

The Debate of Covid Science Part 2: A Team of Covid Experts Debate The Opinions Of BC's College Of Physicians And Surgeons
The College's expert claimed that Dr. Hoffe's statement that "ivermectin was effective in the treatment of Covid" violated ethical standards. Here is my written expert defense testimony.

For those of you who have read Part 1 of my expert defense testimony of Dr. Hoffe, I suggest scrolling down to the first “subscribe” button below (hint, hint), given the introduction to this post is identical. (I did this so each post can stand on its own).

Canadian community doctor Dr. Charles Hoffe was one of the first doctors to notice something was “wrong” with the vaccines in April 2021 after he witnessed terrible injuries (strokes, etc.) and a death in the patients he was vaccinating. He then wrote an open letter to the College of Physicians and Surgeons of British Columbia with his observations and concerns, suggesting that perhaps the jabs should be put on pause until their safety could be more assured. One paragraph from his letter said:
“In our small community of Lytton, BC, we have one person dead, and three people who look as though they will be permanently disabled, following their first dose of the Moderna vaccine. The age of those affected ranges from 38 to 82 years of age.”
*For more background, click the tweet below by Dr. Mark Trozzi, another persecuted Canadian doctor for a summary of what is happening to Hoffe and a powerful speech by Dr. Hoffe.

Through FOIA obtained emails, Hoffe and his lawyer discovered that the College’s first and only internal response was to find someone to report Dr. Hoffe for writing the letter. There is no evidence of any concern for the patients nor a request or investigation into Hoffe’s patient records. They instead simply told him each report was a “coincidence” and that it was best if he stops talking about this issue in the hospital. Both shocking and unsurprising, I know.
Hoffe was then banned from working in the local emergency ward and other provincial hospitals. He later submitted more than a dozen claims of vaccine injuries on behalf of his patients, but all were denied validity.
He then rightly continued to speak out publicly, and the three mainstream media outlets in Canada (there are only 3) have, in turn, viciously and repeatedly done hit jobs on him, making him appear as the least credible doctor in the country (which my readers know well is a censoring tactic, i.e., making truth-tellers appear as un-credible as possible so no one will listen to or believe them.)
More recently, the College began an investigation into Dr. Hoffe for numerous public comments he has made since his letter. This is a summary of the supposedly inaccurate statements made by Dr. Hoffe:
6.1. Patient Safety and Experimental Nature ........................................................................... 23
6.2. Potential Harms to Fertility in Women .............................................................................. 27
6.3. Myocarditis in Children .................................................................................................... 30
6.4. Ivermectin for Treatment and Prophylaxis ........................................................................ 33
6.5. Ivermectin Access ............................................................................................................ 36
6.6. Harms to Pregnant Women .............................................................................................. 39
6.7. Microscopic Clotting ........................................................................................................ 42
6.8. Adverse Events Following Immunization ........................................................................... 46
6.9. Harms to Children ............................................................................................................ 50
6.10. Vaccine Shedding ............................................................................................................. 53
6.11. Statement (1). April 4, 2021, email to Dr. Carol Fenton from Dr. Charles Hoffe................... 56
6.12. Statement (2). April 5, 2021, open letter to Dr. Bonnie Henry from Dr. Charles Hoffe ......... 60
6.13. Statement (3). April 21, 2021, email to Dr. Carol Fenton from Dr. Charles Hoffe ................. 64
The College then hired an “expert” named Dr. Trevor Corniel, who submitted a 151-page report with a whopping 191 references. In that report he argues that each and every public statement made by Dr. Hoffe on the above topics was “incorrect,” “misleading,” and “inflammatory” and violated both the College’s “Prudence Standard” and “Harm Reduction Standard.” Know that these “standards” are ethical codes of conduct that members of the College must abide by (remember ethics?). In my expert opinion, I argue that Corneil (knowingly or unknowingly) amassed data from fraudulent peer-reviewed literature and captured public health agency recommendations to support his conclusions that Hoffe is in violation of practice standards.
If Dr. Hoffe were to be found guilty as argued by Dr. Corniel, he is at risk of losing his livelihood (license) and could be fined up to $100,000. So, they want to end his career and then take his money? I wonder how many future doctors will speak up against the next Big Pharma-Government fraud in Canada once Hoffe’s fate becomes well-publicized? As far as I can tell, Canada only had less than a handful of publicly outspoken doctors and scientists in Canada during COVID (Charles Hoffe, Byram Bridle, Mark Trozzi, Paul Alexander, and William Makis - if I am leaving anyone out, I apologize). However, good luck hearing advice from un-conflicted doctors in the next pandemic.
**Since first posting this, subscribers have sent me other names of outspoken and/or persecuted Canadian docs and scientists so the list is larger than I thought: Rochagne Killian, Patrick Phillips, Chris Shoemaker, Daniel Nagase, Rodger Hodkinson, Patrick Phillips, Chris Milburn, Laura Braden, Michael Palmer, Crystal Luchkiw, Francis Christian, Dr. Steven Pelech, Dr. Chris Shaw, Dr. Howard Tenenbaum, Dr. Ira Bernstein (how could I forget Ira!?), Dr. Bonnie Mallard, and Dr. Linda Rapson.
Anyway, Hoffe’s lawyer, Lee Turner of Doak Shirreff Lawyers LLP in Kelowna, B.C., engaged me to defend a number of Hoffe’s statements regarding ivermectin and shedding. I was proud to learn I was joining an All-Star team of medical dissident experts defending him, such as Jessica Rose, Peter McCullough, Kevin McKernan, etc. I plan to ask them to also post their expert reports on Substack, and I will create a central post linked to all for those interested.
