The Safety Of Orally Ingested Chlorine Dioxide At Commonly Used Treatment Doses
Contrary to the edicts of regulatory agencies worldwide that chlorine dioxide is "bleach," "bleach-like," or a "poison," numerous studies show the safety of oral ingestion at treatment doses.
Due to the history of persecutions and attacks on researchers and practitioners of chlorine dioxide as a therapy, I have to emphasize that in these posts, my intent is not to recommend treatment via oral ingestion of chlorine dioxide because;
It is not FDA approved for oral ingestion to treat any disease
It is not approved as an orally ingested therapy by any other regulatory agency in the world.
It is not classified as a food supplement.
Further, no chlorine dioxide formulation product on the market either meets or has been evaluated in terms of quality and safety for oral ingestion and thus do not meet Good Manufacturing Practice (GMP standards. Also, even if the over the counter products are relatively safe, it is doubtful that people know how to correctly make or store the resulting solution. For instance, it must be mixed with distilled water and be kept out of sunlight in amber glass or plastic bottles (never metal!). Further,(when exposed to sunlight there is a chance that chlorine can be produced, something that can introduce the potential for harm).
Thus, it would be illegal and irresponsible for me to recommend treatment via oral ingestion with it, despite the fact that numerous over-the-counter products for mucosal or skin applications have been allowed on the market (oral, nasal, sinus, and skin).
What is weird it that although it would be illegal for me or anyone to treat Covid with it, a law was passed in Bolivia in early Covid (over the strenuous objections of the regulatory health agencies) which allowed for the widespread manufacture and distribution of chlorine dioxide to be taken by oral ingestion by the military and universities there (albeit under controlled and standardized processes). Millions of Bolivians thus were treated with oral ingested chlorine dioxide for Covid. This effort, I believe, is the reason Bolivia’s outcomes in Covid were the best in South America, something I covered in a prior post on chlorine dioxide here.
I thus view my work here as more in the vein of an amateur investigative science journalist who is exploring and exposing numerous troubling anomalies and contradictions in the behaviors and recommendations of regulatory agencies in regards to chlorine dioxide. It is my hope that this work helps provide the data in order to lift current FDA restrictions of research into oral ingestion of this promising compound. Todays post deeply illuminates only one such contradiction but there are more to follow. Subscribe now so as not to miss upcoming and critically important posts on this topic.
SAFETY OF ORALLY INGESTED CHLORINE DIOXIDE
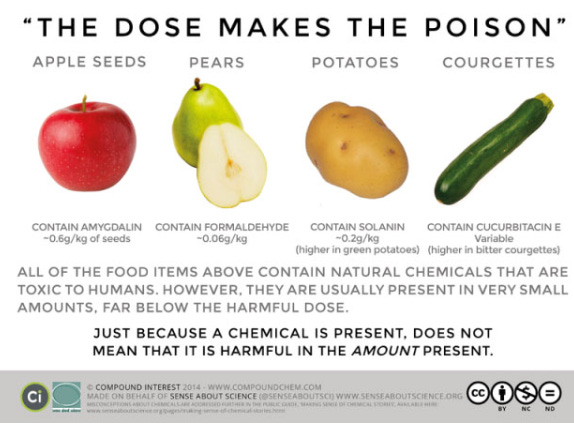
From ChemicalSafetyFacts.org: Nearly 500 years ago, Swiss physician and chemist Paracelsus expressed the basic principle of toxicology: “All things are poison and nothing is without poison; only the dose makes a thing not a poison.” This is often condensed to: “The dose makes the poison.” It means that a substance that contains toxic properties can cause harm only if it occurs in a high enough concentration.
In other words, any chemical—even water and oxygen—can be toxic if too much is ingested or absorbed into the body. The toxicity of a specific substance depends on a variety of factors, including how much of the substance a person is exposed to, how they are exposed, and for how long.
When the topic of oral ingestion of chlorine dioxide is discussed, “authorities” such as the FDA, EMA, TGA, PAHO/WHO and many (if not all) others around the world do not recommend the use of chlorine dioxide via oral ingestion at all, instead they call attention to the toxicity and danger of chlorine dioxide, but they never clearly indicate either the dose or administration route when chlorine dioxide is toxic. This is shocking because humans across the world regularly ingest chlorine dioxide due to the fact it is widely used in water purification.
Further, they often refer to the pure and concentrated form of this gas and not to aqueous chlorine dioxide solution used in treatment protocols for various illnesses.
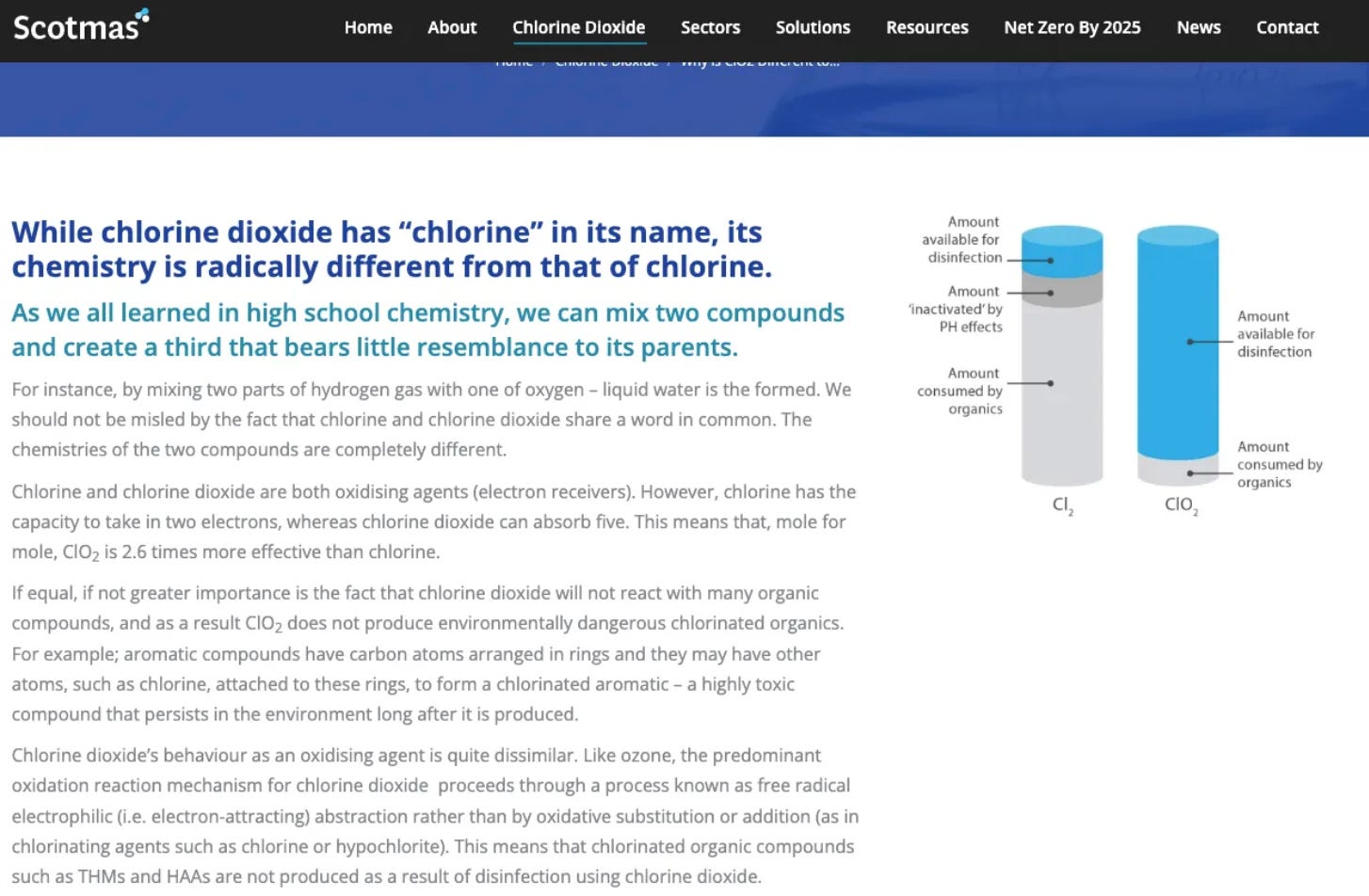
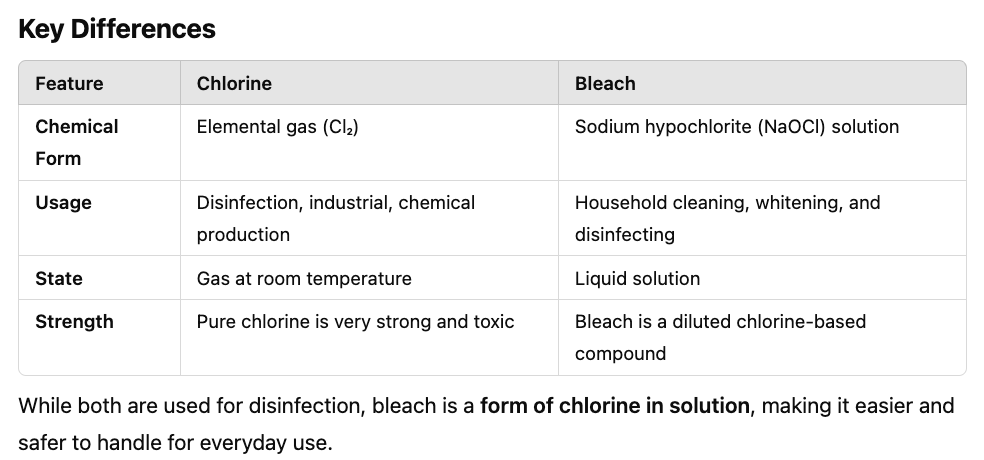
They also often refer to it as a “bleach-like” substance even though it is chemically very different from bleach (bleach is sodium hypochlorite). Sodium chlorite (which makes chlorine dioxide) is widely used for water purification; in higher concentrations, it is used in textile mills to bleach fabrics. Unlike sodium hypochlorite or Clorox (bleach), chlorine dioxide does not harm fabric.
