

The Evolution And Validation Of The Metabolic Theory Of Cancer
For the past 70 years the Somatic Mutation Theory (SMT) guided all research and treatment in cancer. Why are so few aware that it was overturned 15 years ago by the Metabolic Theory of Cancer (MTOC)?

In my last post of this series on cancer, I summarized the history of the scientific discoveries which led to the current consensus theory on the cause of cancer which is called the Somatic Mutation Theory (SMT). I concluded by presenting evidence from the Human Genome Project and The Cancer Genome Atlas Project that emerged in the last 15 years which paradoxically, instead of confirming its validityy, instead contradicted it.
I suggest you read that first post on the SMT before delving into the current post which traces the history and evolution of the competing, and in my and other’s opinion, more scientifically valid theory called the Metabolic Theory of Cancer (MTOC). Please know that this post was highly informed by the amazing books by Travis Christofferson (Tripping Over the Truth or what I will reference below as TOTT), Thomas Seyfried (Cancer As a Metabolic Disease), and Siddhartha Mukherjee (The Emperor of All Maladies). I ask those authors for forgiveness if I mis-referenced or failed to reference statements made below as I wrote much of it from memory and notes.
My other cancer posts are:
The Prevailing Scientific Theory Of Cancer Has Been Overturned
The Scientific Basis For The Somatic Mutation Theory Is Invalid
If you have not read the previous posts, I will quickly review and summarize the conceptual foundation of the two competing theories so you can better understand this post.
SMT adherents believe that cancer arises solely from direct DNA damage, i.e. carcinogens cause mutations in the DNA contained in the chromosomes in the nucleus. These mutations then drive the cell to adopt “cancerous” properties, of which there are 8:
1. it stimulates its own growth
2. it evades growth suppressing signals
3. it resists cell death (apoptosis)
4. it enables replicative immortality
5. it induces the ability to grow new blood vessels to further tumor growth (angiogenesis)
6. it spreads to distant sites (metastasis)
7. it evades the immune system
8. it has a “reprogramming of energy metabolism”
Meanwhile, MTOC adherents believe that cancer results from injury to the mitochondria (the energy forming unit of the cell which is in the cytoplasm). They focus on the fact that all cancer cells, instead of using oxygen to make energy, rely on glucose for energy, something that occurs only when mitochondria are damaged.
Injured mitochondria then send signals to the nucleus which both disrupt the cell’s DNA monitoring and repair mechanisms as well as turn on genes which cause cancer (oncogenes). The main concept to understand is that MTOC researchers posit that unless there are damaged mitochondria, cancer will not result. SMT adherents largely ignore the role of the mitochondria in causing a cell to become cancerous and instead obsessively focus on the DNA mutations they find.
However, SMT adherents (i.e. all of modern oncology) really have no explanation for, nor do they address in a coherent manner the fact that all cancer cells predominantly utilize glucose for energy instead of oxygen. They think it a curious finding without importance, simply a “consequence” of cancer and not a cause.
This finding has always been a problem for the SMT (except if you ignore it as literally nearly all of modern cancer research does). What argues very strongly against SMT as the origin of cancer is the fact that the metabolic defect above is present in all cancer cells while mutations are not universal. Further, many different cancers can arise from many different mutations, and many cells within a single tumor can vary in the number and type of mutations. Hardly universal to the cancer cell.
However, up until the last thirty or so years, no-one knew why cancer cells universally relied on glucose instead of oxygen to produce energy.
HISTORY AND EVOLUTION OF THE METABOLIC THEORY OF CANCER
Where do we begin? Well, with Dr. Otto Warburg of course! Warburg was a German doctor and biochemist who started studying cancer in the 1920’s and ended up winning the Nobel Prize in 1931 for his discovery that cancer cells were unique in that they switched from using oxygen as their primary source of energy to almost exclusively relying upon glucose, a feature known as “the Warburg Effect.”