Of note, Lee has been practicing trial law in British Columbia for 30 years and is experienced in administrative, public health, and personal injury law. He has been very busy in Covid as he has represented numerous nurses, physicians and other health care providers and individuals who were negatively impacted by Canadian Covid-19 public health measures and mandates (which as you know were far more draconian than here in the U.S.)
I elected to do the case pro-bono and began by reading Corneil’s “expert” report, which viciously and repeatedly attacked Hoffe for his many accurate statements. I was so infuriated after reading it, I said to myself, “Game on (expletive)” and immediately launched into a writing and researching frenzy over the last five days, and I would say I put over 20 hours of work into my report. It is 47 single-spaced pages with who knows how many hyperlinked references.
I hope I am not being too full of myself, but I want to share what Lee Turner wrote to me after he read it:
“Pierre, I don't even know how to express how incredible the information in your report is. It is one of the most thorough and well-written expert reports I have read in my 30 year career. And I have read a lot of expert reports. I made a few minor corrections to spelling, and adding in punctuation (periods, commas or colons) and that was it. I think it is very well written and contains powerful evidence.“
Let’s go through Count #2 against Dr. Hoffe shall we? (Defense of Count #1 is here)
EXPERT REPORT - Dr. Pierre Kory, MD, MPA
Dear Mr. Turner,
I acknowledge correspondence from you dated November 3, 2023, asking me to formulate an independent professional opinion concerning the safety and effectiveness of ivermectin as a treatment and prophylaxis for SARS-CoV-2 (Covid-19), as well as the science regarding Covid-19 vaccine “shedding.”
You have asked me to comment on the opinion expressed by the “expert”, Dr. Trevor Corneil, relied upon by the College concerning these issues in his report dated September 26, 2022, specifically in sections 6.4, 6.5 and 6.10 of his report.
I am aware of my duty to assist the panel, and I am not an advocate for any party. I have prepared this report with this in mind and am happy to testify in any setting to address questions regarding the matter.
I attach as Appendix B, a copy of your letter of instruction, including the list of documents which I have reviewed in forming my opinion.
Response To Section 6.4 of Dr. Trevor Corneil’s Expert Opinion
My first comment on Dr. Corneil’s report is that he carefully defines the following terms: “misleading”, “incorrect”, and “inflammatory” and then judges Dr. Hoffe’s statement in relation to meeting the definitions of each term above. He then follows each statement’s characterization according to these terms with his opinion as to whether Dr. Hoffe’s statements meet the College’s “Prudence and Harm Prevention” standards.
Similarly, for the below expert report, understanding the arguments I put forth requires knowledge of the word “disinformation.” The Oxford English dictionary definition is “a form of propaganda involving the dissemination of false information with the deliberate intent to deceive or mislead.”
Understanding my below expert opinion and how I arrived at it also requires the knowledge that disinformation has been long deployed by select corporations across a range of industries. In the article called “The Disinformation Playbook”, written by the Union of Concerned Scientists, they write, “Corporations manipulate science and scientists to distort the truth about their products, using a set of tactics made famous decades ago by the tobacco industry. We call these tactics the Disinformation Playbook.” As you read through all the disinformation campaigns they cite in the article, you realize that the pharmaceutical industry is over-represented in that list.
An important point to understand about disinformation tactics is that corporations deploy them when “science emerges that is inconvenient to their interests.” The Disinformation Playbook was first developed in the 1950’s by the tobacco industry to scientifically counter the emerging reports of greatly increased incidences of cancers in smokers. They successfully used disinformation for 50 years until the Master Settlement in 1995 with the US Attorney Generals of 50 states.
As one of the world experts in the use of ivermectin in the prevention and treatment of Covid-19, my first review paper called “Review of the Emerging Evidence Demonstrating Efficacy of Ivermectin in the Prevention and Treatment of Covid-19” is one of the most popular published scientific papers of the last 15 years with an altmetric score ranking it the 10th most popular paper out of the last 25 million papers published.
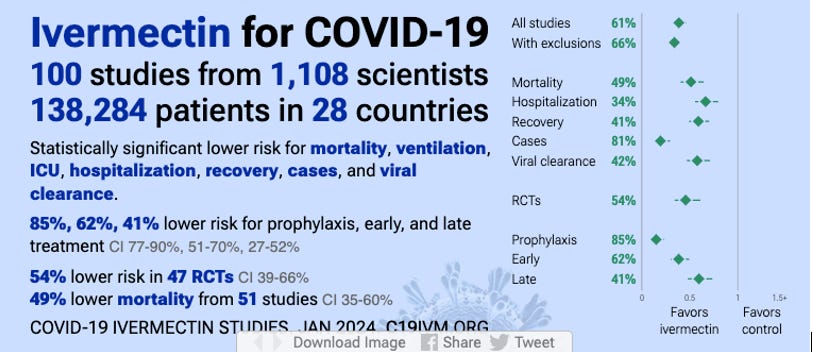
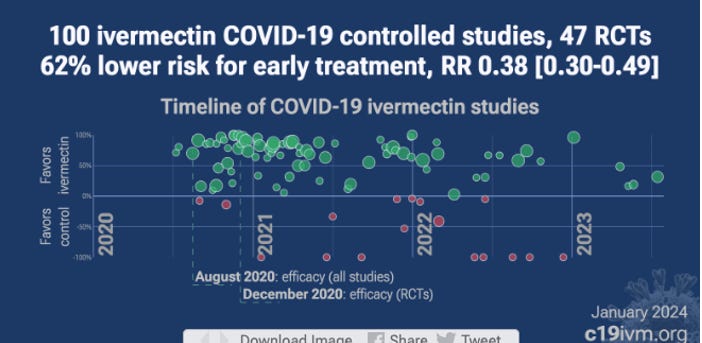
Based on my intensive study of the ivermectin evidence base, including in-vitro, in-vivo, clinical and epidemiological studies, the evidence for efficacy is overwhelming, with, as of today, January 10, 2023, results available from 100 controlled clinical trials, 47 of them randomized, with meta-analysis data finding statistically significant, large magnitude reductions in mortality, hospitalization, time to clinical recovery, and time to viral clearance.