Please read this concise comparison of the two compounds from Scotmas.com:
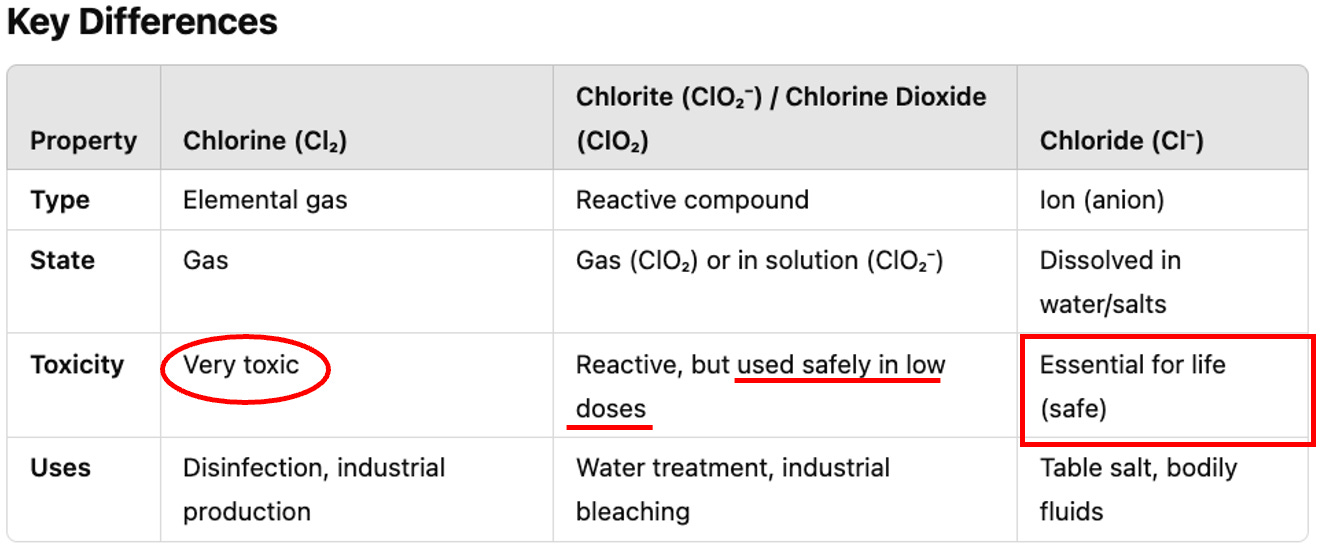
I want to further distinguish between the properties of chlorine, chloride, chlorate and chlorite as they are related but very distinct forms of the same element. Chlorine (the active ingredient in bleach) is a neutral atom with 17 protons and electrons, existing naturally as a diatomic molecule (Cl₂). Chloride, on the other hand, is the anion form of chlorine, which has gained an extra electron, giving it a negative charge (Cl⁻). This difference in charge is the key distinction between the two. Chlorine is a strong oxidizing agent used in various industrial applications, while chloride ions are essential for many biological processes and are found in compounds like table salt (sodium chloride). The most important fact you need to know about the chemical differences is that chlorine dioxide breaks down into the ubiqutious, essential, and safe compound of chloride, it does not produce chlorine!
What about chlorite? Well, chlorite (ClO₂⁻), like chloride, is also a negatively charged anion formed by the combination of 1 chlorine atom (Cl) and 2 oxygen atoms (O₂) and is used as the precursor to make chlorine dioxide. Chlorine dioxide, once formed, will also break back down back into chlorite and then further break down into chloride (no chlorine is produced at anytime, unless exposed to full sunlight). See table from Chat Gpt:
For those who are concerned about the potential for the breakdown product called “chlorate” to be toxic, know that chlorate does not break down into chlorine, instead, depending on methods or conditions, it quickly breaks down into the safe byproducts above of either 1) chloride and oxygen, 2) chlorite or chloride, and 3) chlorine dioxide (in acidic conditions).
I think it is really important to understand that when we are discussing the safety or efficacy of chlorine dioxide, it must be understood that chlorite (the precursor of chlorine dioxide) has also been shown to be a complex immunomodulator, capable both of enhancing the immune response through phagocytosis or cellular defense mechanisms, and of mitigating the effects of the inflammatory response, inhibiting certain cytotoxic effects, as well as the hemolytic effects caused by free hemoglobin and the heme group. Recall from my last post on the therapeutic mechanisms of these compounds that when chlorite is ingested, it can convert into an intracellular form of taurine chloramine (TauCl). TauCl is a long-lived effector molecule within macrophages that down-regulates NF-kB expression and inhibits production of pro-inflammatory cytokines in part through activation of heme oxygenase-1 (HO-1).
So, I am going to suggest that when we assess over-the-counter formulations of chlorine dioxide like MMS, know that they contain sodium chlorite, and that the chlorite itself has therapeutic mechanisms along with chlorine dioxide.,
We good with the chemistry class today? And more importantly, are we good with recognizing that the FDA (and their mass media partners) willfully and repeatedly misrepresent both the chemical nature and toxicity of this compound? If you aren’t convinced yet, you will be by the end of this post, so hang in and hold on.
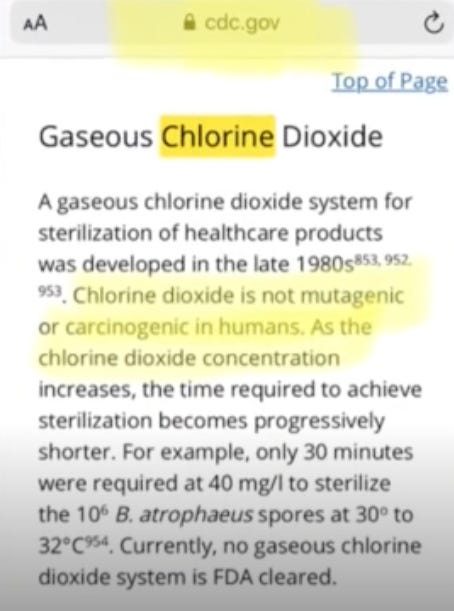
We should also tell the FDA that the CDC says that gaseous chlorine dioxide is not carcinogenic or mutagenic (unlike the breakdown products formed when chlorine (which is in bleach) reacts with organic matter, two of which are both mutagenic and carcinogenic):
Now, in order to assess the safety of orally ingested chlorite or chlorine dioxide solution, one must first understand how to measure doses which are sometimes expressed in weight (mg) or in concentration in solution (ppm). For chlorine dioxide, 1mg dissolved in a liter = 1ppm. In this review I will detail doses both in weight and concentration (the latter is determined by the volume the dose is dissolved in), however know that toxicity levels calculated by regulatory agencies are based on daily ingestion via weight, not concentration.
