symptoms saw improvement to “none” symptoms.
9 patients with “moderate” sinusitis symptoms saw improvement to “none” (6) or “mild” (3) symptoms.
Of 3 patients with “severe” sinusitis symptoms, 2 saw improvement.
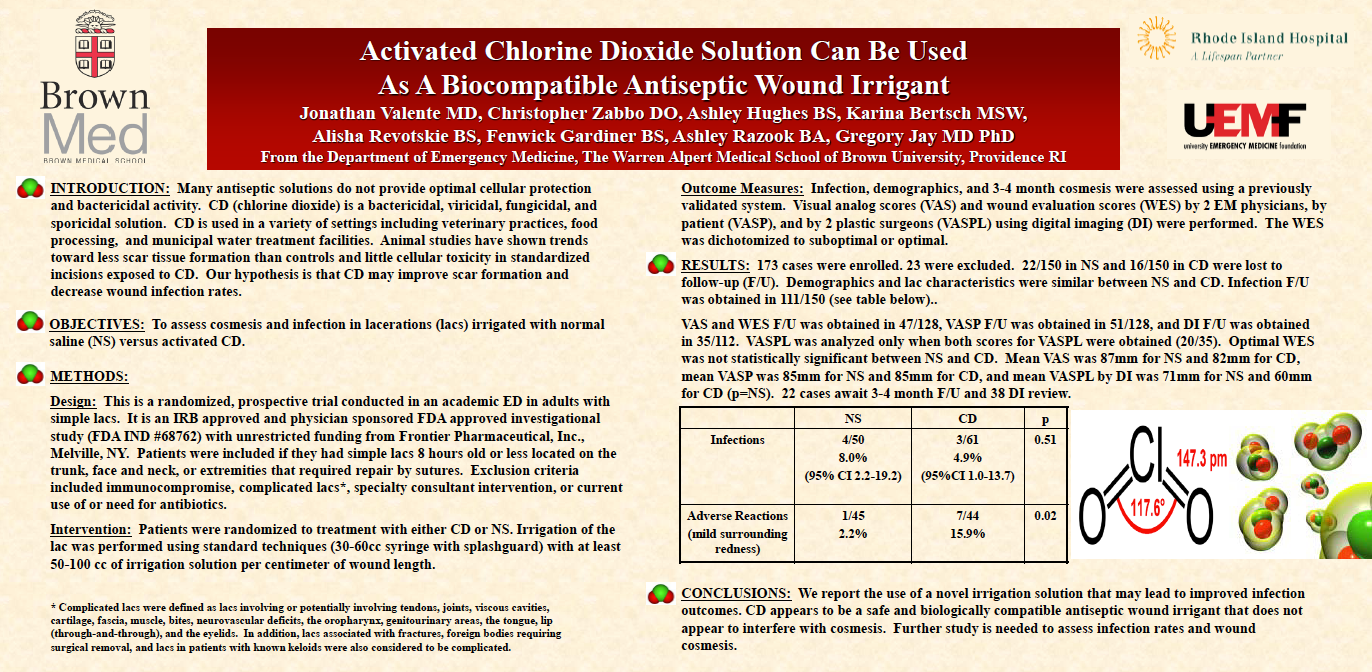
WOUND IRRIGATION AND HEALING
Chlorine dioxide is also recognized as a biocompatible wound antiseptic irrigant. This means that it can be used in human and animal wounds to help reduce infection and inflammation without causing any type of irritation or negative effects on routine healing.
In fact, chlorine dioxide products have been shown to significantly improve wound healing time with safety and biocompatibility in animals. Improvement in wound healing outcomes have been found in humans, rats, dogs, and guinea pigs.
In this paper, they review chlorine dioxide’s critical mechanisms for improving wound healing such as reducing hyperglycemia, decreasing oxidative stress, improving vasculopathy, slowing the progression of neuropathy, decreasing inflammation, killing pathogens and improving wound healing.
Know that existing treatments for diabetic foot ulcers are only partially effective and when these ulcers do not heal, amputation of the affected limb may result. From the above paper, they provide references that estimate that an amputation due to diabetic foot infection occurs somewhere in the world every 30 seconds. Mortality rates following amputation are abysmal with approximately 20% of amputees dying within the first year after surgery, 40% by 3 years, and 60-70% within 5 years. This mortality rate is equivalent to or worse than the mortality rates for breast, colon, and prostate cancer.
In the below case series by my colleague Dr. Patricia Callesperis, the following results were obtained, which, in my mind, are absolutely impressive (and it should go without saying that “bleach” wouldn’t do this). See embedded PDF if interested because the website link for the journal article does not work at the moment (accident?)
In the first case below, the patient was treated with orally ingested chlorine dioxide solution (CDS), (10ml every hour for ten hours a day) as well as a daily dressing soaked in chlorine dioxide solution and…DMSO (AMD would be proud).

In the 2nd case below, the patient was only treated with orally ingested chlorine dioxide solution (10ml every hour for 6 hours a day).

In the 3rd patient below, despite multiple courses of intravenous antibiotics and topical treatments, the wound progressively worsened. Topical chlorine dioxide gel (Ciderm Gel by our friends at Frontier Pharmaceutical) was then applied. The wound became purulent for 1 week. Subsequently, the infection was eradicated and the progression of the tissue destruction stopped. Over the next three weeks, debridements were continued and there was no further progression of the ulcer, which began to granulate. The patient was released from the hospital and his ulcer continued to heal as shown below.