However, Dr. Corneil, along with numerous public health agencies and professional societies across the world’s advanced health economies, consistently ignore or systematically dismiss and distort the evidence of efficacy based on the widespread “opinion” that the evidence base represents “low-quality” evidence that should not be relied on. This is a well-known Disinformation tactic called “the Diversion” where the pharmaceutical industry co-opts third-party agencies and organizations to “manufacture uncertainty where little or none exists.”
The reasons for the Disinformation campaign against ivermectin are multiple. First is that knowledge of ivermectin’s efficacy in both prevention and treatment would have led to the revocation of the EUA supporting the massive Covid vaccine market in the United States and across the world. Second, it would also increase what public health authorities perceived as the #1 enemy in the pandemic, that of “vaccine hesitancy.” A third reason is that knowledge of ivermectin’s efficacy would greatly decrease profits from the competing, patented, highly-profitable Covid medicines such as remdesivir, paxlovid and molnupiravir.
The article “The Disinformation Playbook” names and defines the main Disinformation tactics. The most prominent disinformation tactics deployed against ivermectin have been extensively documented in my book called “The War on Ivermectin.” The tactics described from their 2017 article are as follows:
1) The Fake:
a. using fraudulent studies designed to achieve predetermined results [against ivermectin]
b. censoring the publication of positive studies [of ivermectin in prominent medical journals]
c. selectively publishing only negative studies [of ivermectin in prominent medical journals]
2) The Blitz:
Harassing scientists who speak out with positive results [for ivermectin]
3) The Diversion:
Using front groups and third-party organizations to “manufacture uncertainty where little or none exists” [about the efficacy and safety of ivermectin]
4) The Screen:
Buying credibility through alliances with academia or professional societies [recommending against ivermectin].
5) The Fix:
Manipulating government officials or processes to inappropriately influence policy [against ivermectin].
For the purposes of this report, I will focus mostly on the first tactic above called “The Fake,” which largely focuses on the behavior of high-impact medical journals in their “selective” publication of brazenly manipulated trials intended to reach a “predetermined result.”
Another aspect of “The Fake” disinformation tactic is “censoring reports of positive studies.” Evidence of dozens of rejection letters to investigators of positive studies of ivermectin can be found in Chapter 28 of my book, “The War on Ivermectin” (Exhibit B). In Chapter 27 (Exhibit C), I detail unprecedented examples of positive peer-reviewed papers on ivermectin being retracted without accusations of fraud or plagiarism. My paper was one of them, and this action was unprecedented in the cumulative 120 years of my co-author’s and my careers.
The behavior of the medical journals in regard to ivermectin was, in my opinion, the foundation of the entire global disinformation campaign and has most contributed to the widespread, false beliefs regarding ivermectin that are held by the global medical community.
So, to understand the context of the numerous brazen and fraudulent manipulations of the published data on ivermectin that I will describe in my report, I think it is important that the College understand that the high-impact journals are nearly completely under the control of the pharmaceutical industry.
For support of my statement above that “Big Pharma” exerts immense influence of our most respected medical journals, I will reference the book written in 2001 by the former 20-year Editor-in-Chief of the New England Journal of Medicine (NEJM), Dr. Marcia Angell (she was also the first woman to serve in this role.) The book is called “Drug Companies & Doctors: A Story of Corruption.”
A well-cited statement of Dr. Angell is:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor.”
Dr. Relman, another former editor-in-chief of the NEJM, said this in 2002:
“The medical profession is being bought by the pharmaceutical industry, not only in terms of the practice of medicine, but also in terms of teaching and research. The academic institutions of this country are allowing themselves to be the paid agents of the pharmaceutical industry. I think it’s disgraceful.”
Richard Horton, editor in chief of the Lancet, said:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue. Afflicted by studies with small sample sizes, tiny effects, invalid exploratory analyses, and flagrant conflicts of interest, together with an obsession for pursuing fashionable trends of dubious importance, science has taken a turn towards darkness”
THE EVIDENCE CITED BY DR. CORNIEL
Let’s begin to examine the evidence cited by Dr. Corniel in his contrary opinion to Dr. Hoffe’s statement that ivermectin is effective in Covid-19.
Statement by Dr. Charles Hoffe (d). Dr. Hoffe stated in an interview with Laura-Lynn Tyler Thompson, video of which was posted online on or around July 6, 2021, at 20:45 – 21:23:
“…There are brilliant, very, very safe, very effective treatments for Covid, and for the medical authorities to tell them that they have to go home and do nothing is is utter negligence. … And for people to say that it is it is safer to do nothing than to take something like ivermectin, which is unbelievably safe – I mean, in many countries, it’s available without prescription, I mean it’s safer than aspirin, it really is safer than aspirin, um, so it is absolutely absurd [inaudible] that this is being denied from people”.