Some general statements before we go forward:
Chlorine dioxide is used in many industries such as municipal water purification, decontamination of food and beverages, pharmaceuticals, agriculture and as a disinfectant of both surfaces and of medical devices. Chlorine dioxide tablets are sold in camping stores for outdoor enthusiasts to purify groundwater in the wilderness.
The EPA has registered ClO2 as a “pesticide” [i.e. antimicrobial] due to its ability to eliminate microorganisms such as bacteria, viruses, and parasites from surface water, thereby rendering it safe to drink (EPA, 2006)
As a result, it is an inarguable fact that many Americans routinely ingest safe doses of chorine dioxide in their normal daily activities.
Now, before we explore the studies examining the safe dosing levels of chlorite or chlorine dioxide that can be ingested each day, I want to point out that the dreaded chlorine (as above and which is the main component of bleach) is also used in water purification. Wait, what? We are allowed to drink bleach? In a sense, yes.
What is the difference between chlorine and bleach? Easy - chlorine is a gas, and bleach is formed when chlorine gas is dissolved in solution, thus “bleach” is a liquid form of chlorine (technically the chlorine is in the form of sodium hypochlorite, not sodium chlorite as that turns into chlorine dioxide which sodium hypochlorite does not).
From Chat GPT:
The EPA has set the maximum allowable level of chlorine in drinking water at 4 milligrams per liter (mg/L), or 4 parts per million (ppm). For a human drinking 2.5 L. a day, this would mean that 10mg doses of chlorine are safe for daily human consumption.
The World Health Organization (WHO) has established a health-based guideline maximum value of 5 mg/L for chlorine as a residual disinfectant in drinking water. However, most water companies aim to keep the level below 1 mg/L. Either way, the WHO is saying that for 2.5L of water intake a day, 12.5mg of chlorine can be safely ingested on a daily basis.
OK, so the EPA and WHO are saying that there are safe amounts of bleach that we can ingest daily and the doses range between 10mg and 15mg daily. Remember those doses. Now I have to ask the question as to why the FDA and other regulatory agencies across the world are always “screaming” to chlorine dioxide practitioners that they are ingesting bleach, while ignoring the fact that bleach is apparently safe to drink chronically. Weird no?
Lets start looking at safe doses of chlorite and chlorine dioxide (recall that chlorite is the precursor to chlorine dioxide (as well as a breakdown product of chlorine dioxide).
IS 2MG PER DAY OF CHLORINE DIOXIDE SAFE TO DRINK?
In this terrific review paper by Dr. Michell Brent Liester, a chlorine dioxide expert at the University of Colorado, he reported that the EPA has established a maximum limit for chlorine dioxide of 0.8 ppm (0.8mg/L) when used as a water purifying agent in municipal water treatment plants. Know that the USDA recommends that men, on average, should drink 2.7L a day and women 2.2L a day. Thus, drinking 2.5L of water a day, that would mean that 2.0 mg is a safe dose to ingest on a daily basis (know that under certain conditions like heat and exercise, water intake is much higher thus the safe dose is likely over 3mg daily.) Isn’t this weird, that the EPA says we can drink chlorine at doses up to 10mg a day, but the much much safer chlorine dioxide should be under 2mg a day on average. Hmm.
IS 5MG OF CHLORINE DIOXIDE SAFE TO INGEST DAILY?
In this WHO safety review, they write “The International Program on Chemical Safety (IPCS), based on data on chlorite, proposed an oral tolerable daily equivalent to 2mg/L (2ppm) a day for a 70 kg male taken chronically over time, further supporting the fact that chronic exposure is well tolerated.” This indicates that, contrary to the EPA, the WHO has found that (again, assuming a daily intake of water at 2.5L a day) a total daily dose of 5mg of chlorine dioxide is safe to drink chronically. Caveat - here they are establishing the safe level of chlorine dioxide based on the dose of chlorite which is what turns into chlorine dioxide.
So, ingesting up to 5mg a day of chlorite is considered a safe dose by regulatory agencies for “chronic ingestion,” agreed?
IS 6.5MG OF CHLORINE DIOXIDE SAFE TO INGEST DAILY?
In this study, they gave a half liter of water with 5ppm (5mg/L) to healthy volunteers who drank it for a 12 week period, which “was accompanied by no clinically important physiological effects.” In their conclusion, they establish that this level is safe for “chlorine dioxide and its byproducts.” Thus, this study found that a daily dose of approximately 2.5 mg a day a day for 3 months is safe (if someone drinks 2.5L a day, that would mean a daily dose of 6.25 mg.
IS 10MG OF CHLORINE DIOXIDE SAFE TO INGEST DAILY?
The EPA also approved a limit of 4 ppm (4mg/L) of chlorite for emergency drinking water, which involves disinfecting surface water in emergency situations like while backpacking or camping or by emergency personnel. Again, assuming 2.5L of water intake a day, this would mean that for short periods, one could ingest 10mg a day safely (so, now we are at the same safe level that the WHO has established for chlorine in solution (i.e. bleach).
OK, so now we are up to 12.5mg daily doses of chlorite likely being safe for up to 12 weeks. Should we keep going higher?
IS 24MG OF CHLORINE DIOXIDE SAFE TO INGEST DAILY?
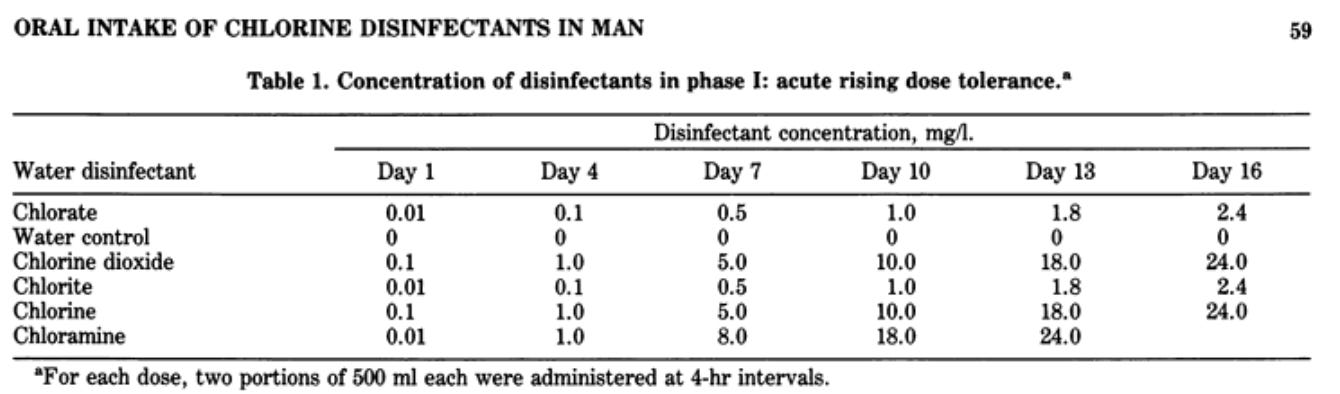
In this study by Lubbers et al from 1982, they had volunteers drink a liter of water a day of chlorine dioxide with increasing concentrations over time. They allowed two days for observation before increasing the next daily dose. They increased up to a dose of 24 ppm (24mg/L) in one day and observed no ill effects. Thus 24mg doses are safe to drink in one day.
Know that in this study, they actually put a number of disinfectants in the water at the same time. For instance, if you look at the Day 16 doses on the far right of the table, you see that not only 24mg of chlorine dioxide was safe, you could do that along with 24 mg of chlorine, 2.4 mg of chlorite, and 2.4 mg of chlorate. Wow!
From the paper:
IS 224 MG OF CHLORITE SAFE TO INFUSE INTRAVENOUSLY?
In this ALS study, they treated patients with chloriteintravenously (recall that chlorite is the active ingredient in the popular over the counter formulation called MMS and that chlorite turns into chlorine dioxide when exposed to something acidic). In that study they reported that 2mg/kg/day doses of chlorite for 5 days in a row (then 3 days in a row on a monthly basis) was well tolerated. Thus, for a70kg male, you could take IV chlorite at doses of 140mg a day.