Know that the Warburg Effect is literally what PET scan technology is based upon and PET scans are the predominant imaging means that all oncologists use for diagnosing, monitoring, and identifying the location and/or spread of cancer. In PET scanning, the radiologist infuses radio-labeled glucose into patients who then undergo full body scanning which produces an image of the body where “bright spots” indicate areas of high glucose uptake, i.e. pinpointing the location of the cancer. Thus, PET scans literally identify cancer based on the Warburg Effect.
So, one might expect that oncologists readily acknowledge that cancer cells survive on glucose which would lead them to universally recommend a ketogenic diet to their patients (when a patient goes into ketosis after strictly following such a diet, the fuel available to cells is no longer glucose and instead they begin to burn fats called ketone bodies. Cancer cells (with some rare exceptions) cannot use ketone bodies for fuel and thus such an approach “starves the cancer cell” of energy and thus it dies off. Problem: I have had a number of patients tell me that when they asked their cancer doctor what they should be eating, they are told “whatever you like.” Hmm.
Warburg’s discovery led to a vexing question, “since metabolizing glucose to make energy is much less efficient than using oxygen, why would cancer cells, which require a lot of energy to behave cancerously, rely on glucose as an energy source even in the presence of oxygen?”
That is the question that Warburg was never able to answer in his lifetime. The other problem with Warburg’s discovery was that it somehow never gained a critical mass of researchers inspired to study it’s implications further. Scientists were somehow unmoved by the importance of the discovery, with one prominent one saying in 1928, “even if Warburg is right, it does not explain why cancer cells grow,” a criticism which remained throughout his life until he died in 1970.
Another missed opportunity for the cancer research community to revisit Warburg’s work was when Cyril Darlington in 1948 surprisingly found an anomaly of the SMT in that he discovered that carcinogens that were the most damaging to DNA were not the most effective at causing cancer (weird). X-ray’s gave the signal in that at low doses they caused chromosomal damage but did not cause cancer. At high doses they caused cytoplasmic damage (where the mitochondria are) and that was when they began to cause cancer. Darlington was the first researcher who came closest to highlighting the implications of this observation in regards to the Warburg Effect, however over time, his observations were somehow forgotten!
Then, in 1953, a discovery was made which further (but erroneously) cemented the SMT while pushing the MTOC further into oblivion. And that was when Watson and Crick made one of history’s greatest scientific breakthroughs - identifying the structure of DNA. After that discovery, most cancer research became almost singularly obsessed with the SMT or, as the National Cancer Institute (NCI) states “cancer as a genetic disease.”
Later, in 1976, the final blow to the MTOC was dealt when one of the world’s leading cancer researchers, Dr. Sydney Whitehouse, published an extremely popular paper where he claimed that there was no evidence that mitochondria in cancer cells had altered structure or function. He called the metabolic injury theory as being causative of cancer “too simplistic” for serious consideration given that no-one had found cancer initiation or survival by faulty respiration and high glycolysis.
THE METABOLIC THEORY OF CANCER SILENTLY GAINS TRACTION
Starting in 1979 and over the next 30 years, the work of a small group of researchers would culminate in the identification of all the pieces of the metabolic theory puzzle that Warburg had first uncovered.
First and foremost was Pete Pedersen in 1979. From TOTT, “as a cancer researcher, he felt almost alone in considering energy metabolism as important to the cancer problem.” His work eventually produced two major pieces of evidence for the MTOC:
He developed techniques to study the mitochondria and found that cancer cells had both a lower number of mitochondria but they also appeared different – they were smaller and had numerous structural abnormalities, missing membranes, and abnormalities in their protein and lipid content (contradicting Sydney Whitehouse’s 1976 paper above).
This brought up a paradox though - how does inefficient energy production from damaged mitochondria “help” a cell to be so “energetic” i.e. to now be able to divide uncontrollably, grow, spread, invade, resist apoptosis etc. It would be like building a race car with the faultiest, most inefficient engine you could find. Didn’t make sense.