In Dr. Corneil’s assessment of the accuracy of Dr. Hoffe’s statement, he concludes the following in regard to the use of ivermectin to prevent or treat Covid-19:
Prior and current evidence strongly suggest that Ivermectin is neither a safe nor effective treatment or prophylaxis for Covid-19 illness. A meta-analysis published in April 2021 urged caution as available trials investigating the use of ivermectin for prophylaxis against Covid-19 exhibited a serious risk of bias and imprecision.141 A Cochrane systematic review conducted in July 2021 noted that the reliable evidence available did not support the use of ivermectin for treatment or prevention of Covid-19.142 Recently, a double blind randomized clinical trial of over 1400 patients observed that administering ivermectin did not prevent the occurrence of serious outcomes, hospitalizations or death from Covid-19.143 The World Health Organization issued a recommendation on March 31, 2021 against the use of ivermectin for patients with Covid-19, regardless of disease severity, except in the context of a clinical trial.144 On Oct. 19, 2021, Health Canada issued a public advisory not to use ivermectin to prevent or treat Covid-19.145
From the above, it is clear that Dr. Corneil cited only two studies to support his assertion that “Prior and current evidence strongly suggest that Ivermectin is neither a safe nor effective treatment or prophylaxis for Covid-19 illness.”
I think it is important that we carefully review the innumerable deficiencies, anomalies, and limitations of the two papers he cited to support the above statement.
In terms of meta-analyses, Dr. Corneil chose to cite only the Cochrane Review of ivermectin by Popp et al. I am concerned that he selectively relied on a single “supposedly negative” meta-analysis and ignored multiple supportive meta-analyses such as Hariyonto et al., Babalola et al., Bryant et al., and Kory et al. I must ask the question as to why an “expert” would ignore such a large, positive evidence base in drawing his conclusions?
Let us begin by analyzing the Cochrane review. First off, Popp et al. excluded dozens of observational controlled trials (“OCT’s”) from their meta-analysis.
The College must be aware that there is no evidence to support the growing practice of systematically excluding OCT’s from systematic reviews and meta-analyses. In fact, it is in violation of evidence based medicine (“EBM”), given that it willfully ignores decades of research which have found, on average, that OCT’s and RCT’s reach the same conclusions.
From the definitive Cochrane review on this topic, the authors conclude that “factors other than study design per se need to be considered when exploring reasons for a lack of agreement between results of RCTs and observational studies.” Further, prominent professional societies have issued policy statements to reverse this practice by concluding, from their analyses of controlled trial designs, that “observational studies should be considered in developing clinical practice guidelines and in making clinical decisions.” Lastly, until Covid, the WHO routinely relied on more diverse sources of data and trial designs to inform their treatment recommendations.
Finally, know that none of the positive meta-analyses arbitrarily excluded such a large portion of the evidence base. One expert systematic review group’s critique of Popp et al.’s review, aptly titled their paper “The Uses and Abuses of Systematic Reviews.”
I maintain that excluding OCT’s is a form of disinformation in that OCT’s can be done for little to no funds by independent investigators free of pharmaceutical conflicts of interests. The known and explicit bias of the massive funders of large RCT’s are rarely present in OCT’s. I maintain that is why the pharmaceutical industry and its high-impact medical journals have increasingly avoided publishing OCT’s in the last decade.
Further, another astonishing violation of EBM is the repeated insistence that “low quality” trials be ignored. The reality is that there is no published evidence that I am aware of that finds that “low quality” controlled trials reach different conclusions than “high quality” controlled trials. In fact, there is only one paper I know of that compared the conclusions of what current EBM grading systems determine is low quality and high quality. In that paper, they found that low-quality and high-quality trials also reach the same conclusions on average.
Thus, it is my strongly-held, evidence-based opinion that the systematic ignoring of both OCT’s and “low quality trials” are instead fraudulent efforts to create the myth that only “Big RCT’s” that require massive funding can determine “scientific truth” or “scientific consensus.”
In the below expert opinion, I will provide extensive evidence that the bias of the funders of those “big RCT’s” essentially determine the results of the RCT’s and those results are then used to establish a fraudulent “scientific consensus.” This occurs when the “real science” I described above reaches conclusions that are “inconvenient to the interests of the pharmaceutical industry.” I suspect that many members of the Royal College of Physicians and Surgeons are unaware of how rife disinformation is or of the studies I just presented regarding the soundness of non-RCT derived evidence.
In contrast to Dr. Corneil and the numerous professional society recommendations he cites, many independent experts like me have, in line with this knowledge of the equivalence of OCT findings and RCT findings and high quality and low-quality trials, chosen to rely upon a “totality-of-the-evidence standard” and include data from OCT’s and supposed “lower-quality” trials. This practice is the most adherent to the foundational principles of Evidence Based Medicine (EBM).
Recall that in the 1980’s, responding to the need to overturn entrenched dogmas with scientific evidence, Gordon Guyatt coined the term “evidence-based medicine” (“EBM”). Then in 1996, David L Sackett published a widely-cited article defining exactly what EBM was: the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.
Notice how Sackett does not define current best evidence as “RCT’s only”:
“By best available external clinical evidence we mean (Ed: all?) clinically relevant research, often from the basic sciences of medicine, but especially from patient centered clinical research into the accuracy and precision of diagnostic tests (including the clinical examination), the power of prognostic markers, and the efficacy and safety of therapeutic, rehabilitative, and preventive regimens. External clinical evidence both invalidates previously accepted diagnostic tests and treatments and replaces them with new ones that are more powerful, more accurate, more efficacious, and safer.”