In another ALS study, they gave chlorite intravenously at doses up to 3.2 mg/kg/day (i.e. 224 mg per day for a 70kg man) and that such doses were “generally safe and well-tolerated, with no serious adverse events observed.” So, 224mg a day of intravenous chlorite was well tolerated.
I think it goes without saying that Iv administration will produce far great absorption than oral administration, so the dose limits of IV administration suggest that far higher doses can be tolerated orally. At the risk of foreshadowing, know that 30mg in a liter of chlorine dioxide solution (CDS) daily is the dose targeted in the most popular, initial treatment protocol using CDS. In the above study in ALS, they gave patients many times that dose, but in the form of chlorite.
Anyway, let’s keep going with trying to understand the safety of treatment doses of chlorite and chlorine dioxide. In the below, we will explore the dose levels established by regulatory agencies that cause toxicity or lethality. Are treatment doses of the oral ingestion treatment protocols below that level?
While you’re here, don’t forget to subscribe for more posts like this one.
THE ESTIMATED LETHAL DOSE OF INGESTED CHLORINE DIOXIDE
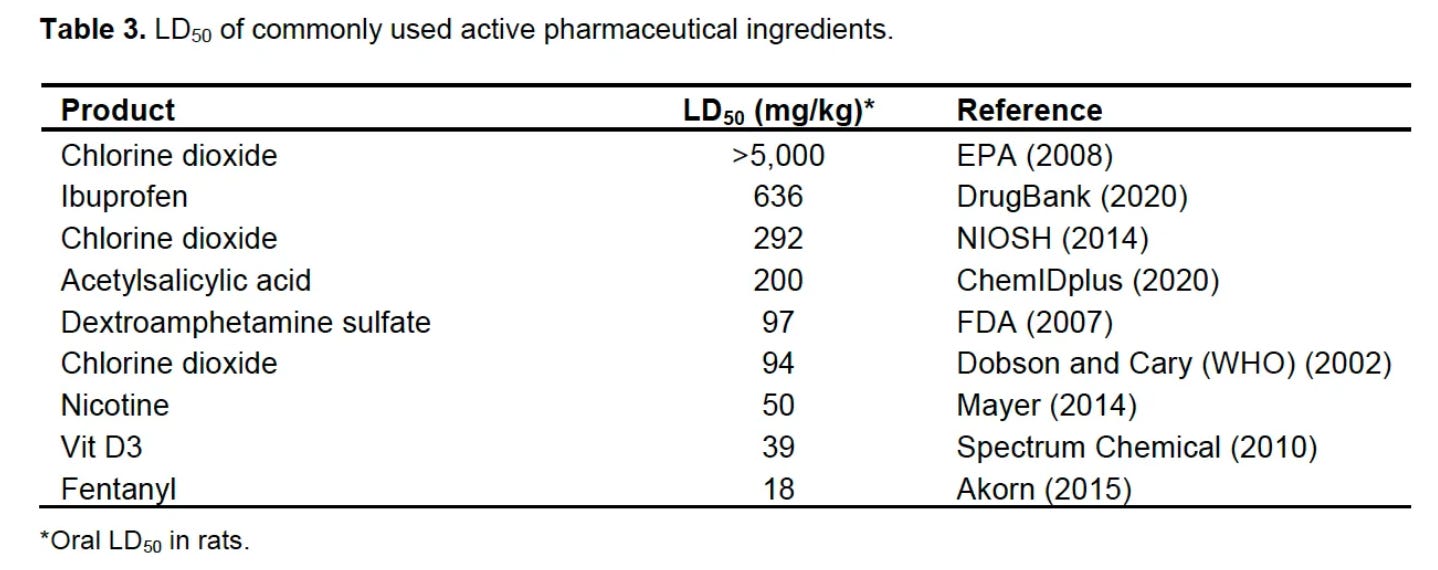
One method for determining toxicity is to assess a product’s “LD50” which is the dose required to kill half the test population. Obviously, we don’t do such tests in humans so the most commonly used test population is rats. **Note that in the below toxicity studies, the amounts of chlorite and chlorine dioxide that is tolerable via oral ingestion is measured in milligrams per kilogram, either per single dose or per day.
The WHO reported the LD50 for oral chlorine dioxide in rats to be 94mg/kg, which falls between the LD50 of 50 mg/kg for nicotine (Mayer, 2014) and 97 mg/kg for dextroamphetamine (FDA, 2007). If you had 70kg rats :), that means you would need the rats to take a dose of 6,580 mg in order to kill 50% of them.
The National Institute for Occupational Safety and Health (NIOSH) reported the LD50 to be 292mg/kg. I won’t even bother calculating that dose for a 70kg rat. This level places it between the lethal level of aspirin and ibuprofen, two of the most commonly used medications in the world.
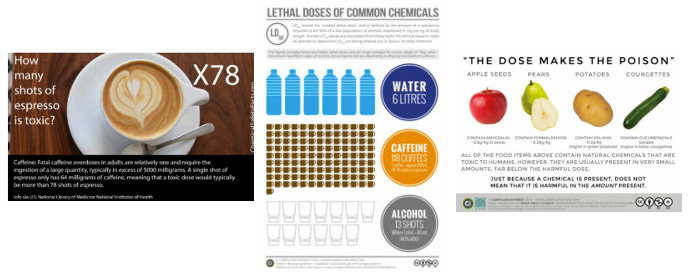
Let’s compare the LD50 of oral chlorine dioxide in rats to that of caffeine, where the acute oral LD50 is reported to be approximately 192 mg/kg, which suggests that caffeine is more toxic than chlorine dioxide. Other compounds far more lethal than chlorine dioxide in rats are nicotine and Vitamin D3. Interesting no?
SO, IF ITS LESS LETHAL THAN CAFFEINE, WHAT DOSE OF CHLORINE DIOXIDE IS TOXIC TO INGEST ORALLY?
Given the above data, it is nearly impossible to kill someone with chlorine dioxide (outside a massive intentional overdose) so what are the sub-lethal toxicity levels?
In a toxicological review issued by the US-EPA in 2000, experimental data, primarily from animal studies, were reviewed. Successive reviews, ultimately based on a long-term toxicity study commissioned by the EPA, including several generations of mice (which are particularly sensitive animals during estrus, lactation, and childbirth) led the EPA and later the U.S. Department of Health to determine the experimental toxicological levels for chronic oral exposure (>90 days) of humans to chlorine dioxide and chlorite. These levels are:
NOAEL: This EPA report identified a NOAEL of 3 mg/kg per day of chlorite based on observed nasal lesions at higher doses. For a 70kg human, that would be 210mg/day of chlorite, but remember, that would not be just one day, but taken chronically over time). I must recognize that in these rat studies, they evaluated the toxicity of chlorite, not chlorine dioxide, but, as per the report:
“The available data suggest that chlorine dioxide and chlorite have similar targets of toxicity and potencies. Therefore, the toxicity information for chlorite is relevant to deriving an RfD for chlorine dioxide.
LOAEL: 5.7 mg/kg/day (Lowest Observed Adverse Effects Level—the minimum dose at which some toxicity was observed). For a 70kg male, that would be 399mg a day chronically.
