

Bolivia's Use Of Chlorine Dioxide Led To The Best Outcomes In South America
Chlorine dioxide is a broad antimicrobial that is safe for ingestion. Bolivian MP's passed a law supporting widespread use to combat Covid. This action led to a massive reduction in deaths.

In my first post in this series, I introduced the topic of chlorine dioxide as a therapeutic within its “political” context, not scientific. After a cursory introduction regarding its safety along with a few citations of its efficacy, I highlighted the regulatory, media, and judicial attacks against any who manufacture, recommend and/or sell chlorine dioxide for medicinal purposes via oral ingestion.
A key point I brought attention to is the bizarre prohibition against “oral ingestion” that “they” are trying to block at all costs (despite studies of both oral and IV administration showing little to no toxicity and the fact that there are numerous products already on the market for oral and/or dental applications).
In this post, I will share what I recently learned of what happened in Bolivia around chlorine dioxide. I think it is a story the world needs to hear. Again, these are the first of a series of posts on chlorine dioxide with later ones going more deeply into the data on safety and efficacy fas well as treatment approaches for various conditions. If you don’t want to miss the rest of the series, I suggest you subscribe now:
THE BOLIVIAN EXPERIENCE
The most notable event around chlorine dioxide in Bolivia was when a group of parliamentarians managed (somehow) to pass a law which allowed for the manufacture and distribution (and use) of chlorine dioxide in Bolivia on October 14, 2020:

Although this was a national law, one of the largest of the 9 departments in Bolivia, that of La Paz, had already passed a similar version on Sept 9, 2020:
However, before these laws were passed in Bolivia, media attacks on the legislators responsible already began in June 2020. This one is a doozy:

“A chemical discredited to exhaustion by the world scientific community.” You can say that again.
To give what the Bolivians did some additional context, know that other South American countries also attempted such legislative efforts: a similar petition action was taken by Brazil’s chamber of deputies a year after Bolivia, but the law was quickly rescinded after the president changed from Bolsonaro (right) to Lula (left) - i.e. the latter’s administration quickly ended the petition:

And then in Peru, a group of parliamentarians passed a resolution to “study its use” in Covid (49 parliamentarians to be exact). However, as this newspaper article outlines, the fight over the resolution and over chlorine dioxide was both highly political and either willfully or negligently misinformed by the health authorities in opposition. To wit, this is the concluding paragraph of the article:
“The issue is how to investigate a substance harmful to humans. I do not believe that any ethics committee in Peru approves such an investigation. Who is going to want to enroll in a study where informed consent tells you that it can cause heart arrhythmia, liver failure and you can die? ”, asks, laughing, the doctor.
Also know that in Peru in June 2020, the Chief of the Covid Command in Ayacucho, a region of 100,000 people, was dismissed for treating patients with chlorine dioxide:

A similar pro-chlorine dioxide petition effort also took place in Paraguay’s Chamber of Deputies. Below is a screenshot of the title and cover page followed by a ChatGPT translated summary:
1. Scientific Findings and Arguments
The document discusses the potential uses of chlorine dioxide, particularly emphasizing its purported benefits in health treatments. Proponents claim it has antimicrobial properties and can treat various conditions. However, it lacks recognized scientific validation, and health authorities generally caution against its medical use due to safety concerns.
2. Legal Implications and Proposed Regulations
The legislative proposal aims to legalize and regulate the production, distribution, and use of chlorine dioxide within Paraguay. Key points include:
Setting standards for its manufacturing and quality control.
Establishing protocols for medical administration.
Outlining penalties for misuse or non-compliance.
3. Controversies and Public Health Aspects
The proposal is controversial because global health organizations, such as the WHO and FDA, warn against using chlorine dioxide for medical purposes, citing potential toxicity and lack of proven efficacy. Supporters argue for its potential benefits, while critics highlight the risks of promoting unapproved treatments to the public.
THE BOLIVIAN EXPERIENCE
Lets get back to Bolivia now because that is where the “action” really happened around chlorine dioxide in South America.
After the law supporting the manufacture and use of chlorine dioxide was passed, the Bolivian Ministry of Health quickly issued a press release attacking the law and also the idea that chlorine dioxide was safe or that there was evidence it had anti-viral properties (which is astounding given it is likely the broadest and most effective viricide in use).
The Ministry tried to assert their authority by stating that the law was in opposition to its guidelines as a health authority and its responsibility to protect the health of the general population in Bolivia. Of course the “health of the Bolivian people” was their primary institutional concern! Who would ever openly question that?
I bolded the most relevant parts of the Bolivian Ministry of Health release below (translated using google translate). Before you read it, I think it will be helpful to remind you of the definition of an “appeal to authority” argument which is used incessantly in the media and by public agencies around chlorine dioxide (and ivermectin, HCQ, Vitamin D etc, etc).
Definition of “appeal to authority” argument:
a type of logical fallacy where someone claims that a statement or proposition is true solely because an authority figure or expert in the relevant field has endorsed it.
Now read the Health Ministry’s release below and notice how I helpfully bolded for you the number of times that they used this type of “logical fallacy” - they referred to a “disapproving expert” no less than thirteen times in 4 paragraphs to be exact:
The Ministry of Health informs the public that the "Law that regulates the preparation, marketing, supply and consented use of the Chlorine Dioxide solution (SDC) for the prevention and treatment of the coronavirus pandemic (COVID-19)" sanctioned by the Plurinational Legislative Assembly, is in stark contrast to what is established by this State portfolio in its capacity as the governing authority in health matters in the country and whose fundamental responsibility is to protect the health of the population.
We regret that the members of the Plurinational Legislative Assembly have been surprised in their good faith and have not gone to experts or institutions knowledgeable in the matter to be appropriately advised before approving this law. (Ed: “Experts” and “Institutions” eh?)