Put differently, Sackett proposed that three different considerations that needed to be weighted equally in evidence-based clinical practice:
•Patient Values
•Clinical Expertise
•Relevant Research
In terms of relevant research, the summary analyses of the RCT’s alone, the OCT’s alone, and their combined evidence base, all find highly statistically significant reductions in mortality, hospitalization, time to viral clearance, and time to clinical recovery. Yet, the agencies and societies across the world all ignored the OCT’s and included only a subset of the RCT’s.
It is my professional opinion that these actions were willfully committed as a disinformation tactic to “arrive at a pre-determined result”, which is to find that ivermectin is ineffective in preventing Covid-19 for the reasons I stated above. It should be unsurprising to know that the high-impact journals were under immense pressure from Big Pharma to support the vaccination campaign, and distorting and suppressing the evidence base for ivermectin (and hydroxychloroquine) was critical in that effort. Dr. Hoffe was almost certainly aware of this reality given his statement above is clearly supported by an expert knowledge of the available trials data.
** To readers, know that I devoted an immense amount of effort in compiling this report which took me away from many other responsibilities, not least of which was my family. I plan to do the same pro-bono for any doctor who needs it, even though each case requires an independent report that takes hours. If you appreciate what I am doing for doctors, support in the form of paid subscriptions would be greatly appreciated.
IVERMECTIN IN THE TREATMENT OF Covid-19
The main tactic that agencies and “experts” like Dr. Corneil use to reject extensive evidence in favor of the use of ivermectin in Covid-19 is to isolate a few negative studies and attempt to highlight them without acknowledging the substantial body of trials contributing data for a substantial meta-analysis.
Of the 42 RCTs available to Dr. Corneil at the time of his report, Dr. Corneil simply cited one “negative” RCT (Bramante et al.) and one Cochrane systematic review from July of 2021 (over a year prior to the submission of his report). Why did he not rely on the most up-to-date evidence?
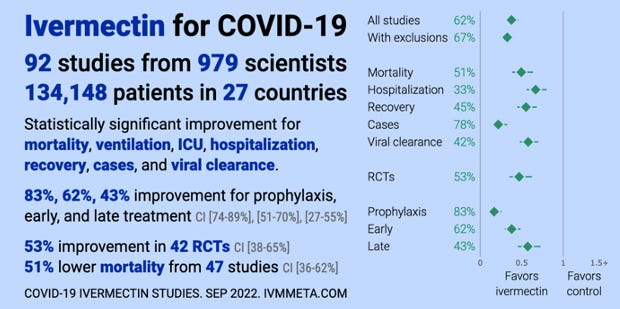
The overall tracking of the studies along with a real-time meta-analysis of not only ivermectin but also dozens of other Covid therapies using the same inclusion and meta-analysis protocol can be found at c19early.com. The results for ivermectin in treatment of Covid as of today, January 10, 2023, are based on 83 controlled trials (17 of the 100 below are in prevention and were reviewed in the previous section.) Note the Forest plots showing the meta-analysis findings to the right in the below figure:
It is widely believed that meta-analyses (summary analysis of all individual trials data) represent stronger evidence than a single study or small collection of studies. I am concerned at the outset that multiple supportive meta-analyses were ignored by Dr. Corneil such as Hariyonto et al., Babalola et al., Bryant et al., and Kory et al.
In addition, the ivermectin meta-analysis performed by the WHO was ignored by Dr. Corneil. Let’s examine that one first.
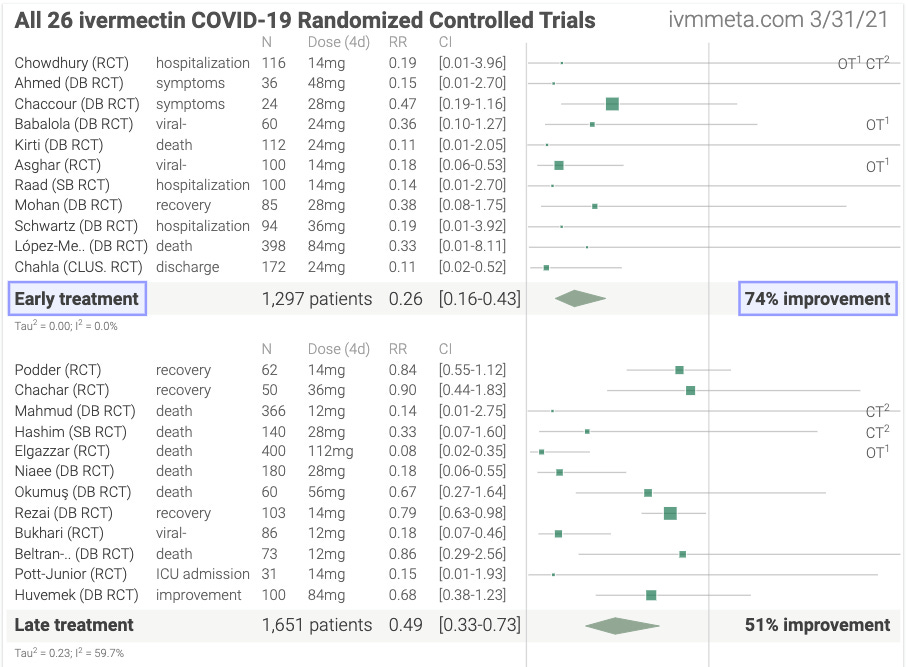
The screenshot below is from the WHO Guideline on Therapeutics and Covid-19 (which has not been updated in over two and a half years despite the evidence base now including 47 RCT’s). As you can see, the WHO only included 6 RCT’s that studied mortality as an endpoint when there were results from 26 RCT’s available at the time (the below screenshot is taken from the Internet archive of ivmmeta.com on March 31, 2021):
Note that from the six studies they included, the WHO found that there were 70 deaths per 1000 in the standard-of-care treated patients versus 14 deaths per 1000 in ivermectin treated patients, leading to a statistically significant 81% reduction in mortality. The chart below is from the WHO guideline document:
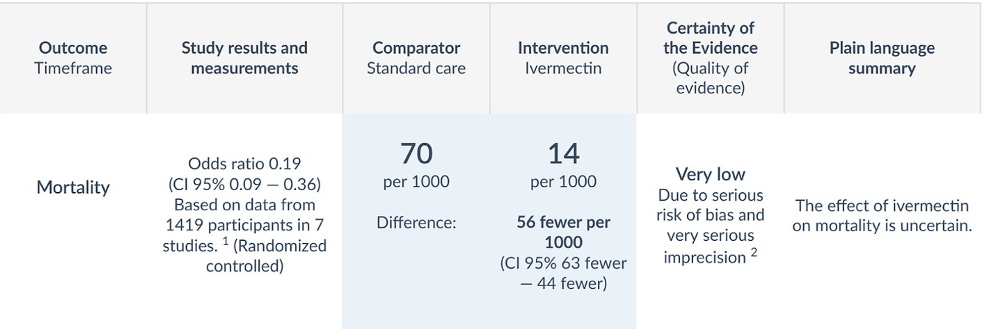
In the “Certainty of the Evidence” column, they graded the evidence as having “very serious imprecision.” Know that the independent expert systematic reviewer team of Lawrie et al. that has long worked for the WHO, graded the quality of evidence higher. More recently, the authors argue that “downgrading the quality of the evidence to this degree based on imprecision is incorrect when the treatment effect is so large, the outcome prevented is death, and the medicine is one of the safest, least expensive, and most widely available in the world.”