Pedersen’s next discovery was his finding that that cancer cells contained large amounts of a rare form of an enzyme called hexokinase which controls how much glucose is metabolized by a cell (normally as glucose is metabolized, it inhibits hexokinase which then causes less glucose metabolism in a negative feedback loop). But Pedersen found that of the four forms of hexokinase, the rarest one was present in large amounts and that this particular form ignored the inhibitory signals and instead acted by essentially “flooring the glucose gas pedal.” As Christofferson wrote, “it was like a beat up old jalopy that has its gas pedal glued to the floor – so it can only run at break neck speed.” (a different car analogy :)
Pedersen also discovered that hexokinase affects the signaling for apoptosis (programmed cell death). Know that apoptosis is critical for life as the body must constantly renew, so billions of cells must die each day for billions to replace them. If apoptosis is inhibited, the cell begins to act cancerously.
Thus Pederson’s research into hexokinase ended up providing explanations for two of the characteristics that are universal to cancer cells, i.e. glucose metabolism and lack of apoptosis (recall that mutations are not universal to every cancer cell, and although mutations are very common, they often vary between cells of the same tumor so cannot explain why the cell is behaving cancerously).
Without jumping too far forwards, many of the repurposed drugs and nutraceuticals that we have been using at The Leading Edge Clinic in our complementary cancer protocols have signaling mechanisms which directly stimulate apoptosis. Even more importantly, the medicines we use do this selectively to the cancer cell (unlike chemotherapy which leads to indiscriminate killing of both healthy and cancer cells).
Pedersen dealt yet another blow to the SMT when he discovered that carcinogens that were better at damaging mitochondria were better at causing cancer than those that damaged chromosomes (building upon Darlington’s work above from 1948).
Pedersen also found that viruses can infect and use mitochondria. Recall that one of the theoretical pillars supporting the SMT came from Varmus and Bishop’s discovery that RSV could insert into DNA and cause cancer, a finding which further cemented the idea that cancer originates in the chromosomes. However, Petersen later found that RSV could infect the mitochondria of chicken cells! The “error” which led Varmus and Bishop’ss argument to prevail over Pedersen’s was the overlooked fact that many viruses are capable of causing cancer but not in the way RSV supposedly does.
Basically, the work of Pedersen and Darlington found that 3 common cancer transforming agents (chemical carcinogens, radiation, and viruses) could damage both the mitochondria and the DNA in the nucleus. So, based on the work of Pedersen, it remained to be determined which “damage” is more important in causing cancer?
So, although Pedersen took Warburg and Darlington’s work much further towards a coherent MTOC, unfortunately, as Christofferson wrote “the larger research community continued to ignore Pedersen’s work as being important or foundational.”
THOMAS SEYFRIED AND THE METABOLIC THEORY OF CANCER
Thomas Seyfried was a biochemist and geneticist who was a leading basic science researcher of a rare category of diseases caused by “gangliosides” (a category of fats found in cell membranes). Ganglioside diseases are caused by defects in the enzymes that break them down which causes them to accumulate and typically lead to death by the age of 4.
Around 2000, Seyfried was approached by a small drug company that had found a molecule that inhibited the formation of these gangliosides. While Seyfreid was doing studies on the molecule, one day he fortuitously decided to give it to mice with tumors. What he found was that it slowed the growth of the tumors! He informed the company who then became very excited because the potential market for their molecule went from minuscule to massive.
From TOTT: But Seyfried also noticed that the mice given the drug lost a lot of weight. So, again on a hunch, Seyfried did an experiment where they used a control group of mice that they forced to lose the same amount of weight. They found that the effect of the drug disappeared in that now both groups showed an equal reduction in the growth of the tumors! This is how he discovered that it wasn’t the drug working against tumors but it was the caloric restriction which occurred in both groups. The company was obviously disappointed and immediately pulled their funding of his research.
So, Seyfried discovered that caloric restriction slowed tumor growth. Here is where it gets scary. He hypothesized that current cancer drugs were working the same way, i.e. the patients receiving them may be simply eating less food from loss of appetite and that may be the mechanism behind the way they worked?