FOURNIERS GANGRENE
See below for photographic examples of another case of remarkable healing observed with daily chlorine dioxide ingestion and topical application. This case has not yet been published but comes to me from Dr. Patricia Callisperis who authored the paper on the three diabetic wounds above. First know that Fournier’s gangrene is a rapidly progressing, tissue-destroying infection affecting the genitals and nearby areas. It is a life-threatening condition with a mortality of between 20-40% with one series finding 88% mortality. This was the original presentation:

Now see the progression throughout treatment, the last picture on the bottom right is evidence of a truly remarkable result for such a deadly disease:

TRAUMATIC WOUNDS
Requires no explanation:


There is also this abstract below, presented at a scientific conference which showed modest, non-statistically significant improvements when chlorine dioxide was used (I am trying to be comprehensive with presenting all the published evidence because, overall, as I have alluded to in prior posts, it is difficult to find published research on chlorine dioxide, with that difficulty being much more directed toward studies of oral ingestion).
BURNS
In the below pdf is a burn wound study called “Studies of Infection and Microbiological Surveillance of Troops With Thermal Injury - Topical Use of Sodium Chlorite-Lactic Acid Gel in Pseudomonas Burn Wound Sepsis.” The study was performed in 1980 at the US Army Institute of Surgical Research, using a precursor chlorine dioxide Gel formula made by Howard Alliger while at Alcide, Corp. From the study discussion – “Surprisingly, sodium chlorite-lactic acid gel gave excellent results with only one treatment (rather than 10) and with one days’ delay.”
IDIOPATHIC ORAL ULCERS
Personal experience of Dr.Patricia Callesperis:
“I used to have these lesions in my mouth every month or every couple of months. That type of lesion would appear repeatedly. I received treatment from various doctors, and I even traveled to the United States to a center because they told me it could be lichen planus, coxsackie, a herpes mutation, and so on. I received many diagnoses, but nothing improved. I used balsiclovir, I tried many vitamins to boost my immunity.

They wanted to perform a biopsy, and that’s when I discovered chlorine dioxide. I started taking chlorine dioxide and since then, I’ve never had those lesions again. I’ve been able to practice my profession normally and perform surgeries because the lesions even started appearing on my fingers, preventing me from operating. Now, I’m fine.”
Based on that experience, she became professionally dedicated to researching and promoting the use of chlorine dioxide as an alternative therapy. As a result, I am gratefully indebted to her for all of her guidance and knowledge around chlorine dioxide that she has shared with me.
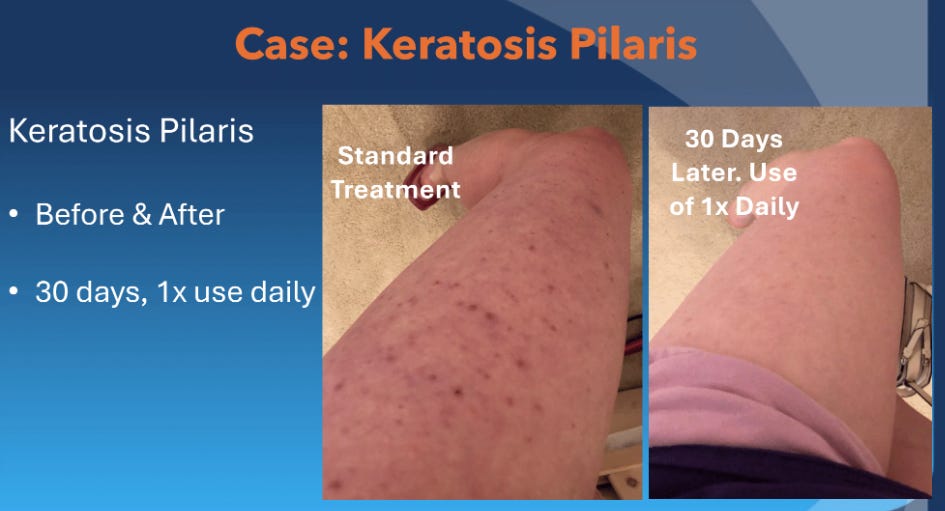
KETOSIS PILARIS
KP is a skin condition that results from a buildup of keratin, a hair protein, in the pores. This blocks hair follicles, forming small bumps over where hair should grow. Nothing works very well, given that existing therapies are either too irritating, too expensive, take too long or are too difficult to comply with as they smell or feel weird. In this case series, they reported:
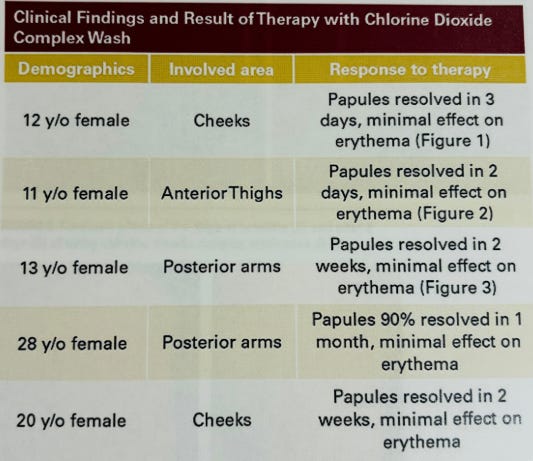
Here is one photo example:
DERMATOLOGIC APPLICATIONS
Dr. Jill Fechtel is a dermatologist that gave a lecture last year where she highlighted the numerous uses for Frontier’s chlorine dioxide products:
ACNE

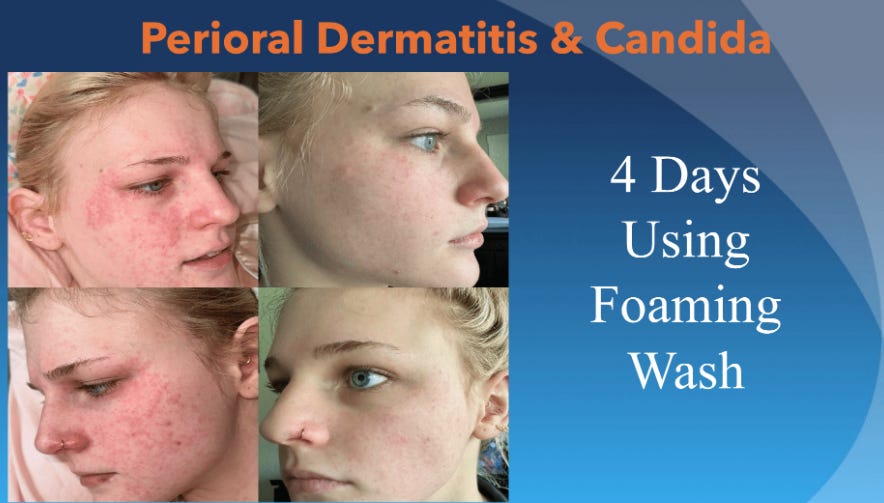
PERI-ORAL DERMATITIS
ERYTHEMA MULTIFORME

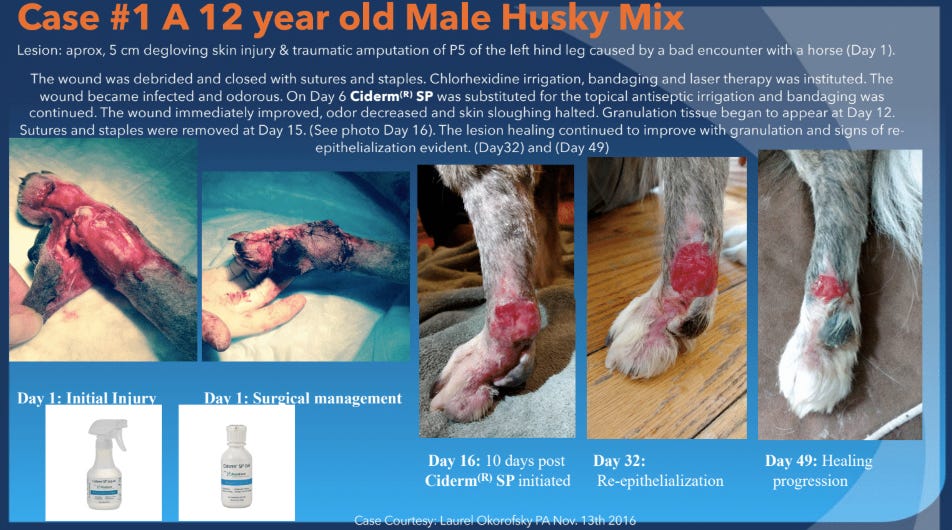
PET WOUNDS
Check out what happened to this poor Husky when he had “an encounter with a horse.” See the initial wound to the left and its healing progress on Day 16, 32 and 49:
EVIDENCE FOR “ORALLY INGESTED” CHLORINE DIOXIDE IN THE TREATMENT OF HUMAN ILLNESSES
Ok, now we are getting into dangerous territory as you will see from the examples of censored and/or retracted evidence. I initially considered a paywall here to try to compensate for the immense amount of hours and weeks I spent compiling this opus… but I couldn’t. If you appreciate this effort, please consider a paid subscription
MALARIA
NIGERIA: In a previous post, I detailed a report from an anonymous scientist with high-level security clearances during the latter part of last century where, in 1985, he helped design a Nigerian water treatment plant that initially and mistakenly uses a higher, but still non-toxic level (6ppm) than is typically used (0.5ppm). He reported that it led not only to the eradication of a cholera outbreak, but also that suddenly, no new malaria cases occurred in the town downstream from the plant. Obviously this is not data from a peer reviewed and published study but, knowing the source and his background, I find it highly credible and in-line with the following studies.
UGANDA: A documentary called “Malaria Red Cross Study” provides videotaped evidence that a study in malaria was done using chlorine dioxide in the form of MMS in Uganda in 2012. The International Red Cross, Uganda Red Cross, and a group called the Water Reference Center had members present that conducted the study and documented the results. In the study, 154 people tested positive for malaria and 154 were cured of malaria within 48 hours. After the study was conducted by the Ugandan Red Cross, the International Red Cross authorities denied that the entire study took place and refused to verify the results. The study was documented on video by several people, and these videos made their way online. Unfortunately, the malaria study documentary has been banned multiple times from YouTube but can be found on alternative video platforms like Brighteon and BitChute as well as on this page here.
CAMEROON: This published study (in an admittedly obscure journal) reported on 500 patients treated for malaria with a specially formulated sublingual tablet of chlorite that resolved all symptoms within two days. Further, their blood samples were free of any parasites by Day 6. This paper was quickly and unsurprisingly retracted and the principal investigator, Professor Enno Frye was then accused by his affiliated University of not having actually performed the study. Based on direct personal communication with Dr. Frye and my personal review of the study documents and protocol that he submitted to me, I believe there is sufficient evidence to believe the study (and its results) actually occurred. I will detail all in an upcoming post.