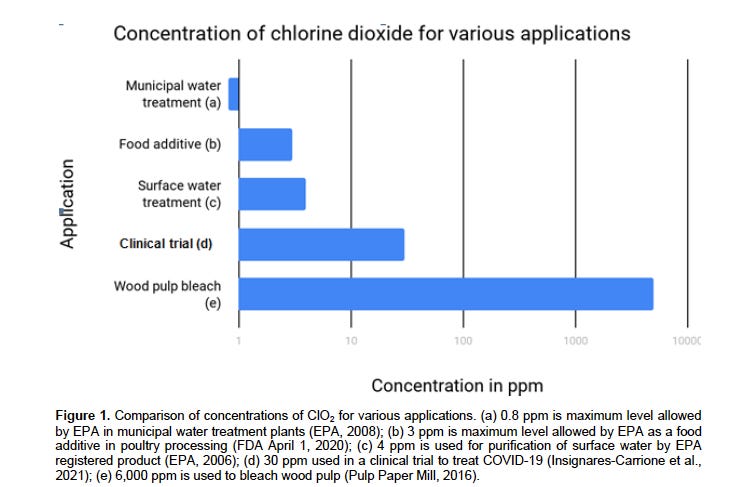
From the Liester review (see pdf), the chart compares concentrations in ppm, i.e. mg/L):
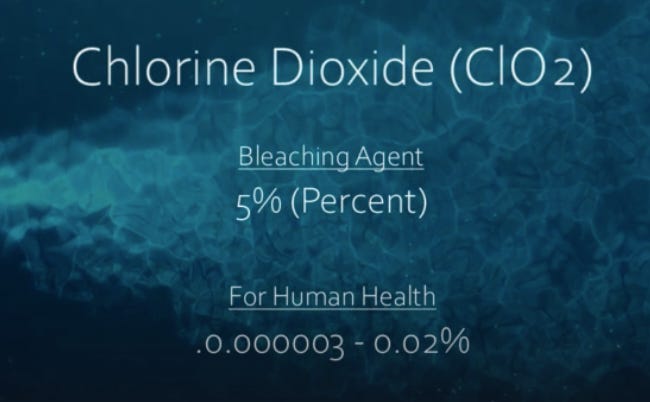
In “The Universal Antidote” (TUA) documentary, they provide a powerful illustration of the absurdity of the FDA and other regulatory agency claims by comparing the concentrations with which it is used as a “bleaching agent” in the paper industry and the concentrations with which it is used therapeutically in humans:
So, when chlorine dioxide is used as a bleaching agent (5% concentration), the amount would equal 50,000 mg per liter which is over 300X the maximum amounts (160mg/L daily) used in treatment via popular oral ingestiontreatment protocols.
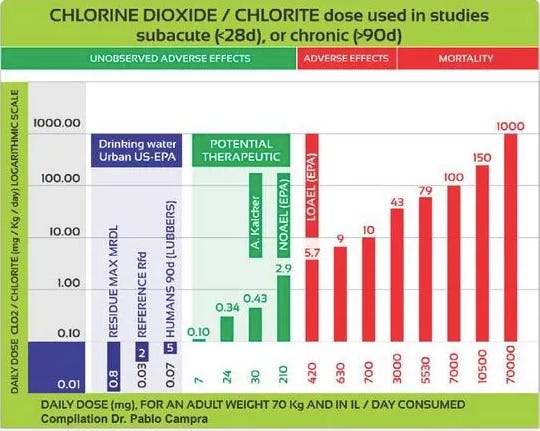
From this chart compiled by Dr. Pablo Campra (the bottom row shows the total daily dose in mg):
DOSES USED IN POPULAR TREATMENT PROTOCOLS ARE FAR LESS THAN TOXIC LEVELS
Thus, as per the previous section, the doses used in treatment protocols are far less than what has been established to produce adverse effects in chronic ingestion and nowhere near the levels used in industrial applications.
Now, I think it is important to understand the difference between Miracle Mineral Solution (MMS) and Chlorine Dioxide Solution (CDS) given they are the two main formulations of chlorine dioxide used to treat human diseases. These formulations differ by their method of production and the precision of estimated dosing levels:
Miracle Mineral Solution (MMS)
The original method pioneered by Jim Humble results in a compound he called “Miracle Mineral Solution” or MMS (his explicit rationale for calling it this will be covered in a later post). This original formulation involved simply ingesting sodium chlorite (NaCL02) water purification tablets or liquid, and then allowing our stomach acid to “activate” it into chlorine dioxide. (which dissolves in water and blood).
Since then, the method of preparation has changed, with the new formulation called “MMS1” where the chlorine dioxide is formed before ingestion instead of after ingestion. Making MMS1 involves combining equal drops of liquid sodium chlorite (NaCLO2) and a liquid acid activator (HCL) for 30 seconds prior then icing the drops with distilled water at 40z. . Since most protocols recommend hourly dosing up to 8 times a day, the MMS1 either needs to be mixed each hour (although it only takes seconds to prepare) or can be made in a larger volume for the day and ingested in hourly doses from a single container. The issue with MMS1 dosing is that only about 10% of the sodium chlorite is activated before ingestion, so some of the unactivated chlorite will then be activated by our stomach acid, thus increasing further the amount of chlorine dioxide available.
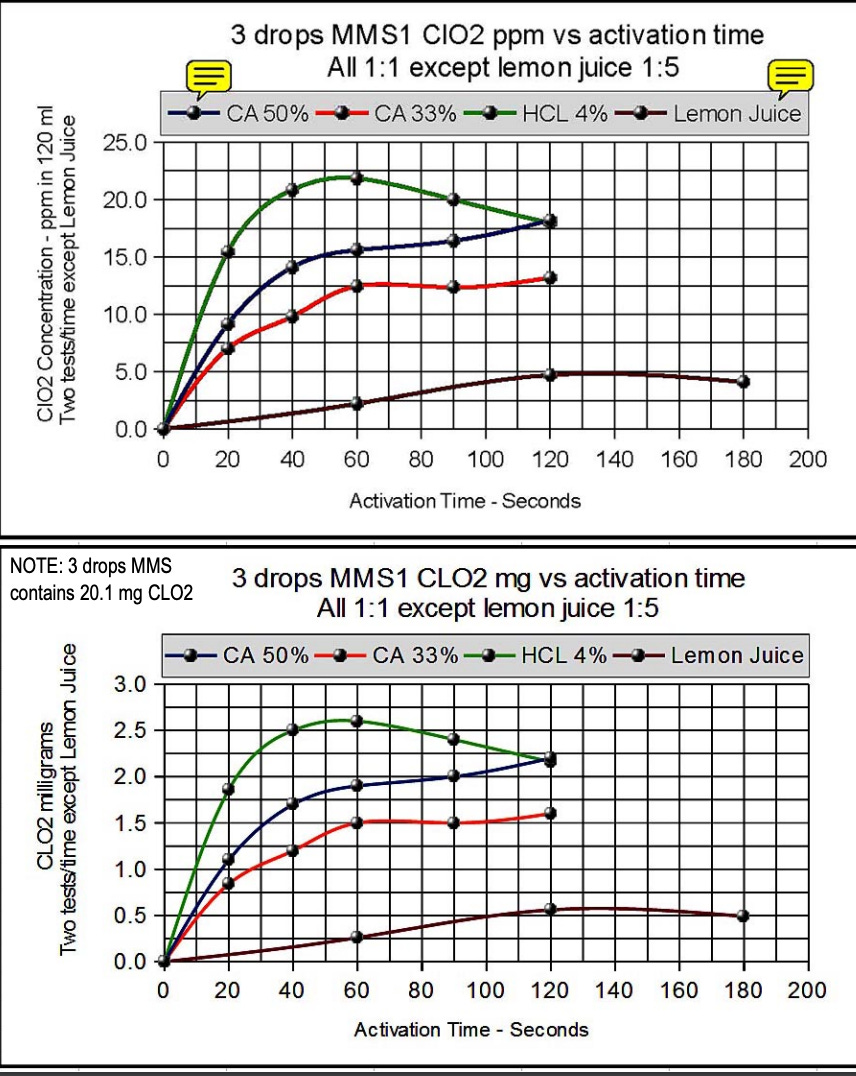
An anonymous scientist who goes by the name Charlotte (anonymity is prevalent by researchers in this field) and whose website on chlorine dioxide is terrific, employed spectral photometry (the only technique that can measure doses accurately). They found that 3 drops of MMS1 activated for 30 seconds produced a dose of 2.2 mg which when diluted in 1/2 cup of water (120ml/4oz) led to a concentration of approximately 20 ppm (20mg/L) (note that in the below, the amount produced after 30 or 60 seconds is not much different):
The above brings up an extremely important point about chlorine dioxide research. Given it is so heavily restricted, there are many questions that chlorine dioxide practitioners and researchers have not been able to answer reliably, mainly in terms of pharmacokinetics and pharmacodynamics.
Know that I am a newly inducted member of a group of expert chlorine dioxide researchers and practitioners which was named the “Bio-oxidative Research Task Force” where we meet weekly. Triggered by the groups review of a draft of this post, a fascinating discussion ensued which highlighted the knowledge deficits that still exist about the pharmacokinetics and pharmacodynamics of chlorite and chlorine dioxide.