Lo and behold, he began testing known anti-cancer drugs and found many of them were indeed working this way, e.g. Imclone’s Erbitux, the drug from the Martha Stewart insider trading case). A quote of his from the time, “Many of these drugs were doing nothing but making the mice lose their appetites and it was the reduced calories that had the anti-tumor effect.”
From TOTT: He then “moved backward” by looking into the metabolism of cancer, despite never having heard of Warburg. He quickly discovered Warburg’s work which led him to Pedersen’s 1978 review which Seyfried referred to as a “masterpiece.” Then he found the work of Darlington. He also gave a lot of credit to Carlos Sonnenschein and Ana Sota who had compiled “a blistering attack “on the gene theory (i.e. SMT) of cancer, with their 1998 paper called The Society of Cells: Cancer and Control of Cell Proliferation, “they did a magnificent job of showing the inconsistencies of the gene theory.”
Although Pedersen discovered the metabolic reasons why cancer cells relied on glucose and also why cancer cells did not undergo apoptosis, in his words, he was still unable to “establish whether mitochondrial function is essential to transform a normal cell to a cancerous one.”
Seyfried then developed a hypothesis that mitochondria, when damaged, must be sending a signal to the nucleus which then altered the expression of cancer causing oncogenes (i.e. an epigenetic signal). Problem is that epigenetic signals are very difficult to study.
Know that mitochondria, besides creating the energy needed in order for the cell to survive, also regulates many other important functions like cellular division and differentiation, programmed cell death (apoptosis), heme and steroid synthesis, and iron metabolism. To perform these, mitochondria use signals to direct the nucleus all the time.
Also know that most of the genes in the nucleus that respond to mitochondria sit at signaling hubs and therefore dictate multiple operations such as cell division and angiogenesis (growth of new blood vessels). Seyfried termed this signaling from mitochondria back to the nucleus as the “retrograde response” and felt that if the mitochondria were damaged, it must be sending signals that allow for uncontrolled proliferation, (i.e. cancer) and he felt it likely did so by “turning off” the DNA repair mechanisms, thus allowing mutations to develop and the cell to become cancerous. In essence, he felt strongly that mutations in the DNA occurred downstream from mitochondrial damage.
How to prove this? It turns out, he didn’t have to because researchers had already done so in the 1980’s yet the world had paid little attention to their studies (heck the original researchers themselves did not understand the importance of their findings). It was Seyfried who dug up the studies and used their findings to essentially prove his hypothesis.
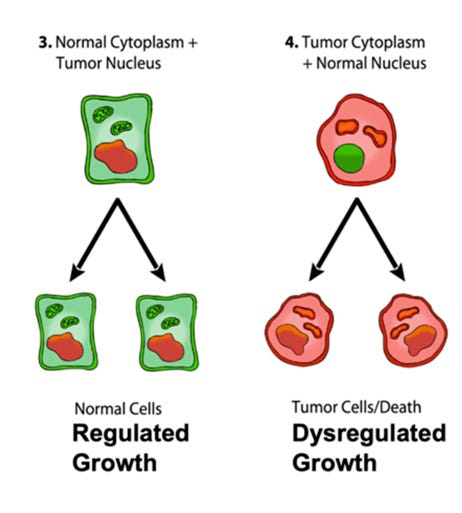
THE NUCLEAR TRANSFER EXPERIMENTS
What Seyfried discovered was that back in 1980, two different research groups (one at the University of Vermont and the other at Texas Southwestern), performed a series of technically simple experiments whose results held profound implications to proving the metabolic cause of cancer.
Briefly, what the group in Vermont did was they took the nucleus of a cancer cell and transferred it into a normal cell whose nucleus had been removed (something Warburg could never have done in the 1920’s). They called this cell a “recon” (reconstituted) cell. If mutations to DNA caused cancer then the recon cell which now had a nucleus from a cancer cell should become cancerous no? Conversely, if mitochondria were the proximate cause of cancer, the normal mitochondria in the recon cell should then prevent it from behaving cancerously.