It is necessary to note that various national and international institutions have spoken out about the health risk of consuming this product, such as the Bolivian Academy of Medicine, various Scientific Societies affiliated with the National Medical College, the College of Biochemistry and Pharmacy, the Committee Scientific advisor to the Ministry of Health, national universities such as UMSA, UAGRM and the Universidad San Francisco Xavier de Chuquisaca. The latter institution has just published the results of a clinical investigation in which it concludes that “Chlorine dioxide has no antiviral effect.”
This study was carried out by professors from the Faculty of Medicine and the Departmental and Municipal Health Directorates. At the international level, the WHO and PAHO do not approve it and chlorine dioxide is not part of the international list of medicines. Prestigious international institutions in the field of drug regulation such as the Federal Drug Administration of the United States (FDA) and the European Medicines Regulatory Agency (EMA), have a clear position with scientific foundations against the use of chlorine dioxide for therapeutic purposes. In practice, there is no country, at least in our hemisphere, where it is legally authorized, because there is no scientific evidence, there is no evidence to demonstrate its preventive or curative properties, its promoters resort to testimonies from people, supposedly treated, and the testimonies have no scientific validity if the product is not supported by controlled clinical studies that demonstrate its effectiveness in the sense that it has curative properties and demonstrate its safety and that it does not produce adverse reactions. On the other hand, it is noted that the approved law incurs in contradictions in the following articles: Article 4. (Marketing of chlorine dioxide).
b) It authorizes pharmacies to market it “without the need for a medical prescription and with the full consent of the buyer” (Ed: Amazing!)
Article 6. Administration.
“Medical professionals may administer chlorine dioxide solution, with the informed consent of the patient or a family member, in accordance with the established protocols”
Article 7. Use. (Ed: I included only the concluding paragraph for brevity here:
… Therefore, the Ministry of Health, in its capacity as the national governing authority whose main responsibility is to ensure the health of citizens, maintains its position that, since chlorine dioxide has no scientific evidence demonstrating its therapeutic or preventive nature and since it is not registered as a pharmaceutical product, it will maintain its prohibition at the national level and will hold legally responsible any authority or person who, in an irresponsible manner, has caused damage to health by encouraging the consumption of that product.
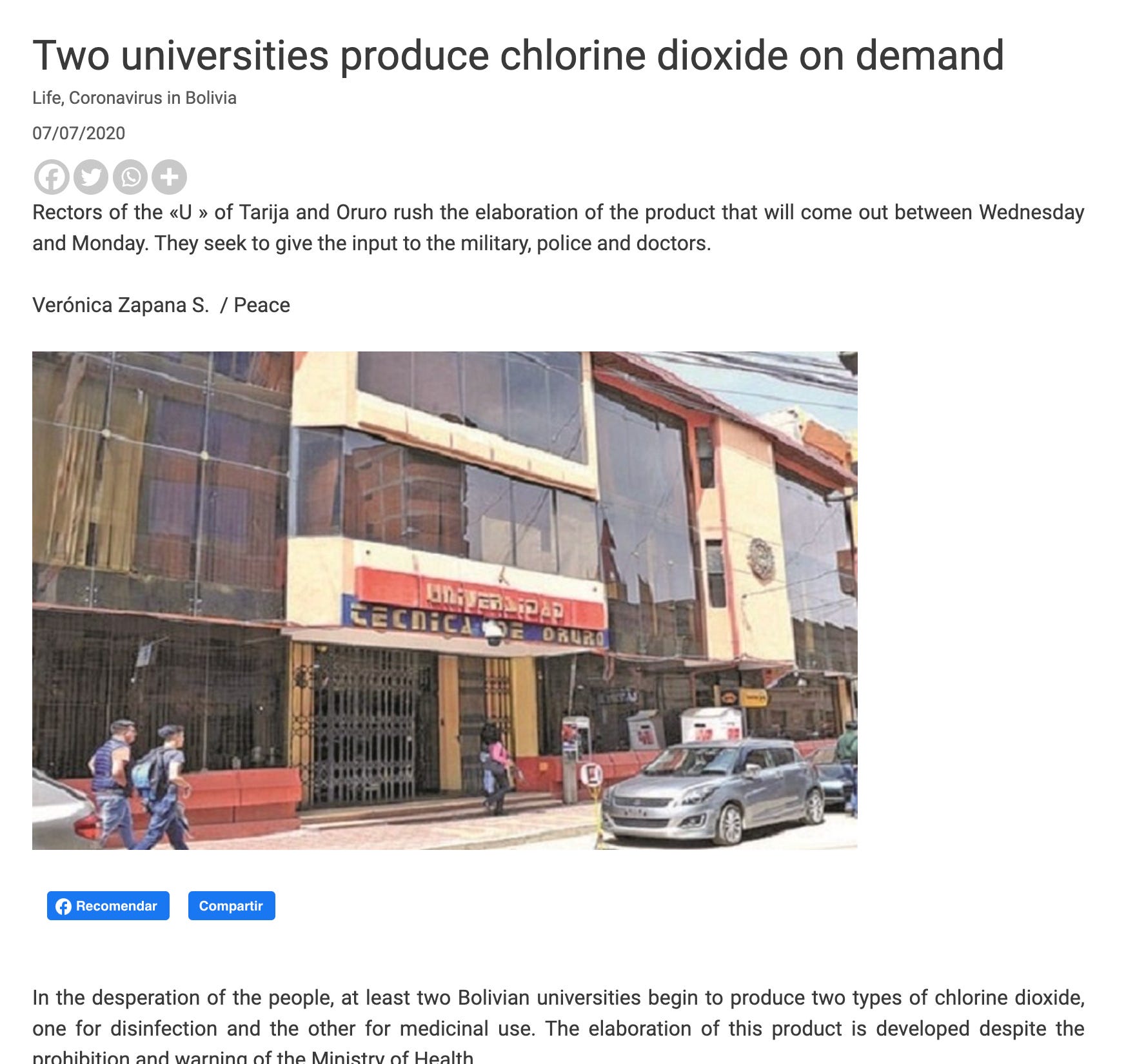
Now, although the law was passed in La Paz on September 9, 2020, interestingly, already back in July, there were reports of Bolivian universities producing chlorine dioxide to treat Covid:
Now watch this short news interview below with a physician who served as a Bolivian military representative to announce the distribution and treatment program. The below is subtitled, and a transcript in English can be found here, it is less than two minutes:
Unsurprisingly, after Bolivia passed the law allowing for the manufacture and distribution of chlorine dioxide, newspapers (gleefully?) reported that this action directly defied the PAHO (a specialized health agency of the United Nations) as reported in this news article):