Anyway, the discussion highlighted the fact that, since we do not have access to sophisticated measuring devices nor an affiliation with a research lab willing to undertake such research (career suicide), the exact dose of chlorine dioxide and its metabolites that are produced by current “over the counter” methods (MMS and CDS) are not precisely known and instead are roughly estimated.
We identified critical knowledge gaps that need to be filled for the field to proceed (wish us luck). Some of the first knowledge gaps are knowing the exact doses produced externally using the two most popular methods and then the doses generated and or absorbed internally by the body. This knowledge gap applies to both MMS1 and CDS formulations, but is probably more important to know for MMS1 given that this method involves ingesting a significant amount of unactivated sodium chlorite.
For instance, what happens after ingestion of MMS1? If only 10% is activated in the preparation glass by this method, how much will then be activated by stomach acid after ingestion (increasing the amount of chlorine dioxide absorbed) while at the same time the chlorine dioxide already produced will be reduced by interaction with tissues and/or pathogens into its metabolites like chlorite and chloride. What are their concentrations and how long are they active in the body?
Thus, you should know that with MMS1, it is impossible to know the exact amount of chlorine dioxide or its metabolites that are formed and/or absorbed with each dose. The main reason is that, as opposed to the decades of research into the pharmacokinetics and pharmacodynamics of topical applications of chlorine dioxide performed by the chlorine dioxide pioneer Howard Alliger and Frontier Pharma (more on him later), there is a paucity (but not absence) of similar research in regards to oral ingestion.
To do this research it would require complex studies using sophisticated methods of measurement due to the numerous variables which contribute to the amount of chlorine dioxide produced (and the amount of chlorite that remains or is metabolized into), e.g. the time allowed for activation before swallowing, type of acid activator (HCL most effective), the amount of stomach acid present, the temperature and pH of the components, and the amounts being mixed (not all droppers produce a standard “drop” - some droppers produce larger and some smaller).
So, although the actual amount of chlorine dioxide and chlorite that is produced by the MMS and CDS methods are not precisely known, in order to establish the safety of the MMS method for instance, one could simply calculate the maximum amount of chlorine dioxide that can be produced from 28% sodium chlorite. Those calculations can be found here and are briefly summarized by me below:
Assuming a maximal activation rate of 75% (i.e. the maximal amount sodium chlorite that can be activated), the maximal amount of chlorine dioxide that can be generated from 1ml (20 drops) of sodium chlorite and HCL is 125mg. Thus one drop produces a maximum of 6.2 mg. Humbles main protocol (“Protocol 1000”) calls for a maximum of 3 drops, 8 times per day which would equal a total of 24 drops. 24 drops times a maximum of 6.2 mg/drop= 148 mg a day. Now, recall that the No Observed Adverse Effect Level (NOAEL) for chlorite (equivalent to chlorine dioxide in terms of toxicity and potency) is 3 mg/kg/day, which for a 70kg person would = 210 mg a day. Thus, the maximum dose in Humble’s main protocol is far less than the NOAEL for a 70 kg person.
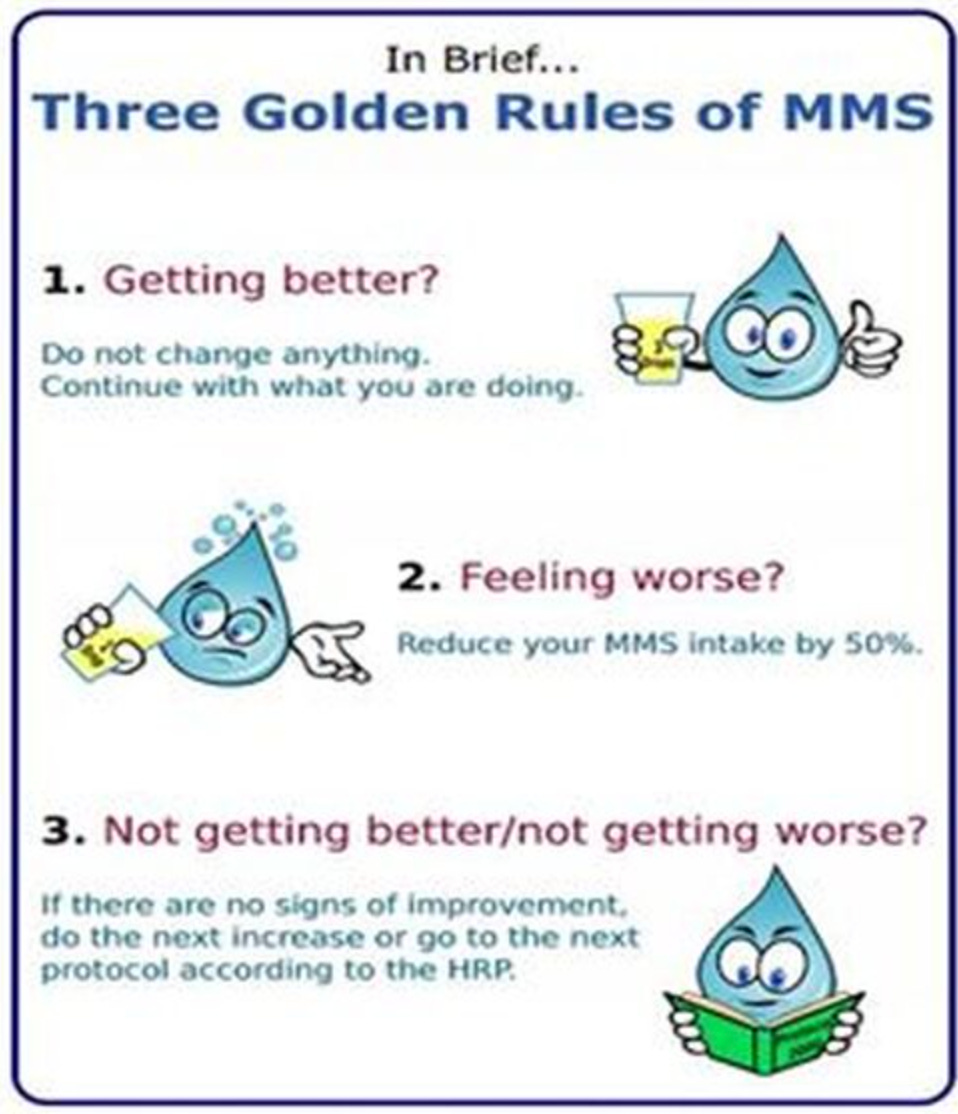
As a clinician however, I want to emphasize the unimportance of knowing the exact dose absorbed given that, as above, the dose ranges produced are far below levels producing adverse effects and, as long as a patient follows the “3 Golden Rules” of titrating MMS doses, the dose they arrive at will be safely tolerated and effective (as long as they prepare their MMS the same way with the same dropper each time).
Chlorine Dioxide Solution (CDS)
CDS was created by a group of scientists around 2007 who were trying to make “pure” chlorine dioxide solution by fully (100%) activating the sodium chlorite and HCL into a gaseous form. Similar to MMS, they combined sodium chlorite and HCL, but they did so in a closed container. Chlorine dioxide gas was created and then dissolved in distilled water, producing a solution which is now called CDS. The method is illustrated in Lesson 2 on the TUA website here.
Contrary to the claims by advocates of the CDS method, precise knowledge of the amount of chlorine dioxide in solution generated by this method cannot be attained without spectrophotometry. Using color coded “chlorine dioxide test strips” only allows for a rough estimate given that the color differences on the strips are not discrete - this method thus “estimates” the exact concentration but can be 2-3 fold off (however, again, to a clinician, this is not terribly important given the three golden rules of clinical dosing and the fact that any amounts generated will be far below toxic levels based on the amounts of sodium chlorite and HCL used).
Another variable which introduces imprecision is the fact that the geometry of the closed container used to generate the gas will affect the dose produced and those employing this method at home will not be using the same containers.
One purported strength of the CDS method is that a larger volume of solution can be easily created such that it can be dosed numerous times a day from the same container without having to mix each time like some do with MMS1. However, those who become familiar with making MMS1 can also easily make an “all day” volume of solution without having to mix each time.