VIRAL RESPIRATORY INFECTIONS
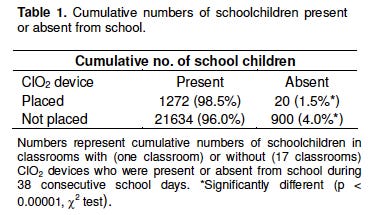
In Japan, they did a study where they released chlorine dioxide gas in the classroom of Japanese schoolchildren over a 38 day period, and they found it lowered absentee rates - i.e. there was significantly less illness in the classrooms exposed as can be seen in the table below:
EVIDENCE BASE FOR EFFICACY IN COVID-19
1. Bolivia - In a previous post, I compiled copious evidence of its use in Bolivia during Covid-19, taken from legislative documents and TV and newspaper reports which documented that, in early Covid-19, the passing of a national law allowed for the manufacture and distribution of orally ingested chlorine dioxide. Numerous media reports provided evidence of its being distributed by both the military and many universities.
The number of cases of COVID-19 subsequently dropped 93% from August 20, 2020 to October 21, 2020 and daily deaths decreased 82% from a peak on September 3, 2020 to October 21, 2020. Although other factors may have played a role in the decline in cases and mortality during this time, the fact that cases and deaths dropped in Bolivia but not surrounding countries suggests ClO2 likely played a large role in the progress seen in Bolivia (Insignares-Carrione et al., 2021)
THE BOLIVIAN RCT THAT WAS BLOCKED AFTER APPROVAL
A year later, in 2021, Dr. Patricia Callisperis and her team (she was one of the main physicians involved with the military program) made an attempt to conduct a randomized, double-blind study. The trial was developed by a branch of Bolivia's army, Clínica del Sur and the Spanish scientific society SCIB. The chlorine dioxide solution was developed by the Escuela Militar de Ingeniería (EMI).
Three Bolivian Army hospitals, were selected to enroll participants because in Bolivia, there are regions at different elevations above sea level, from valleys at 2,800 meters to high-altitude areas at 3,800 meters. This is important because the response to chlorine dioxide apparently varies depending on the altitude.
The project first got the approval of two bioethical comittees and then it was presented to AGEMED (The Bolivian version of the FDA) and the Comisión Farmacológica Nacional (CFN). Initially, CFN approved the solution to be used but AGEMED first delayed the protocol approval and then later rejected it. They didn't give any real reason, altough Dr. Callesperis suspects it was likely due to personal and political infighting within the agency
The below document is the approval letter from the CFN dated the 13th of August, 2021:
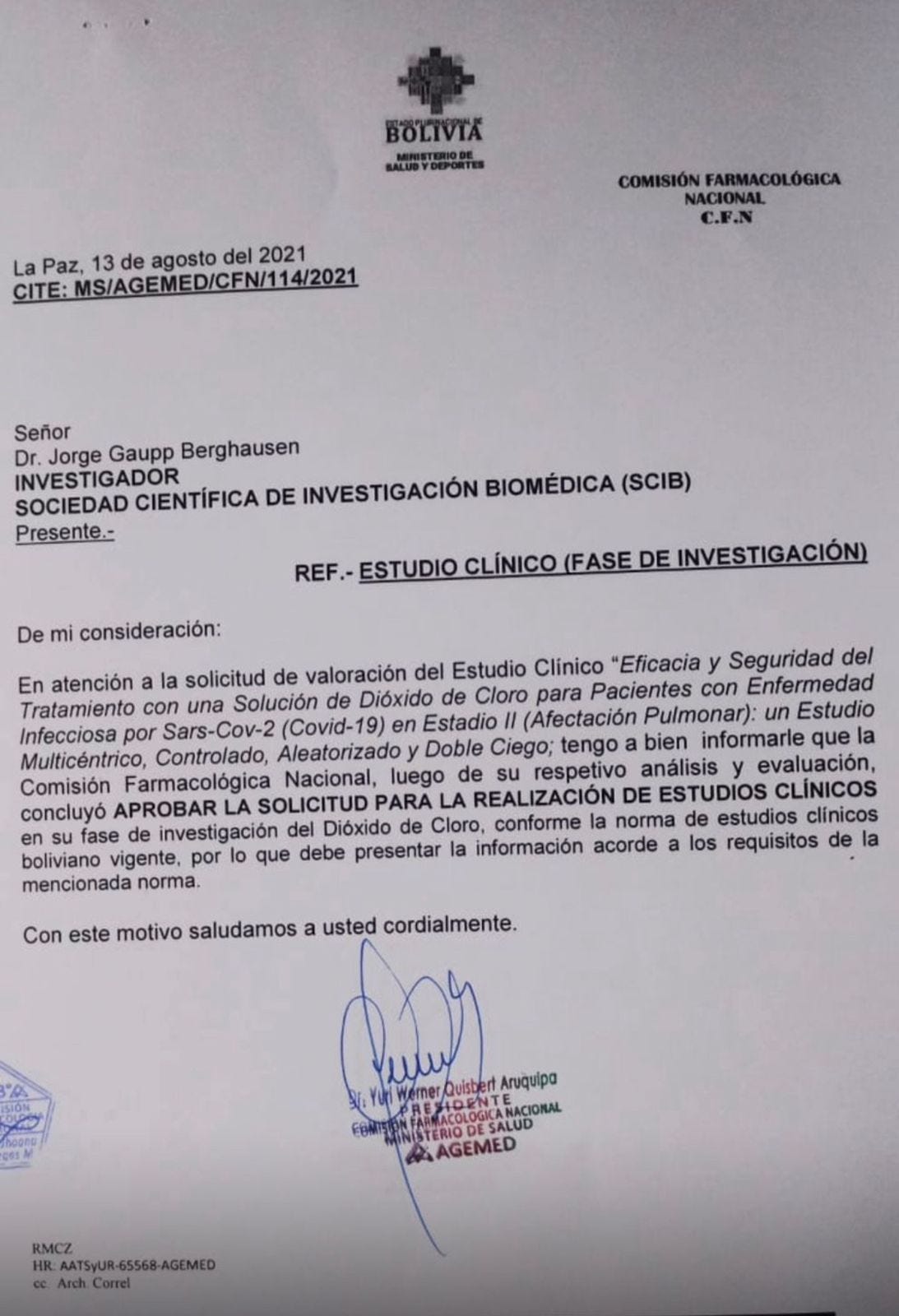
The English translation of the above:
Reference: Clinical Study, Research Phase
In response to the request for the evaluation of the efficacy and safety of a clinical study involving a chlorine dioxide solution as a treatment for patients with SARS-CoV-2 infectious disease (COVID-19), Phase 1, a multicenter, randomized, controlled, double-blind study, I am pleased to inform you that the National Pharmacological Commission, after its respective analysis and evaluation, has concluded to approve the request to conduct the clinical study in its research phase with chlorine dioxide, in accordance with the current Bolivian clinical study regulations.
Consequently, you are required to submit the information in compliance with the requirements established by the aforementioned.
Their study protocol:

2. A study of relatives of Covid patients who took chlorine dioxide solution found this practice led to a 90% efficacy in preventing infection (1,051 of 1,163 relatives taking chlorine dioxide regularly did not report any symptoms of Covid).