So what did they find? Recon cells were transplanted into sixty-eight mice and they found that only a single mouse developed cancer over an entire year. The healthy mitochondria must have “silenced” the mutations in the DNA!? Now, although they knew this contradicted the prevailing dogma (SMT), the problem was they did not have an understanding of the metabolic theory of cancer at the time so they were unable to explain their findings sensibly.
Next, the Texas group confirmed the Vermont groups’ results by also performing the same experiment in ten mice. None of the mice developed cancer. But they went further by investigating whether the transfer process itself could be the explanation for why the new cells did not behave cancerously. Here, they transplanted nuclei from a cancer cell.. to another cancer cell and then put that into mice. Seven out of the eight mice developed cancer! So it wasn’t the transfer itself which led to the Vermont groups result.
They then did another experiment which blew the whole case wide open. They reversed the Vermont experiment and took mitochondria from a cancer cell and transplanted it to a normal cell. 97% of the mice developed cancer. They had effectively proven the cause of cancer – damaged mitochondria, not damaged nuclei.
Although the above was the conclusion in their paper, the problem was.. their claim was ignored. The NCI made a decision that their experiments merited no further exploration (as per TOTT). The NIH study committees they approached “would not entertain such an idea at the time” as they were focused on genetics and were not about to reverse course completely. Welcome to “Science” folks. Warren Schaeffer of the Vermont team later lamented that he too “was stuck on the genetic origin theory” which confounded him at the time. Later, when he learned about the MTOC, he reflected nostalgically (from TOTT):
“Also at the time, I was not aware of the metabolic research even though I was familiar with Warburg (I spent the greater part of my PhD research work using the Warburg apparatus). However, putting that together with our work should have caused us, in RETROSPECT, to delve further into the earliest research involving mitochondria. Where was Seyfried when we could have used him?
So, if Seyfried had not dug these studies up, they would have been forgotten. Seyfried instead rightly recognized that “the origin of carcinogenesis resides with the mitochondria in the cytoplasm and not with the genome in the nucleus.”
Although Seyfried discovered the above missing pieces to the puzzle simply through a medical literature search, he also did research which contrasted the MTOC with the SMT when he studied the one drug which supposedly validated the SMT and that drug was the famous Gleevec which treats a specific from of chronic myelogenous leukemia (CML).
Gleevec has been held up as the crown jewel product developed through applying the SMT to research, a drug which comes from a class of cancer drugs called “targeted therapies,” i.e. these are drugs which are designed to target a specific genetic mutation. Targeted therapies have long been heralded as a “paradigm shift in cancer drug development” and as “proof of principle” that the SMT of cancer was the right starting point when designing any cancer therapy. Know that CML is a cancer thought to be caused by a defect on a specific chromosome and the defect is present in every CML case.
Briefly, the chromosomal defects in CML form a new “hybrid” gene called ABR-BCL which is stuck in an “on” position such that it produces a large amount of a specific enzyme called a tyrosine kinase. Over many years and across several labs, researchers worked to find a “kinase inhibitor” which would counteract the effect of this overactive gene. The drug they found, called imatinib (Gleevec), led to a complete remission in 53 of the first 54 patients it was tested on!
Per TOTT, no other cancer therapy would have such a profound impact on the field (and the supposed validity of the SMT) and oncologists even refer to pre-Gleevec and post-Gleevec eras. They had literally discovered a non-toxic cure for a cancer by targeting the product of a mutation! The main caveat is that CML is unique amongst cancers in that it is homogenous in terms of the mutation that drives it whereas most other cancers “display a hurricane of genetic chaos.” Thus it vastly oversimplifies cancer given that the vast majority of cancers are too complex to apply a Gleevec model to them. Christofferson argues that its success directed researchers “down a perilous path.”
Here is the amazing thing though. Although Gleevec seemed to validate the SMT, many overlooked the fact that the chromosomal defect causing CML could also be found in a lot of people without the disease! So, something else was needed to cause the cancer! Further, 20% of advanced cases died even with Gleevec treatment.