Another supposed strength is that when taking CDS, there is no secondary activation in the stomach because there are no remnants of sodium chlorite and acid as occurs with MMS1, thus the ingested (not absorbed) dose is precisely known. However, this also introduces a “weakness” of CDS as a therapeutic - there is no additional sodium chlorite ingested, and, as above, chlorite itself has numerous therapeutic mechanisms.
Another difference is that CDS is said to have less of the chlorine smell and taste (which sometimes needs to be masked with something sweet or flavorful for patients with a strong dislike for the taste of MMS1). CDS is also considered to reduce the diarrhea reaction, in particular when used in higher doses, however, making CDS takes significantly more time and complexity than making MMS1.
Basically, both are considered highly effective, however, the chlorine dioxide pioneers, including Jim Humble, Mark Grenon, CM etc all prefer MMS1 both therapeutically and practically in most conditions for oral administration (for IV, IM, or enema administration, most would use CDS). For another comparison of the two formulations, I refer you to this post by Dr. Robert Yoho where he provides his reasoning for the preference of the MMS1 formulation.
DOSES USED IN POPULAR TREATMENT PROTOCOLS OF MMS AND CDS
So, if no toxicity of chlorine dioxide has been observed chronically for doses less than 210mg per day for a 70kg human, are the doses used in popular treatment protocols less than that level?
Again, Jim Humble’s main MMS1 protocol recommends increasing to a maximum of three drops of sodium chlorite with 3 drops of an acid activator per hour (referred to as a “3 drop” dose not “6 drop”). Per Charlotte’s measurements above, a 3 drop dose activated for 30 seconds = 2.25 mg. If one were to perfectly adhere to the main MMS protocol (Protocol 1000) and take this dose 8 times a day, this would approximate a total ingested dose of 18mg daily (note the “absorbed” dose of chlorine dioxide is likely higher than this due to secondary activation of chlorite by stomach acid and also know that the excess sodium chlorite ingested is therapeutically active by itself).
The main protocol for CDS relies on a making a solution of 3000 ppm (3000mg in 1L of water). But again, if measured using test strips, this amount is approximate and not precise. With this highly concentrated solution, they then take10ml out and dilute it in separate 1L of distilled water, thus making a solution of approximately 30ppm (30mg/L) which is then ingested over 10 single doses (i.e. a total of 30mg per day). It is advised to increase dose as tolerated by adding up to 30ml (of the 3000ppm solution) to 1L of water, making this approximately 90mg in a liter a day. It is advised against adding more than 60 ml (approximately 180mg in a liter per day).
From this report by the COMUSAV organization in October of 2020 (slightly paraphrased);
“The clinical experience of Latin American doctors over the past six months suggests that the intake of 30 mg per day of chlorine dioxide dissolved in one litre of water (e.g. 30ppm or 30mg/L), and drunk during ten events distributed over the day, is a successful treatment for COVID-19, which is 7 times below the dose considered as a NOAEL for a 70kg patient (i.e. 30mg daily vs. the limit of 210mg daily to avoid adverse events.
Further, from the Curious Outlier:
“I have done quite a bit of self experimentation with MMS1 and CDS and I have far exceeded NOAEL doses desiring to make sure I know that the things I am instructing on are well below any tolerable range. The worst symptom that I have ever experienced is mild nausea and diarrhea. When experimenting with MMS doses that were more concentrated above 50 ppm (50mg/L) it did occasionally give me a scratchy throat feeling. Very infrequently do I ever experience those symptoms with use now.”
Thus, the doses used in popular protocols are far lower than what has been established to produce adverse effects.
This is again where the whole “chlorine dioxide is bleach” propaganda argument falls apart. No-one anywhere in the world is using anything close to toxic or “bleaching” concentrations for anything to do with the treatment of human diseases. Plus, chlorine, the active ingredient in bleach, is often used for water purification and safe doses have been established for oral ingestion! Maybe tell that to all the TV News producers?
See this 5 minute “propaganda playlist” put together by The Curious Outlier in his The Universal Antidote Documentary (reproduced with permission).
In 2021, noted Mexican entrepreneur Pedro Luis Martin Bringas, associated with the Soriana Group, publicly pledged $2 million to anyone who could provide evidence supporting the claims of CDS toxicity at the commonly utilized dosages. He has also contacted the FDA but has not yet received any feedback.
REPORTS OF TOXIC INGESTIONS OF MMS
Now, despite the above, there have been 5 reports to the FDA Adverse Event Reporting System [FAERS] of adverse effects associated with the use of chlorine dioxide, and all 5 of these involved MMS.
It is clear to me and many of my network of chlorine dioxide experts that these cases are used by the FDA to warn against using MMS and similar products, stating “ingesting these products is the same as drinking bleach.”
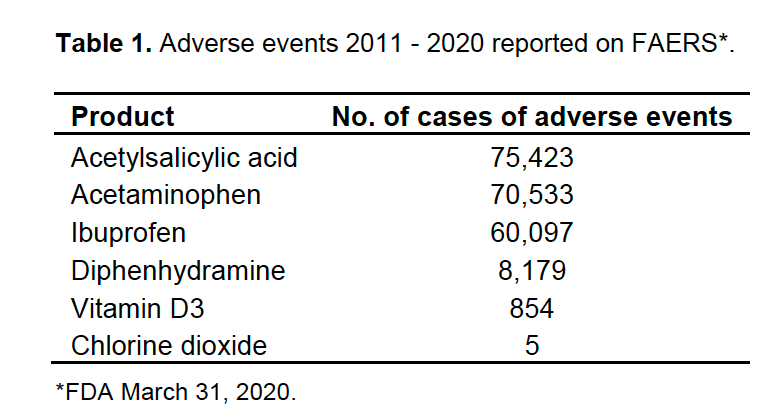
Which brings up the question, “How many reports of bleach ingestion have been reported to FAERS compared to the number related to chlorine dioxide ingestion?
This gets interesting, from Chat GPT:
So, the FDA collects and publicly reports data on adverse MMS ingestions but not bleach ingestions? Weird. It also gets a bit weirder, because Chat GPT then suggested I go to the below for data on bleach ingestion incidents:
Problem: I could not find these data on that website. Oh well, lets go back to the FDA’s FAERS system to review the reports on MMS ingestion:
From Liester’s review (edited for brevity):
The FDA has continued to warn against using MMS and similar products, stating “ingesting these products is the same as drinking bleach.” The FDA reports MMS “has caused serious and potentially life-threatening side effects” and describes reports of “severe vomiting, severe diarrhea, life-threatening low blood pressure caused by dehydration and acute liver failure after drinking these products” (FDA August 12, 2019).
Reports of adverse effects come from sources other than the FDA also. The Children’s Hospital of Philadelphia (2019) reported receiving 6 calls in 5 years related to MMS. The callers ranged in age from 3 to 48 years. One child experienced nausea and weakness following oral ingestion and the second experienced intestinal burns after being administered an enema that contained MMS.
The bias of health authorities can be seen in the purposely misleading headline of this report:
Adverse effects were also described in a case report of a 41-year-old woman who developed Kikuchi-Fujimoto disease [histiocytic necrotizing lymphadenitis] after ingesting an unknown quantity of MMS in a glass of water that was given to her by a relative. She was admitted to a hospital 11 days after the onset of symptoms which included fever, left-sided lymphadenopathy, chills, rigors, and a dry cough. An excisional lymph node biopsy was performed, and histological findings were consistent with Kikuchi-Fujimoto disease. She was treated symptomatically with paracetamol 1 g every 6 h for 72 h and she defervesced 16 days after the initial onset of fever. Outpatient follow-up at 2 weeks found no recurrence of fever (Loh and Shafi, 2014). (Ed: how is this in any way related to MMS?)
Stories in the media have also described adverse effects and death in people who ingested MMS. Several news stories reported the case of a woman who was sailing with her husband in the south Pacific in August 2010 when she suddenly became ill after drinking MMS. This woman developed nausea, vomiting, diarrhea, abdominal pain, and felt faint, then lapsed into a coma and died (Galli et al., 2016; New Zealand Herald, 2016; Ono and Bartley, 2016). Autopsy results were inconclusive (Gibson, 2010). (Ed: This case is clearly inconclusive as to the toxicity of MMS given lack of knowledge as to the illness she was treating and/or the dose she ingested).