Further, I, along with many other ivermectin experts, strongly disagree--and are deeply troubled by--the rationale put forward by the WHO Guideline Development Group for not recommending ivermectin to the world:
“Applying the agreed values and preferences, the GDG [Guideline Development Group] inferred that almost all well-informed patients would want to receive ivermectin only in the context of a randomized clinical trial [emphasis mine], given that the evidence left a very high degree of uncertainty in effect on mortality, need for mechanical ventilation, need for hospitalization and other critical outcomes of interest and there was a possibility of harms, such as treatment-associated SAEs [serious adverse events].”
The College must understand that the WHO based their entire recommendation against ivermectin by arguing that acutely ill patients would rather participate in a placebo-controlled trial instead of immediately being treated with one of the safest medicines in history at a time that the WHO’s best available evidence found an 81% chance of reducing their chances of dying.
This is beyond absurd as most people on the planet would not have access to an RCT nor would most acutely ill patients refuse a potential life-saving therapy in favor of a placebo while in the face of a life-threatening illness. A much more appropriate and humane action would have been to issue a “weak” or “conditional” recommendation, which the ivermectin evidence clearly met WHO’s criteria for.
Either way, Dr. Corniel ignored the WHO review and chose to cite only the Cochrane Review of ivermectin by Popp et al. and not the positive meta-analyses by Hariyonto et al., Babalola et al., Bryant et al., and Kory et al. I must ask the question as to why an “expert” would ignore and/or “cherry pick” from such a huge supportive evidence base in drawing his conclusions?
Most troubling about the only review Dr. Corneil chose is that Popp et al. only selected 14 of the 31 published studies available at the time, rejecting large studies with positive effects on questionable grounds, such as:
· A demand that only studies with PCR testing be included even though availability and accuracy varied considerably, especially at the time;
· Inconsistent rejection of comparators, such as disallowing trials against hydroxychloroquine even though it has been determined by these same reviewers to be [?] without clinical effect and thus could properly serve as a control/comparator group;
· Exclusion of combination therapies even though that is how it is actually used in practice. A principal criticism the Popp authors had of favorable studies was inclusion of those that used doxycycline in the intervention arm, complaining that the impacts of doxycycline could not be separately determined. Popp, ibid. at 32-33. While there may be some sense to this, given complications such as pneumonia, if doxycycline had a significant therapeutic impact on Covid-19, we would be living in a better world;
· In five of the included studies in the unfavorable Popp review, subjects only received a single dose, which could not have possibly reached therapeutic levels and are not valid studies. Subjects only received the FLCCC-recommended dosing in five of the 14 studies. Ibid. The study authors expressly state that they were aware of the dosing issue but did not have sufficient information to look at dose-response curves, yet included low-dose studies in the analysis in any event;
· Pre-defined (and essentially arbitrary) time points for outcome measures (28-day mortality, infection within 14 days) resulted in further exclusions; and
· High risk of bias studies were rejected for “primary” analyses.
The inclusion policies thus excluded much of the available trials yet Popp et al. still were not done whittling down the evidence base. They then further fragmented the data by analyzing inpatient and outpatient data as separate comparisons, though the patients had the same disease and hospitalization criteria varied considerably according to local resource constraints.
More anomalous actions occurred when more than a year later, Popp et al. released an updated version. They somehow managed to add new criteria so that seven of the 14 studies they had included the previous year were no longer eligible. Even though new trials were added, they ended up with fewer studies in 2022 than in 2021.