Here is where Pedersen and Seyfried noticed that Gleevec had a mechanism of action which actually converged with the MTOC. Simply, the BCR-ABL gene also activated a signaling pathway (PI3K/AKT) which also gets activated by damaged mitochondria! This pathway is what causes the cell to dramatically increase glucose uptake and use. When you block ABR-BCL, you are also blocking the glucose uptake pathway signal, thus restoring oxidative metabolism, i.e reversing the Warburg effect! The one targeted drug out of the seven hundred they tested in CML was later found to exert its effect via a metabolic pathway? Coincidence? I think not.
Now convinced of the validity of the MTOC, Seyfried then focused his research first on caloric restriction and then on restricting carbohydrates (i.e. glucose). When carbs are sufficiently restricted (ketogenic diet), the body no longer makes glucose and instead makes an alternative fuel from fat called ketone bodies. Ketone bodies can only be metabolized using oxygen and require healthy mitochondria to do so. Cancer cells do not have this option, so he reasoned that a ketogenic diet would selectively “kill” cancer cells and not normal cells! “Starve” the cancer?
What is now known about ketogenic diets is that they have been shown to positively impact a range of neurological diseases including epilepsy, Parkinsons, Alzheimers, ALS, and brain trauma. Further, ketone bodies appear to preserve and even restore damaged mitochondria!
Seyfried kept researching caloric restriction and ketogenic diets and found they were;
1) Anti-angiogenic – stopped tumors from producing new blood vessels
2) Pro-apoptotic – facilitated orderly cell death
3) Anti-invasive – less metastases in mouse models
4) Pro-aerobic metabolism- it turns down the P13K/AKT pathway which promotes glucose metabolism
Basically, everywhere he looked the diet “pushed back” on every biochemical process which causes a cell to behave cancerously. He then tried what he called the “R-KD” diet (restricted calorie ketogenic diet) on one woman with glioblastoma after her tumor was resected with surgery. Her next few MRI’s showed no evidence of any tumor but then the patient relaxed the diet and less than three months later, the cancer was back. Numerous studies have since supported the beneficial impacts of a restricted and/or ketogenic diet in cancers of the breast, brain, colon, pancreas, lung, and prostate. Studies also show that the same diet also lessens the side effects of chemotherapy. In addition, other studies have shown the diet also potentiates the effects of chemotherapy. Patients who do R-KD and radiation or chemo do better then either one alone.
Ultimately it is Thomas Seyfried who deserves the credit for compiling all the pieces which make up what he coined “The Metabolic Theory of Cancer.” Know that until Seyfried, nobody had been able to complete the theory that began with Warburg’s first observation of aerobic fermentation and finished with Weinberg’s six (later eight) hallmarks of cancer. Seyfried has stated that the MTOC (summarized in his 2012 book “Cancer As a Metabolic Disease”) consists of:
1) A fusion of Pedersens review
2) The work of Sonnenschein and Soto
3) His own work on the damaged lipids of tumor mitochondria
4) His study on the effects of R-KD diets on tumor growth
5) A massive literature search which uncovered the nuclear transfer experiments
6) His background in genetics which enabled him to evaluate the inconsistent and contradictory data from The Cancer Genome Atlas Project.
You would think that after the publication of his papers and books, the National Cancer Institute as well as leading researchers across the world would have shifted focus no? That unfortunately (and predictably - science is stubborn and resists correction) didn’t happen but laypeople noticed. He became a bit of a media star, featured on radio shows and high-profile blogs. He gave lectures at medical conferences where he received standing ovations!
Anecdotal cases of cancer patients employing metabolic therapies began to pop up – some with stunning results. His work and insights were getting out there, but not from the “top down via academia but from the bottom up” through patients, physicians, and the handful of academics who noticed.
As Seyfried wrote in the forward to Christofferson’s book:
“Metabolic therapies will be more effective and less toxic than the current gene-or-immune based therapies, and have the potential to significantly improve quality of life and long-term survival for millions of cancer patients worldwide.”