A paragraph from the article:
Furthermore, the Pan American Health Organization (PAHO) issued a warning against the use of chlorine products as treatments for Covid-19. «PAHO does not recommend using products based on chlorine dioxide or sodium chlorite orally or parenterally (intravenous, intra-arterial, intramuscular, and subcutaneous) in patients with suspected or diagnosed Covid-19, or in any other case, because there is no evidence on their efficacy and the intake or inhalation of these products could cause serious adverse effects, is stated in the document.
Check out CNN jumping in with coverage of the Bolivian legislator’s efforts:

Know that the physician in the video above was asked to represent the military’s program at the time (although she is not in the military). Her name is Dr. Patricia Callesperis and she has become a new and trusted colleague and friend to me as I pursue my research into chlorine dioxide. Here is a short bio of Dr. Callisperis:
Dr. Patricia Callisperis Vieira Dias holds a medical degree from the Pontifical Catholic University of São Paulo, with a specialization and subspecialty in Pediatric Traumatology and Orthopedics from the Federal University of São Paulo (UNIFESP). With 25 years of experience, she has held leadership roles, including Director of the Children’s Physical Rehabilitation Center (2001-2006), and currently serves as Director of Clínica del Sur in La Paz, Bolivia, while actively contributing to professional organizations such as the Bolivian and Brazilian Societies of Orthopedics and Traumatology, and the Ponseti Associations in Bolivia and Latin America.
More pertinent is that during the last ten years of her career, she became professionally dedicated to researching and promoting the use of chlorine dioxide as an alternative therapy. The “origin” story of her interest into chlorine dioxide as a therapeutic is both visually and emotionally telling:
“I used to have these lesions in my mouth every month or every couple of months. That type of lesion would appear repeatedly. I received treatment from various doctors, and I even traveled to the United States to a center because they told me it could be lichen planus, coxsackie, a herpes mutation, and so on. I received many diagnoses, but nothing improved. I used balsiclovir, I tried many vitamins to boost my immunity.

They wanted to perform a biopsy, and that’s when I discovered chlorine dioxide. I started taking chlorine dioxide and since then, I’ve never had those lesions again. I’ve been able to practice my profession normally and perform surgeries because the lesions even started appearing on my fingers, preventing me from operating. Now, I’m fine.”
After overcoming the chronic lesions in 2017 with chlorine dioxide, she began using it to treat and publish reports of patients with varicose ulcers, diabetic foot, and other conditions, achieving promising results.
During the COVID-19 pandemic, she applied chlorine dioxide for hospital disinfection and in patients without access to hospitals, making a significant impact. In 2021, she organized the first Oxidative Therapies Congress in Santa Cruz de la Sierra, bringing together specialists from 16 countries and advocating for scientific research to support the use of chlorine dioxide. She is currently committed to the responsible validation and application of these innovative therapies.
Here she is more recently, with all lesions in the distant past:

Back to Covid now: when I asked her for the published results and/or data on the impacts of the national and military chlorine dioxide program, she informed me that, unsurprisingly, the Bolivian “FDA” (known as AGEMED) denied her and her colleagues' application to do a prospective double blinded study (even though they had manufactured a “placebo” - i.e. a solution that tasted like chlorine dioxide but was inert). Dr. Callisperis pointed out that the “pharmaceutical division” of AGEMED actually did approve the study but the “higher-ups” in AGEMED then rejected it.
Then AGEMED went even further and denied their application and access to data to be able to do a retrospective observational study. This was shockingly unsurprising to me (odd paradox I know) just as it would be for the vast majority of my readers.
Thus the actual scientific and clinical data results of the Bolivian program are not accurately known (which I would argue is as intended) however, as you will see below, the epidemiological and anecdotal evidence is overwhelming (including reports of eradication of Covid in certain cities).
The below interview televised on “El Pais” is fascinating given that El Pais is one of the largest media outlets in Bolivia. Unlike the way the U.S media treated the topic of ivermectin, El Pais “presented both sides” by interviewing one clinical researcher who stated its safety and efficacy and then they interviewed a pharmacy regulator who stated there is insufficient evidence for chlorine dioxide and that it is dangerous to patients. The actually broadcast contrasting opinions instead of having someone simply call it a horse dewormer (or toxic bleach in this case) over and over again. Worth a watch (I added English subtitles, 6:16 total):
One statement from the clinician expert in chlorine dioxide jumped out:
“over 50,000 in Cochabamaba were using chlorine dioxide, and the lines to get treated were up to 500-800 people a day.”
I swear that was my initial vision/fantasy after discovering the potent efficacy of ivermectin in Covid - I first imagined a U.S national ivermectin distribution program! I had thought we could just “copy” the 40 year old WHO ivermectin distribution programs against parasitic diseases that had been conducted across Africa and other continents. Do you guys remember Fauci’s national ivermectin distribution program for Covid in the U.S.? I didn’t think so.
Anyway, let’s contrast some statements from the “regulator” and the “expert clinician:”
Chlorine Dioxide Expert Clinician:
So, when they threaten us with trials, they think they are going to shut us up. This is something that is not going to stop anymore. This is something that has already grown in such a way that it is impossible for any human power, no matter how much, I don't know how no human power, no matter how many, what do I know, high level authorities want to stop it. They are not going to scare me with a process because I am not doing any harm. They have to prove to me that I have done any harm.
Ed: His statement “they are going to threaten us with trials,” really resonated with me given that is what they did with ivermectin - health authorities across the world refused to recommend its use until “they” could publish trials deliberately manipulated to try to show ivermectin did not work.
This is extremely important to be aware of because I am certain that if they ever remove the restriction on chlorine dioxide research, the first trials to be conducted and published will be trials manipulated to obtain “negative” results. This is a tactic from the Disinformation Playbook called “The Fake” as I have harped on many times before and is literally the primary tactic at which they suppress, prevent, and distort evidence of efficacy of safe, inexpensive, widely available therapies that produce little profit to industry:
Bolivian Health Regulator comments:
“there is a weakening of the institutional structure, of the confidence institutional structure, of trust in the organs of the state, of trust in public institutions. And that is part of the problem here and we regret that it is that it has ended up into something so harmful to the population. (Ed: I wish he had expanded upon why such a widespread loss of trust in these “organs of state” was occurring).
People are taking it either too much or in an artisanal way and they are hurting themselves. The people who are taking it are uninformed and are doing what they can with a very difficult time that all Bolivians are going through a very difficult moment that all Bolivians are going through. It is a very difficult moment in which there is a lot of fear, desperation and little information. The people are clamoring for something that will help them to maintain their health, not to die, in other words.
Ed: Notice how he provides no data to support that people are hurting themselves.
As I detailed in my first post, recall that the worlds “authorities” moved against chlorine dioxide even before their later coordinated attacks on HCQ and then ivermectin.
So, with all the fervor and national attention on chlorine dioxide in Bolivia, the powers that be hit back.. with lies (if you read the article below they mention 5 people being poisoned but no links or references to this statement were given, plus, even more absurdly, if you look at the sub-headline, they mention 10 people being “poisoned.” Isn’t it weird that a simple number was so different in the headline and the text of a major media newspaper?

Dr. Callisperis recently told me,
“The universities started to produce chlorine dioxide too. And then in some of the cities (Ed: all hyperlinks go to news reports showing evidence they were doing this) like Universidad Técnica de Oruro, Universidad Gabriel René Moreno, and Escuela Militar de Ingeniería in La Paz. and they started giving it out for free to all the people.”
This is further substantiated with this interview with a Rector of a Bolivian University on this news program (in subtitles):
The interview above was held with the Vice Rector of the Gabriel René Moreno University, Dr. Osvaldo Ulloa. He first admits that the university was producing it for their workers and students:
our University Social Security, directed by Dr. Méndez is justly using it, he has said so publicly and its effects are quite beneficial and that is very important because what we want is to collaborate.
Well, actually we have developed it and we have donated it, we can say, to the university insurance and the idea is to produce it to distribute it in a totally free way.
For that, of course, we need the support of the authorities such as the governor, the mayor's office, so that they are the actual owners, right?
Those responsible for managing the first, second and third level hospitals in our capital. So, therefore, doctors in some way depend on the Ministry of Health and of course also municipal governments and the government.
So, in order to use it in the treatment of these people who are hospitalized, we necessarily need their authorization. We know that there is a controversy at this moment, right?
From the Ministry of Health, which issued at a certain time a ban on consumption, since it claimed that it is a toxic product that we have done the research into. Doctors must control the supply of this product, even though we are aware that the product is not toxic, what is more, paradoxically I could tell you that if someone wants to commit suicide or, for example, has the idea of committing suicide and wants to commit suicide with chlorine dioxide, it is not you will be able to get it (sic: done) because it is not really toxic.
So rather with any other the drugs that are being used it would be much easier to do so. ŸOusand then that shows us that this product in the quantities and in the measurements of its components, as established and as indicated, could be very beneficial to combat the coronavirus and above all to give life expectancy to people, that is the objective that we pursue. We are aware that so far there is no definitive protocol that says this definitively cures the coronavirus (Ed: How can there be if authorities refuse to allow publication of the data or to do prospective research?)
All the medications that have had good results are still in research and that research is still ongoing.
Basically, if you listen to the whole interview, the Rector of the University states that they were having excellent results treating students, staff, and the community while pointing out that “the Ministry of Health calls it a toxic product.” Further he points out that in order to treat the patients in the hospitals, they “need the collaboration of the Ministry and municipal governments and federal government” (which they were not getting).
Interestingly, the head of Human Rights for Bolivia ended up intervening on the side of the chlorine dioxide program by going after the Ministry of Health for not drafting the regulations on the use of chlorine dioxide which the law demanded they do. This article below called out the “administration” for not obeying the law of the people. Imagine that?