3. Another study found that patients treated with CDS were 19% less likely to experience Long Covid than patients who received standard Covid-19 therapies.
4. The AEMEMI doctors' technical report found an efficacy of 97% in the treatment of patients with COVID-19 during 4 days in Guayaquil/Ecuador (AEMEMI 2020).
5. More than 14,000 cases registered by over 3000 Medical Doctors of the COMUSAV association have not reported any serious side-effects in 6 months of use with 100% efficacy in treating Covid-19 patients diagnosed with PCR tests.
From the report by the COMUSAV organization way back in October of 2020;
“The clinical experience of Latin American doctors over the past six months suggests that the intake of 30 mg per day of chlorine dioxide dissolved in one liter of water, and drunk during ten events distributed over the day, is a successful treatment for COVID-19.”
7.Insignares-Carrione et al. (2020) In this paper exploring the hypothesis that chlorine dioxide would be safe and effective in treating COvid-19, the authors described having done “a preliminary trial” which involved 104 patients in Ecuador. They reported that all symptoms of COVID-19 began to decrease on the first day of treatment and were significantly reduced by the 4th day of treatment.
8.Aparicioco-Alonso et al performed a chart review of 1,167 outpatients that had been treated with with oral chlorine dioxide solution, using three different dosing protocols, two of them via oral ingestion and one via intravenous infusion (43 patients). Note this is the only published paper that demonstrates the safety and utility of IV chlorine dioxide administration. The average daily dose taken orally was 98mg/day (1.2mg/kg) for 15.87 days. 99.03% of all patients recovered. Reported side effects were mild, transient, and rare (and they were ill with Covid):
(6.78%) reported mild-sporadic secondary effects posterior to ClO2 intake: headache (2.20%), diarrhea (1.58%), gastritis (1.32%), dizziness (1.14%), nausea (1.05%), vomit (0.44%), rash (0.44%), throat pain (0.26%), myalgia (0.18%), colitis (0.18%), tachycardia (0.09%), and chills (0.09%).
9.Another controlled study of 40 patients with Covid was published on a non-peer-reviewed, predatory journal site. It purportedly found significantly decreased symptoms at multiple time points among the treated patients vs. controls. However, based on personal communications with physicians peripherally involved in the study, I will not list due to significant concerns they raised about the validity of the control group data.
TUBERCULOSIS
Evidence for the efficacy of chlorine dioxide against TB is also unpublished and comes from my anonymous source, the translational scientist that worked closely with scientists from bioweapons programs in the UK and USSR. He helped the famous Russian Bioweapon whistleblower Vladimir Pasechnik defect to the UK. He informed me that Pasechnik had done studies in the treatment of TB and reported that it “cured TB.” That’s all I got.
However, I am proud to report that my new non-profit, Rebuild Medicine, has given a grant to a group that is beginning a study in TB in a foreign country (that I will not name) where Research Ethics approval can be obtained (something that, as of now, would never happen in the United States). To wit, my colleague, Dr. Mitch Leister applied for IRB approval for a study of chlorine dioxide in Covid-19 and, despite submitting numerous studies demonstrating the safety of the therapy, was promptly denied permission by the University of Colorado who claimed that the FDA would not allow it.