Travis Christofferson wrote the following in his final Chapter, Where Do We Go From Here:
We have not been at this very long at all. The first chemotherapy was developed in the middle of World War II. By letting highly toxic substances flow through the veins of patients, cancer cells are preferentially (to a small degree) killed off, highlighting that they are more vulnerable than healthy cells. If scientists have mischaracterized the origin of cancer, then we have lost three decades trying to target mutations that are in fact only a side effect rather than the motor driving the disease. If cancer is metabolic, we are just getting started, and real progress should be quick to follow. We will find more ways to push the sick cells over the edge.
As Per OTT, a cosmologist named Paul Davies was hired by the NCI to help break the stalemate in our understanding and treatment of cancer. In 2015, he wrote:
“A major impediment to progress is the deep entrenchment of a 50 year-old paradigm, the so-called somatic mutation theory. . . . If cancer is caused by mutations, so the reasoning goes, then maybe subtle patterns can be teased out of petabytes of bewildering cancer sequencing data. . . . Never has science offered a clearer example of a preoccupation with trees at the expense of the forest.”
CONCLUSION
As alluded to by Christofferson, the sad reality of this entire topic is that cancer research and drug development have been almost exclusively driven by the SMT and that is likely why, despite Nixon’s War on Cancer which began in 1971, currently:
deaths from cancer have increased 9 percent since 1950
From Paul Marik’s Cancer Care book:
As of 1997, the overall contribution of curative and adjuvant cytotoxic chemotherapy to 5-year survival in adults was estimated to be 2.3% in Australia and 2.1 % in the U.S.
5-year cancer survival rate has only increased from 63% to 68% over the last 25 years (1995 to 2018).
Over the past 15 years, the improvement in overall survival by new cancer therapies is a meager 2.4 months.
Advances in all experimental treatment approaches has led to an improvement in overall survival of 3.4 months over the last 30 years.
Further, in the past few decades researchers and funders have been obsessively focused on “targeted therapies” which try to focus on correcting or inhibiting the products of specific mutations. How are targeted therapies doing?
Dr Fojo, head of the Experimental Therapeutics Section at the NCI’s Center for Cancer Research said in 2013:
“A conservative estimate of the number of targeted therapies tested in patients with cancer in the past decade was seven hundred, yet no patients with solid tumors have been cured by targeted therapies over that time period. Zero is the number of targeted therapies that have prolonged survival by one year, when compared to conventional treatment.”
Christofferson’s book reviewed the history of two famous targeted therapies:
Avastin for metastatic colon cancer (later breast cancer as well). It was approved based on its ability to shrink tumors yet it had no impact on extending overall survival. One year of therapy = $90,816. When added to standard of care (paclitaxel), it more than doubles the chance of significant toxicity.
Herceptin for HER-2 positive breast cancer also was approved for shrinking tumors however this did end up having an impact on survival, but quite modest (2.9% improvement in overall survival at 4 years, median survival of 4.8 months longer). Costs $70,00 a year.
From Paul’s Cancer Care Book:
“This data suggests that despite the billions of dollars spent on cancer therapy, the “traditional” approach has largely failed; alternative, less expensive, less toxic, and more effective therapies are urgently required.”
This is where the more recent work of Dr. Paul Marik comes in. “Tripping Over The Truth” inspired Paul to begin working on a project where he reviewed over 2,000 studies on the metabolic mechanisms of hundreds of repurposed medicines and thousands of nutraceuticals as well as other metabolic interventions to treat cancer (i.e. diet). He then created a compendium of repurposed medicines and nutraceuticals that have either been tested in cancer trials or have been used in treatment by practitioners (mostly in other countries where cancer is treated using more diverse tools and approaches than in the U.S. ) Then, based on the depth and breadth of their respective in-vivo, in-vitro, and clinical evidence bases, he assigned graded recommendations for their use in cancer (i.e. strong, weak, and insufficient evidence).