On the issue of the University Rector calling out for collaboration with authorities to help the patients in hospitals, in the below article, the Mayor of San Juan De Chiquitos boldly proclaimed that they “emptied their ICU of 16 critical patients” after using chlorine dioxide and that “he was bringing the records of all 16 patients to La Paz” (Ed: like data makes a difference).
Again, here is another anomaly in reporting - read the translated headline below and then go read the article, you will find a massive discordance between the headline and what is actually written in the article which is almost all positive towards chlorine dioxide!

So, a law was passed allowing for the production and use of chlorine dioxide and the military and universities started producing and treating Bolivians ill with Covid and Bolivians were lining up all over the country to receive treatment. What were the impacts of this campaign? Since the clinicians and researchers were not allowed to gather nor publish data in an organized way we are left with, once again, epidemiological data. Let’s see, from Our World in Data:
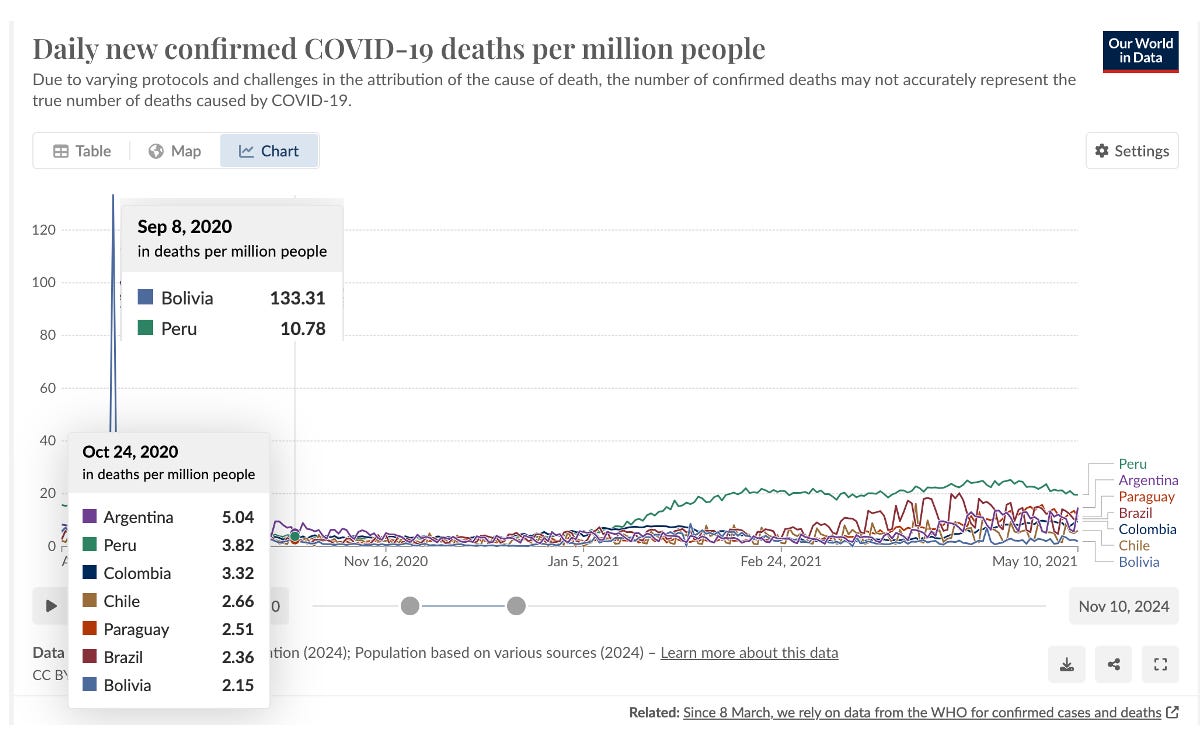