CANCER
In vitro-evidence for its utility in treating cancer comes from two seperate experiments where they exposed cancer cell lines to chlorine dioxide to assess its ability to halt proliferation. They found it did so effectively in a lung cancer cell line, two breast, and three colorectal cell lines
The clinical evidence of efficacy in cancer comes from several published case series, the first authored by my newfound friend and colleague in Paris, Dr. Laurent Schwartz, who published on his clincal experience treating three patients with metastatic cancer that had failed all other therapies:
Patient 1: 65 y.o man with metastatic adenocarcinoma of the pancreas. Patient decided to refuse chemotherapy and instead underwent treatment with lipoïc acid, hydroxycitrate, and orally ingested chlorine dioxide. Blood tests and imaging returned to near normal and remained stable at 18 months (Wow. In metastatic pancreatic cancer?)
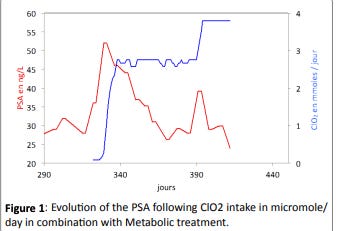
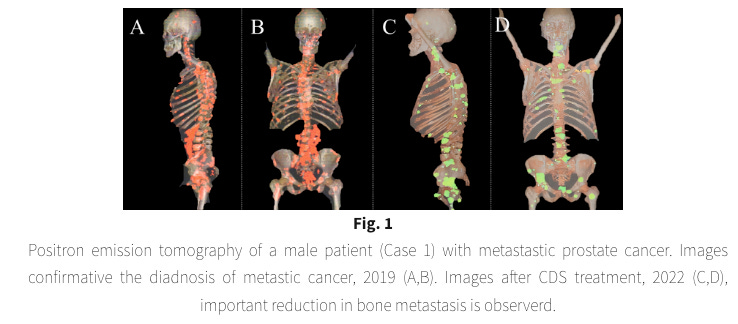
Patient 2: 67 year old man with Gleason 8, hormone resistant metastatic prostate cancer. Oral chlorine dioxide ingestion protocol led to a sharp decrease in his PSA level as well as decreased pain and an increased Karnofsky performance score. Despite taking 8 times a day, some months later his metastatic pain, which had almost completely disappeared, returned and caused significant insomnia. He increased intake to every 90 minutes during the night in addition to his daytime dosing. Nightly metastatic pain decreased drastically from day one, and the second part of the night was practically pain free. The PSA decreased again linearly from 39 to 24. See below:
The other case series is still on a pre-print server:
Patient 1: 64 y.o man with metastatic prostate cancer, diagnosed in 2020, refused chemotherapy initially. Instead he received 2.5 months of daily intravenous administration of the glucose analog 2-deoxy-D-glucose (2DG) and a ketogenic diet with 20 hour fasting windows daily.
The patient then began both an oral and enema chlorine dioxide protocol along with zeolite. 2 years later he adopted an intravenous chlorine dioxide protocol. 3.5 years from diagnosis, he lives without any limitations in his daily routine and has normal PSA levels. See PET scan below:
Patient 2: 65 y.o with metastatic renal carcinoma and diabetes.Initially received two immunotherapy agents which caused immense side effects and which he discontinued. A lung nodule grew despite the treatment. He then did both an oral and enema chlorine dioxide protocol. At almost 5 years from diagnosis he is in complete remission.
Patient 3: 73 y.o woman with metastatic non-Hodgkins lymphoma received 8 sessions of chemotherapy with significant side effects. New bone mets were then noted and she refused any further chemo or radiation that was being offerred. She then started on an oral chlorine dioxide protocol combined with oral DMSO but low back pain continued. She then added an enema protocol along with 18-20 hour fasting windows on a daily basis. At 38 months from diagnosis, a significant reduction of the tumors in the invaded tissues was observed without new metastases.
Although I did not do this for any of the other disease applications, the vast majority of the clinical evidence base for oral chlorine dioxide consists of many thousands testimonials. On my colleague Jeff’s “Curious Outlier” Substack, in his review of its efficacy in cancer, he included 10 cancer testimonials which can be directly reviewed at this link.
INTRATUMORAL INJECTIONS FOR CANCER
A study employing intratumoral delivery in mice with lung, melanoma, and breast cancers showed potent responses.