It is generally not good practice for a systematic review to modify its protocol between revisions—since it gives the impression of p-hacking taking place.
This protocol modification led to even more problems. The new criterion—that did much of the heavy lifting in terms of exclusions—was the “trial registration” criterion, specifically the requirement that a trial be prospectively registered:
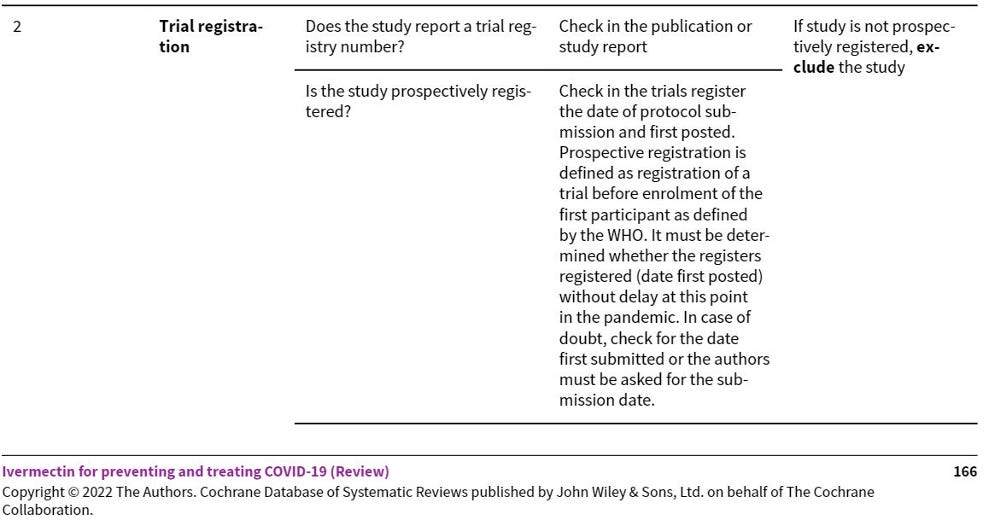
They were quite clear that if the date of registration is not before the date of the enrollment of the first participant, the study should be excluded. In fact, on the basis of this criterion, they excluded several studies they had included in their 2021 edition of their systematic review. The excluded trials were: Abd-Elsalam, Biber, Chachar, Okumuş, and Shah Bukhari.
The problem is that, despite this clearly-stated new exclusion criteria, they selectively ignored it by including the five largest studies, all of which did not prospectively register their trial prior to enrolling the first patients. The trials are TOGETHER, Vallejos, I-TECH, Kirti, and Gonzalez. By violating their own trial protocol, they invalidated the systematic review, since 2,582 of the 3,409 patients included did not qualify for inclusion.
Another disturbing anomaly within the Popp et al. review is that the authors stated “serious adverse events (SAE) including vision problems, neurotoxicity and liver damage can occur” though the cited source contains no such reports. Moreover, the considerable literature on safety is ignored (see next post).
Finally, know that none of the positive meta-analyses arbitrarily excluded such a large portion of the evidence base. One expert systematic review group’s critique of Popp et al.’s aptly titled their paper “The uses and abuses of systematic reviews.”
The only other study that Dr. Corneil cited was an RCT by Bramante et al., which was a “remote” phase 3, double-blind, randomized, placebo-controlled trial which included 1,431 patients.
There is an almost innumerable amount of critical, severe, and major issues with this trial, as delineated in the analyses contained in the links below (click on these links to see the c19rearly.com group’s evidence of these issues):
CRITICAL: Ivermectin vs. placebo analysis - 61% lower hospitalization.
CRITICAL: Severity mismatch for ivermectin treatment but not for any other medication or control
CRITICAL: Ivermectin vs. placebo symptoms consistent with efficacy
CRITICAL: Multiple outcomes missing, including time to recovery
CRITICAL: Adverse events suggest authentic ivermectin not taken
CRITICAL: Major event counts differ between paper and registry
CRITICAL Control group includes metformin, adjustment protocol violation
CRITICAL: Primary outcome changes
CRITICAL: All 7 secondary outcomes deleted
CRITICAL: Author claims results from 596 researchers should be censored for false information
CRITICAL Administration on an empty stomach
17 CRITICAL: Results delayed 6 months (including life-saving metformin results)
CRITICAL: Subject to participant fraud
20. SERIOUS: Control arm results very different between treatments
SERIOUS: Authors claim placebo is not better than the treatments
SERIOUS: False conclusion
SERIOUS: Trial outcomes modified
SERIOUS: Very high percentage of missing data
SERIOUS: Treatment 3 days for ivermectin, 14 days for metformin and fluvoxamine
SERIOUS: SAP dated after trial
SERIOUS: Test requirement and delivery prohibits early treatment
SERIOUS: Conclusion modified by journal
SERIOUS: Symptom results contradictory
SERIOUS: Adherence very low
34: SERIOUs: Inconsistent blinding statements
SERIOUS: Author indicates a best guess can be used for onset
MAJOR: Ivermectin from source chosen has shown lower efficacy
39. UNKNOWN: Maximum symptom duration not clear
UNKNOWN: No discontinuation due to hospitalization for ivermectin
COMMENT: Authors indicate up to 5 day delay in real-world usage
I ask the College to recognize that, despite all of these severe, critical, and major issues identified in the c19early.com groups analysis of the study, it sailed to publication in the highest-impact medical journal in the world.