His work is what not only inspired my interest in cancer, but also led to our designing of a prospective observational trial to study the impact of adding combinations of metabolic therapies to current standard of care approaches. With my partner Scott Marsland, we quickly built a complementary cancer care practice and have become a study site where we see patients in all 50 states (and even in other countries).
Just as our clinic responded to what I believe is the greatest unmet medical need in the world, that of treatment for mRNA vaccine injury syndrome and/or Long Covid, we are also now responding to the horrific explosion in cancer timed with and in the wake of the mRNA campaign, most expertly and recently detailed by The Ethical Skeptic here. A couple of recent graphs from that post:

Ultimately, the MTOC and SMT lead to very different therapeutic approaches. Personally, I believe they should both be employed in a “complementary” fashion as we do at our Leading Edge Clinic and in our multi-center study – we do not advise patients to forego standard of care approaches but instead add metabolic therapies in synergy, complementary to the care they already receive.
However, we have also treated some patients who have “exhausted” conventional standard therapies, e.g. some patients come to us because their treatment was stopped either for ineffectiveness or toxicity and they are then only offered comfort care. To date, the results have been mixed in those patients, but we have seen some responses that have been quite dramatic. Here are two PET scans of a recent patient of mine with metastatic lung cancer, the left was taken in June after diagnosis, the right was a follow-up in September (look only at the lung fields, the remaining “spots” in the abdomen represent physiologic uptake):
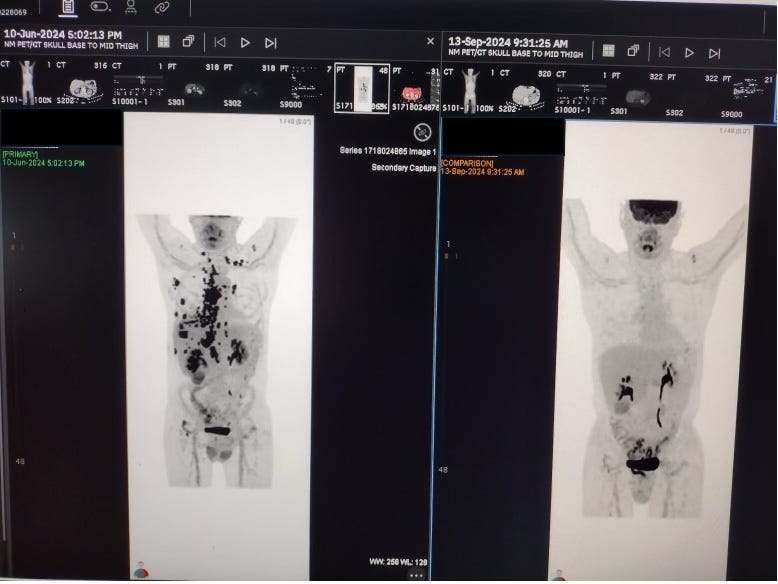
Official Report:”near complete resolution of prior metastatic and pleural disease.”
Although dramatic, I have to say that a number of similar late-stage patients have failed to respond. We desperately need to lean more about why some respond and others don’t. It is my hope that our cancer care study will help start answering that question. Either way, I believe it is time for the NCI and NIH to focus much more on the MTOC in its research funding. If Bobby gets in to HHS, it will be something I hope that I and others can try to influence.
I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amount of time I spend researching and writing my posts, so again, thanks. - Pierre
Fascinating article.
My first career was in radiation therapy. Looking back I see how I was a product of the system. Regurgitating to patients what I had learned in class. I think now that all students of the medical industry are this way. Especially doctors. So overloaded with information to memorize that it does not allow time to ‘think’. Thank you Pierre for taking time to think. About everything we have been told. My whole view has changed regarding treatments for neurological disease such as Alzheimer’s, seizures etc and also for cancer.
Thank you for this excellent article and the dedication to finding truth.
Amazing!! I read Turtles all the Way Down and TOTT on your recommendation. I have worked in an ICU for 30 years but my real education started 4 years ago and you and FLCCC were key to my knowledge. I feel like I am drinking from a fire hose now. THANK YOU!