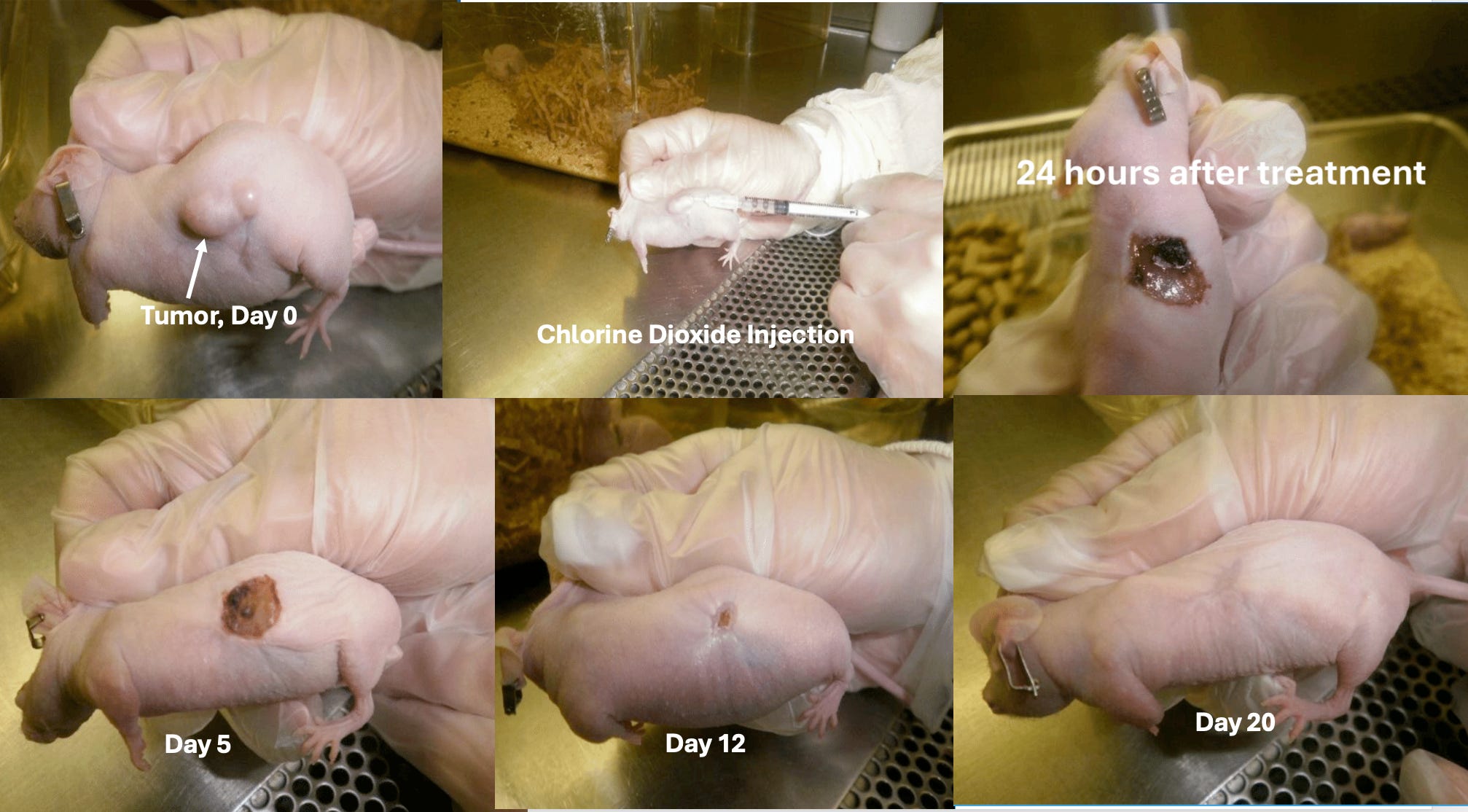
I have not yet posted the history of Howard Alliger, the man that founded Alcide Corporation (now Frontier Pharmaceuticals). He filed a patent in 2017 where he provided experimental research that was performed with mice that showed a complete tumor regression within 48 hours of injection. Check out this experiment done in 2017 at Stony Brook University where they transplanted a human brain tumor onto a mouse and then injected it with his chlorine dioxide preparation:
In a recent communication with Howard Alligers daughter Valerie (co-owner of Frontier Pharma), she writes:
As requested, please find attached information about the cancer treatment developed by my father, Howard Alliger.
The treatment consists of a chlorine dioxide complex, called INtume™, that is injected into a tumor. He received a patent in 2018 (see attached).
Testing is in early stages. We are still optimizing formulation concentration and dosage. Testing mainly consists of the injection of implanted tumors on the backs of mice. We have also done direct injections into organs to test for toxicity and also did a small study to evaluate the oral ingestion route.
Tumors tested include: prostate, breast, brain, pancreatic, lung, colon, melanoma, and ovarian cancers. Results have varied depending on formula, dosage and delivery method, but mainly, what we find is that INtume will disintegrate tumor tissue within 24 hours, leaving an open wound which heals. In some cases, the tumor was either partially or fully disintegrated (depending on technique) but the tumor regrows around the edges. We have 3 (maybe 4) cases where the tumor was disintegrated and did not return, and the mice lived out their natural life spans. (See the attached Zimmerman report.) This is promising and we believe can be repeated with the correct technique and formula.
Testing sites include: Stony Brook University in NY, Southern Research in Alabama, and Memorial Sloan Kettering in NY. Testing is unfortunately stalled at this time due to lack of funding.
A chlorine dioxide researcher by the name of Xuewu Liu has reported on his Substack that he has been collaborating with clinics in Germany, Mexico, and the Phillipines (with more apparently joining) where they are performing protocolized intra-tumoral injections of cancers.
To date has has “posted” (not published - apparently he is having trouble getting his paper accepted) on approximately 30 patients who have received injections with consistent reductions in both tumor presence, tumor size, or cancer pain. Specific descriptions of results in patient with tumors can be found at these links: perineal, liver and lung, breast, and peritoneal)
In a personal communication with me:
I am pleased to report to you that my German partner clinic is currently using my intratumoral chlorine dioxide injection therapy to treat five advanced cancer patients. The treatment results have been surprisingly consistent. Regardless of tumor size or number, we inject a high concentration of chlorine dioxide (20,000 ppm) directly into the tumors. Immediately after the injection, significant tumor necrosis can be observed via ultrasound. Subsequently, the tumors shrink in a highly consistent pattern: 70% reduction in 2 weeks, 90% reduction in 2 weeks, and potentially complete disappearance within a month. This happens with just one injection.