As you can see, Bolivia suffered a sudden and unprecedented spike (even for South America) in Covid deaths in early September 2020, where on Sept. 8, they were recording 133 deaths per million and then 6 weeks later, they recorded the lowest in S. America at 2 per million. But notice the sharpness of the spike - soon after the first of “the laws” were passed in La Paz, the rates and deaths disappeared rapidly and within a month, Bolivia had the lowest death rate in S. America. Coincidence?
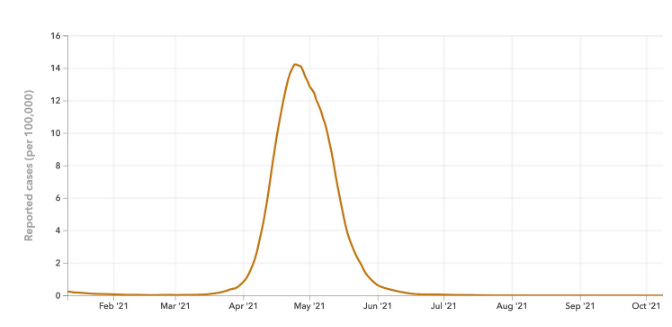
Does the “sharpness” of the spike on the graph of Bolivia remind you of India’s delta wave in Uttar Pradesh (from my previous series called “The Miraculous Success of Uttar Pradesh”) where they distributed ivermectin using 160,000 workers (who were all taking ivermectin prophylactically) that visited 97,000 villages, testing widely and treating all positive cases with ivermectin and prophylaxing all family members of positive cases with ivermectin. This is the graph of cases that resulted in Uttar Pradesh:
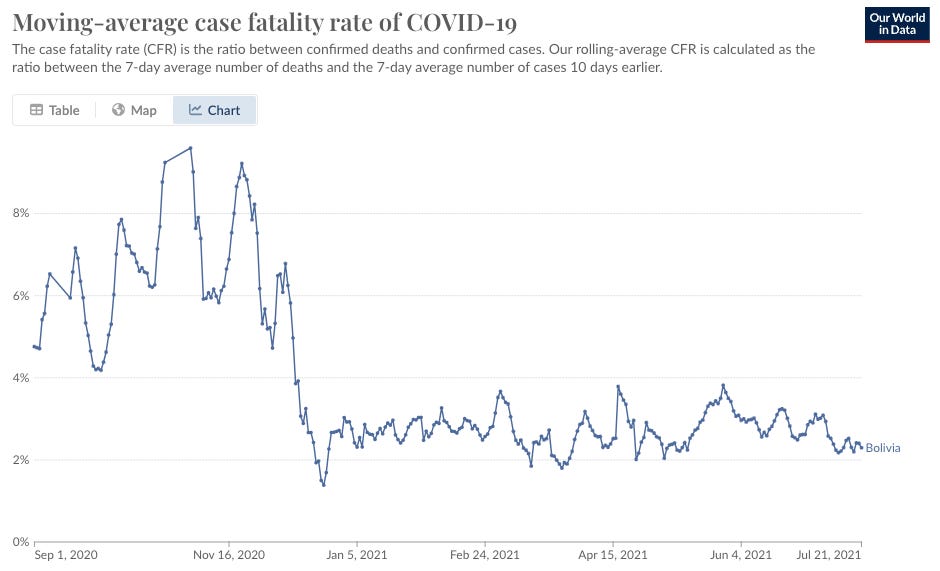
Another graph that one of my subscribers just sent me is this one:
Next, the below article highlights the fact that the first city to adopt chlorine dioxide in a coordinated program, San Jose De Chiquitos, found that their program led to “epidemiological silence” for 39 straight days at the time the article was published on Nov. 8, 2020:

Bolivia, with a population of 11.6 million people and a health expenditure of 11.52% of its budget (2017), according to Datamacro Expansion, has had fewer than 100 daily Covid-19 cases in November. While Costa Rica, with a population of 5 million people and a health expenditure of 26.91% of its budget (2017), has had more than 850 daily cases of Covid-19 in November.
As can be seen in the tables of daily variation, the Bolivian curve has managed to flatten, a goal that no other country in America has yet achieved.
Bolivia’s performance in combatting Covid with chlorine dioxide, like Uttar Pradesh’s performance with ivermectin, did not go unnoticed by the WHO. Recall this report from the WHO that celebrated Uttar Pradesh’s success without mentioning their systematic use of ivermectin! Same thing happened with Bolivia - the below WHO report on Bolivia’s success also somehow did not see fit to mention the nation’s use of chlorine dioxide. Curious no? See below, translated awkwardly by Google:

From above:
“In the last three months, Bolivia has experienced a significant reduction in cases and deaths from COVID 19 per 100,000 inhabitants compared to neighboring countries such as Argentina, Chile, Paraguay, Peru and Brazil, which have remained at levels 2 to 4 times greater and even increasing its progression,” said Auza.
Now, one of the most compelling and sincere testimonials regarding the efficacy of chlorine dioxide against Covid was this below testimony by a Mexican surgeon who treated three thousand patients with 99.6% success (4 deaths out of a 1,000).
In addition, he was forced to treat the patients at home and not at his clinic, because he claims that when they were reporting the near 100% effectiveness of chlorine dioxide, he says the “authorities” came and closed down the Covid unit of his clinic.
He was then forced to individually treat patients in their home without his medical staff to support him or the patient. I excerpted this clip via “fair use” from the documentary “The Universal Antidote.” Please watch:
He ends with:
“I know that I have seen thousands of patients getting better with this treatment and I will never stop using CDS (chlorine dioxide solution) in the treatment of Covid-19, no matter what.”
Now, just for kicks, I sent the above video to a friend and colleague of mine who is a world expert in detecting “deception” or “dishonesty.” His name is Louis Conte and besides being the guy who recruited me to SkyHorse publishing to write my book The War on Ivermectin, he is also considered one of the world’s experts at polygraph testing. However, know that polygraph data analysis is only one tool he uses in determining truthfulness, the rest relies on the voice, facial expressions/movements, mannerisms, tone, speech, etc.. Check out his assessment of truthfulness after I asked him to watch the video and comment:
I listened and watched again. I read him as being truthful.
His facial expressions line up with the underlying emotions of his statements, and there is no facial expression that I saw that was discordant.
I did not observe any increase in blink rate or indicators of dry mouth (licking lips, words, getting stuck or reaching for water to hydrate). These would be indicators of the fight, flight, freeze response.
I read him as being an honest doctor.
Poor bastard.
(Ed: I laughed out loud reading the last line… until I remembered it’s not funny :)
CONCLUSION
I have spent many weeks researching numerous aspects of chlorine dioxide and, in my opinion, I believe there currently exists a “wealth of evidence” of its safety and effectiveness against a broad array of microbes including viruses, bacteria (even multi-drug resistant), parasites, and fungi. Its efficacy in a broad range of non-infectious diseases also appears promising and I will be sharing evidence of that in future posts.
I now believe, like ivermectin, HCQ, nitazoxanide, and DMSO, chlorine dioxide should be a critical component of the medicine cabinet of every family’s household that is intent on preserving their health against future viral and/or bioweapon pandemic assaults.
If it is a living organism making you ill, I believe there is likely a single effective treatment for it and that is chlorine dioxide. To prove that, a lot of work needs to be done to overcome the regulatory barriers on research, however I have joined a promising international group of clinicians and researchers who are all collaborating on this mission. More will be revealed (I hope).
If this post whet your appetite for learning more about chlorine dioxide, please subscribe because my next posts will contain more detailed and referenced information on its safety and efficacy, as well as how to source and use chlorine dioxide in treatment of infectious (and other) diseases.
Ed Dowd uses a term quite often and it is A TELL. (especially in poker) an unconscious action that is thought to betray an attempted deception. From Ivermectin to HCQ to Chlorine Dioxide, whenever a Government Medical Authority and the MSM comes out against it ( THE TELL) you can be confident the product in question works quite effectively.
The effectiveness of simple remedies is likely proportional to how strenuously they are opposed by “authorities” as they desperately cling to their own inflated self- importance even at the cost of life and limb to their “subjects”.