Thus, it is my opinion that the numerous above actions by the investigators essentially prove that this trial was an example of the Disinformation tactic called “The Fix,” whereby investigators conduct a trial with the intent of reaching pre-determined results, i.e., to show that ivermectin does not work.
Further, I find it troubling that Dr. Corneil would rely on only a single RCT out of the 42 available to him at that time of his report as below (note date of this summary chart - September 2022):
I must add here that the Bramante et al. study was not the only “Fix” within the ivermectin evidence base. Studies with similarly identified anomalies in the design and conduct of the trial include TOGETHER, Lopez-Vallejo, and the two ACTIV-6 trials but a discussion of their deficiencies are beyond the scope of this report.
If interested, I refer you to Chapter 25 in my book called “Counterfeit Trials - The Big Six”, which provides significant documentation that the 6 largest studies referenced therein, all published in high-impact medical journals, were brazen examples of studies that were “designed and conducted with pre-determined results.”
Finally, beyond the 83 controlled trials in treatment available (43 of them RCT’s) and the numerous positive meta-analyses, there are also a number of health ministry reports of early treatment programs with ivermectin, all showing large reductions in hospitalization or death. See:
· La Misiones, Argentina – Their Health Ministry analyzed the data from 4,000 ivermectin-treated patients and, compared to the rest of the population over the same time period, found a 75% reduction in need for hospital and an 88% reduction in death.
· Uttar Pradesh, India – The government used a strategy of close surveillance combined with both ivermectin treatment of all positive cases and preventive treatment of all family contacts. On September 10, 2021, only 11 cases with no deaths were recorded in a population of 241 million with 67 of their 75 districts having no active cases at the time.
· The Brazilian city of Itajai – They offered ivermectin as prevention to the entire city’s population with 133,051 (60%) agreeing to take ivermectin every two weeks for 6 months. Compared to the 45,716 city inhabitants that declined to use ivermectin, ivermectin users were 47% less likely to contract illness, had a 70% lower mortality rate, and a 67% lower hospitalization rate. By the end of the 6 month program, the citywide Covid mortality fell from 6.8% to 1.8%.
· La Pampas, Argentina – The Health Ministry compared over 2,000 patients they treated early with ivermectin to over 12,000 without treatment and found that in patients over 40, rates of ICU admission and death both fell by 40%.
· Peru – Their government conducted a nationwide mass-distribution program called “Mega-Operación Tayta” (MOT), initiated at various times across 25 states of Peru in May 2020, led to a 74% drop in regional excess deaths within a month, with each drop beginning 11 days after each MOT region’s varied start times.
· The Health Ministry of Sultan Kudarat, Philippines – They launched an ivermectin drive and found that cases rapidly dropped by 86%. compared to nearby regions.
Finally, 23 countries (39 including NGO’s) have now given either partial or full approval for use of Ivermectin to treat Covid, which encompasses 25% of the world’s population.
Thus, based on the large and consistently positive evidence base from RCT’s, OCT’s, and health ministry reports, I find Dr. Hoffe’s statements on the efficacy of ivermectin to be fully supported by and consistent with the scientific evidence. I, thus, strongly disagree with Dr. Corneil’s conclusion.
P.S. **Know that I devoted an immense amount of effort in compiling this report, which took me away from many other responsibilities, not least of which was my family. I plan to do the same pro-bono for any doctor who needs it, even though each case requires an independent report, which takes hours. If you appreciate what I am doing for doctors, support in the form of paid subscriptions would be greatly appreciated.
Ok, more to come in subsequent posts detailing my expert report defending Dr. Hoffe. Stay tuned.
P.P.S. Our 3rd Annual FLCCC. Medical Conference is coming up! Come on down to Phoenix. I cannot tell you how not only informative but also how spiritually and socially restorative these conferences are, as the community has some of the best people ever in it!

Gather with like-minded people from across the world, learn from leading medical experts and health freedom advocates, meet healthcare professionals, and take charge of your health and well-being!
- I am also proud to report that my book has gained Best Seller status in several countries and is climbing up the U.S. Amazon rankings. If any of you have bought and read the book, please leave a review on Amazon? Thanks! Link:
As a reader of Kory’s writings early in covid, he made a point about the 30,000 foot view of ALL of this ivermectin talk: the directionality tells the story.
When patient responses are thrown up on the board as clouds of dots in sundry trials of varied complexity, rigor, size, etc., ONE thing stood out about ivermectin: it showed DIRECTIONAL improvement. “How much” was a secondary phenomenon.
Think of it this way. CPR probably has a wildly varied outcome depending upon the circumstances of any individual case. Was it performed in a hospital by staff while in surgery, in the field by EMTs, or in the supermarket by some teenaged bystander? Outcomes probably are recorded already by class, and it would stand to reason that the above list declines in positive outcome. However, the mere fact of administration of CPR no doubt is borne out in records that positive outcomes are possible whereas negative outcomes are moot.
In the case of ivermectin, if the needle is consistently moving directionally in the favor of positive outcome, then there is efficacy. Because the safety profile is, uniquely, so benign, ivermectin was blessed with this de-cloaking device that enabled Kory to see and declare this beautiful discovery. By causing no known harm, any needle movement PROVES action, and if action is positive, the treatment has efficacy.
On this basis, standing alone, ivermectin earned its place in the arsenal, and Kory cemented his place in history as a savior of countless lives.
Many thanks to you and Paul. You have saved one life in this family with your protocol, which had to be fought for against 4 critical care physicians. Your details mattered, and they prevailed.
Thank you for doing this work pro bono. For all of us.