In another personal communication, the author also informed me:
“Amazon.com removed my book, The Chlorine Dioxide Miracle: Safeguarding Health with Safe and Effective Applications, 1.5 months after its self-publication.”
TESTIMONIAL EVIDENCE FOR ORALLY INGESTED CHLORINE DIOXIDE
For those that dismiss the value of anecdotes and testimonials that have not been published in peer-reviewed medical journals, remember the old axiom, “one anecdote is one anecdote, a thousand anecdotes is data.” Never in history has this been more true that on the use of oral chlorine dioxide.
My friend and colleague who goes by “Jeff” is the Director and Producer (and webmaster) of The Universal Antidote Documentary and website. Taken from a transcript of the narration of his documentary:
There has been a quietly growing grass roots movement of people using chlorine dioxide to self treat disease and they have been using chlorine dioxide to cure a wide range of infectious diseases including antibiotic resistant bacterial infections, malaria, influenza, hepatitis, and more. Others have had some remarkable results relieving diseases such as arthritis, cancer, and other inflammatory diseases. From written testimony reports to video testimonies, there have been hundreds if not thousands of reports.Many of these have been banned from media platforms like YouTube, Facebook, and Google search engine.
Beyond the above studies and reports, as Jeff mentions, there are literally tens of thousands of testimonies from missionaries and providers from all over Africa (and the world) about quick recoveries from malaria and other diseases. See this 7 minute video of a missionary relating his many thousands of treatment experiences. Note his face is blurred in the video and he only gives his first name:
You can also see video interviews of some of the most experienced chlorine dioxide practitioners in the world such as Jim Humble and Mark Grenon, founders of the Genesis II Church of Health and Healing where they recount the many dozens of teaching seminars they have given around the world and the tens of thousands of patients they have seen recover with their MMS protocols.
Finally, other chlorine dioxide obsessives (of which I am admittedly now one) have devoted a significant portion of their energies compiling submitted testimonials on websites, Substacks, and Telegram channels (and in several languages as well - Italian, Spanish, Vietnamese, and Japanese to name just a few. A large yet incomplete list of these databases of testimonials can be found below:
Jeff’s Telegram Group is called The Universal Antidote Videos, has over 85,000 members. Jeff is beginning to transfer all of his Telegram group testimonies on his Substack here. Jim Humbles website has categorized testimonials here: mmstestimonials.co. Brian Stone compiled over 250 testimonials in this free on-line pdf book. Below is a screenshot of just some of the table of contents:
I know its a bit excessive but Jeff also compiled a list of testimonial websites in other languages as follows: English, Spanish (here, here, and here), German, Italian (here and here), French, Japanese, Chinese, Vietnamese, and Algerian!
Many video testimonials can also be found here.
CONCLUSION
In summary, the published evidence for:
IV chlorite formulations is increasing, high quality, and shows efficacy in a broadening array of illnesses.
Topical chlorine dioxide (and one case of just oral ingestion) in the treatment of all sorts of non-healing wounds is both compelling, reasonable quality, reproducible and increasing.
Orally ingested chlorine dioxide consists of a handful of what “the establishment” would call “extremely low-quality” studies in Covid-19 while the most impactful evidence comes from either retracted studies (Cameroon malaria study), “scrubbed studies” (Uganda malaria study), “hearsay” (Nigerian water treatment plant disappearing malaria cases in the town), or is “classified” (Soviet scientists curing TB).
To me at least, the most convincing evidence for oral ingestion of chlorine dioxide rests on the “real-world” testimonials from all over the world by the many many thousands of both practitioners and patients who have used it to treat a wide array of diseases.
Again, the above is why I am hoping RFK Jr. can somehow open up the restrictions on research using orally ingested chlorine dioxide in order to make the treatment both legal and more mainstream so it can have even more impact on the health status of the world.
In summary, the many mechanisms of action of chlorine dioxide makes it broadly antimicrobial against nearly all infectious pathogens, reduces inflammation, prevents scarring. aids in wound healing, is non-toxic when orally ingested (in appropriate concentrations), reduces oral plaque, treats oral atrophic candidiasis, is a potent deodorizer. In cancer, it has in-vitro anti-cancer cell effects, stimulates an in-vivo anti-cancer cell immune response and is also effective when injected intra-tumorally or via a combination of oral, enema, and IV administration.
This combination of properties is not found in any other compound. The therapeutic uses for chlorine dioxide are endless. And therein lies the problem. Stay tuned for my upcoming posts on the plights of the more modern pioneers of chlorine dioxide therapies.
If this post whet your appetite for learning more about chlorine dioxide, and you appreciate the time and effort I put into researching and writing my posts, please consider a paid subscription.
If anyone is interested in going to the “Truth Seekers” Conference and golf tournament with over 40 speakers from all over the world, sign up at this link: and see below flyer (I love how they used a picture of me from 15 years ago :). They also claim that I am Board certified which I am no longer, whoops…

Thank you for all the amazing innovations you have provided in research to aid patients’ health!
Thank you Dr. Kory for this comprehensive accounting of the many uses of chlorine dioxide and for recognizing the work of my father, Howard Alliger, his past company, Alcide Corp and our current company Frontier. After more than 40 years in the field of chlorine dioxide it’s incredible to see how far reaching ClO2 has become, and what’s more incredible is that we still don’t know the half of what it can do. It’s going to take all of us to see that through and your contributions to that effort are instrumental.