A story in The New York Times reported the FDA had “received reports of at least 20 people affected by exposure to MMS, with at least seven deaths of people who had ingested Miracle Mineral Solution - two in 2018 and one each in 2017, 2014, 2013, 2011 and 2009” (Hauser, 2019).
However, a review of the FDA’s Adverse Events Reporting System [FAERS] Public Dashboard indicates as of March 31, 2020, only 5 reports of adverse effects were received, one each in 2011, 2014, 2017, and two in 2018. Furthermore, no deaths were listed (FDA March 31, 2020). (Ed: More disinformation from the New York Times).
High doses of ClO2 can cause methemoglobinemia. When ClO2 is added to water, chlorites are formed. High concentrations of chlorite ions oxidize hemoglobin to methemoglobin (Moore et al., 1978), and the ingestion of a high dose of ClO2 can result in methemoglobinemia. One example comes from the report of a 25-year-old male who ingested 10 g (ED: 10,000 mg or 10,000 ppm) of sodium chlorite dissolved in 100 mL of water during a suicide attempt.
He subsequently developed generalized cyanosis and respiratory distress and was found to be suffering from methemoglobinemia which also led to kidney failure. After receiving dialysis for 24 h, his methemoglobin decreased from 43.1 to 16.9%. Hemodialysis was continued for 4 weeks and after 3 months, renal function normalized (Lin and Lim, 1993).
Now, although someone like the man above who took 10,000 ppm (10,000mg/L) of chlorine dioxide has no relevance to the safety of short term use for acute illness at doses that are way less than established toxicity levels, the issue of G6PD deficiency should be examined. If patients with that disorder are particularly susceptible to methemoglobinemia, then maybe the established “safe” levels do not apply to such patients. Lo and behold, the answer is that safe doses have been established for such patients as well. To wit:
This study found that drinking water purified with chlorine dioxide did not affect patients with G6PD deficiency.
This study purposefully tested chlorite at a concentration of 5 mg/l (5ppm) daily for twelve consecutive weeks to a small group of potentially at-risk glucose-6-phosphate dehydrogenase-deficient subjects. No toxicity was observed.
Thus, G6PD patients should not be concerned at concentrations of 5ppm (5mg/L) for 12 weeks, and, outside of the intentional overdose case above and another case of a 1 year old boy who drank a chlorine dioxide household product, no other methemoglobinemia cases have been reported.
SAFETY OF TOPICAL APPLICATIONS OF CHLORINE DIOXIDE
There are dozens of research papers that extol the benefits and safety of topically applied chlorine dioxide for human wound management and microbial control. In 2014, the Journal of Advances in Skin and Wound Care published an article that stated,"Chlorine dioxide appears to be a safe, biologically acceptable, antiseptic wound irrigate that does not appear to interfere with cosmetic outcomes."
Know that the published paper contains a dosing error (personal communication with Frontier Pharma). Instead of 0.8% (8000ppm) as stated, Frontier Pharma informed me that their product’s concentration range is between 40 - 200 ppm, (far less than the 8000ppm in the paper which would not be tolerable as a rinse). The paper is still a testament of the safety and efficacy of chlorine dioxide, and in particular Frontier’s formulation (which is not just straight chlorine dioxide).
To show just how safe topical and mucosal chlorine dioxide is, know that Frontier Pharmaceuticals, the daughter company of Howard Alliger, the pioneering researcher of chlorine dioxide, sells an approved suite of oral, dental, nasal, and wound care products to treat bad breath, biofilms, acne, toenail fungus, canker sores, oral infections, and chronic sinus infections. One of the most popular products, the Snoot nasal/sinus spray, has about 20ppm when initially mixed which can then increase to about 80ppm before dissipating over a week (again, personal communication with Frontier Pharma).
At the risk of turning this into a commercial for their products (I have absolutely no financial relationship or incentives with the company), know that, per Frontier Pharma:
The Snoot formula provides the benefits of glycerin to moisturize and prevent irritation and mild wetting agents to help break up mucous. DioxiRinse contains calcium and phosphate to protect the teeth from etching, as well as menthol and glycerin for soothing and hydrating. It has a fresh, invigorating mint flavor. The products are “ready to use” and shelf stable for 2 years. These features separate our products from using straight chlorine dioxide alone. We are able to control the rate of reaction and generate known concentrations of chlorine dioxide with each use.
EFFECTS OF CHLORINE DIOXIDE ON THE HUMAN MICROBIOME
Now, many question whether, due to its broad anti-microbial properties, chlorine dioxide has negative effects on our own native microbiome. The chlorine dioxide experts I have talked to argue that this does not happen largely because the organisms that make up our microbiome, unlike pathogens, generate significant amounts of reactive oxygen species (ROS) which protect them from the oxidizing effects of chlorine dioxide. Further, one of the most important properties of chlorine dioxide is that it is known as a relatively “weak” oxidizer and that this property is what makes it so safe - it is too weak to kill our native microbiome but strong enough to kill pathogens. Wow.
In essence, the ROS generated by the gut bacteria (in particular lactobacillus) are protected due to the fact that 1) the ROS protects them by neutralizing the chlorine dioxide. It is felt that unless the chlorine dioxide doses are massive, the microbiome is not affected, although the exact dose which the microbiome is susceptible to is not known. It should also be noted that many people with chronic intestinal inflammatory or infectious disorders have reported significant improvements after oral ingestion of chlorine dioxide without side effects in the gut.
“Chlorine dioxide is a less powerful oxidizer than hydrogen peroxide. Hydrogen peroxide will oxidize many things that chlorine dioxide will not oxidize, and which makes chlorine dioxide an ideal oxidizer for the body. It doesn't have the power to oxidize the healthy cells of the body or the beneficial bacteria in the body or a lot of the tissues of the body. While hydrogen peroxide can oxidize a lot of things, chlorine dioxide oxidizes a very limited number of things. It will only oxidize pathogens. That's the things that cause disease in your body. It only oxidizes the pathogens. It won't oxidize any of the beneficial things in the body, so you don't really have to worry about it. “
Finally, although it is clear that doses used in oral ingestion treatment protocols are below the levels where adverse effects are observed when taken chronically, this does not mean that chlorine dioxide treatment is without some side effects. When using the MMS1 formulation, if patients use doses they have not yet developed tolerance to (i.e. increasing their dose too quickly), watery stools are common, nausea and vomiting may occur and fatigue is sometimes reported, particularly in older patients.
Mild “Jarisch–Herxheimer” reactions can occur (sudden and typically transient reactions from “die-off” of infectious pathogens after being administered anti-microbials). Symptoms include fever, chills, shivers, feeling sick, headache, etc. Humble feels such reactions are simply evidence that the “MMS is working.”
Either way, from my previous post where I detailed a recent illness that I suffered and that I self-treated with chlorine dioxide, I had decided to dose a bit more aggressively than most due to the severity of the illness. I myself found the side effects tolerable and were greatly eclipsed by the fact I recovered quickly.
If you appreciate the time and effort (and the personal and professional risks I am taking) in researching and writing on chlorine dioxide, support in the form of paid subscriptions is appreciated - Pierre
P.S I am again emphasizing that I am not recommending treatment with chlorine dioxide via oral ingestion to anyone as these posts are simply intended to help open and guide research into treatment of human diseases with this promising compound.
As someone who ingested oral CD for a year, following the protocol in Kerri Rivera's book, I find this article both sad and amusing. I got immense benefits from it, basically getting my life back after a long term severe (undiagnosed of course) toxic mold exposure along with FQAD from incompetent efforts to treat the undiagnosed CIRS. I don't know what it detoxed but my eyes actually changed color from more green to more blue, and I dumped amazing amounts of visible parasites. So I view the Bleach Screechers with scorn and label them trolls.





As someone who ingested oral CD for a year, following the protocol in Kerri Rivera's book, I find this article both sad and amusing. I got immense benefits from it, basically getting my life back after a long term severe (undiagnosed of course) toxic mold exposure along with FQAD from incompetent efforts to treat the undiagnosed CIRS. I don't know what it detoxed but my eyes actually changed color from more green to more blue, and I dumped amazing amounts of visible parasites. So I view the Bleach Screechers with scorn and label them trolls.
Amazing work Dr Pierre! Have needed this and am sharing everywhere.
Thank you for being a well informed humble man who cares about others. God bless you and your family ❤️🔥🕊️🛐