

How I Lost Three ICU Jobs During the COVID-19 Pandemic - Job 1
Prior to COVID, I was a nationally known expert in Pulmonary & Critical Care Medicine. Despite the massive need for specialists like me across the US, I had to leave 3 different US medical centers.

What follows is my standard “Super Short Bio” that I send to folks whenever I have to give a lecture so they can introduce me quickly (lecturers in medicine essentially get a summary of their CV read as an introduction before they speak, with some lecturer introductions lasting 15 minutes - I exaggerate only slightly). I actually have several different bios, a “super short one”, a “short one”, and a “long one,” each of which I use for distinct purposes. I have been giving lectures across the country and world to doctors in my specialty for over 15 years, on a variety of topics that I am expert in, chief among which was the use of ultrasonography in the diagnosis of acute respiratory failure & circulatory shock states, the use of therapeutic hypothermia after cardiac arrest, and the use of high dose intravenous Vitamin C in severe sepsis.
PRE-COVID “SUPER SHORT BIO”
Dr. Kory is a Pulmonary and Critical Care Medicine specialist, and is a former Associate Professor and Chief of the Critical Care Service at the University of Wisconsin. He is an internationally renowned pioneer in the field of critical care ultrasonography, having served as senior editor of an award-winning textbook in its 2nd edition, now translated into 7 languages. Dr. Kory is also considered a master educator and has won major Departmental Teaching Awards at multiple institutions during his career.
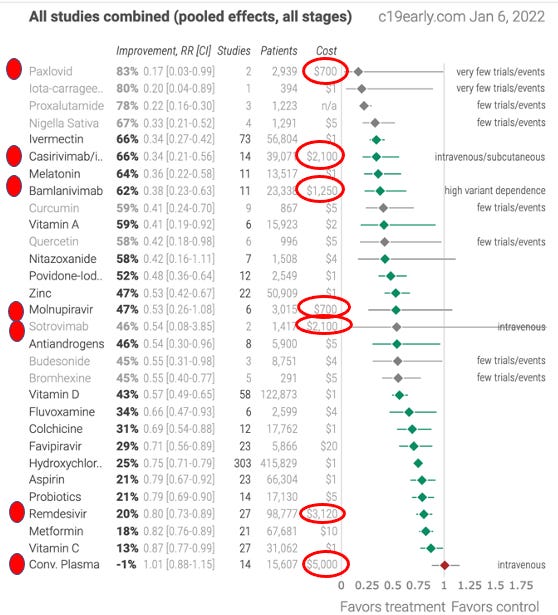
I do not include the above as some sort of ego exercise but rather to introduce the topic of what happens to even well-established physicians that spoke up (or spoke out) against the U.S health system’s COVID response as it passed through its initial state of unethical therapeutic nihilism which led to a historically unprecedented ICU mortality, followed by its evolution into a corrupt system of highly profitable therapeutic strategies written by pharmaceutical companies that long ago gained control of our federal health agencies. Whoa is right. If you don’t believe the last sentence, please just look AGAIN at the list below of all the compounds which have shown efficacy in clinical trials from across the world. Now look at the only ones approved for use in the good ‘ole United States of Pharma. I circled them in red for you. See a theme? Not even Vitamin-%&#!-D makes the cut. Insane.
If you want to know how far back this kind of corrupt control of both medical therapeutics and medical education in the United States stretches.. watch this disturbing video about the beginnings of allopathic medicine in the US.
Job 1- University of Wisconsin, Madison. Medical Director of the Trauma and Life Support Center, Chief of the Critical Care Service. Left mid-first surge of COVID April 2020 on a “humanitarian leave” to take over my old ICU in New York City during the latter half of their surge. Resigned while I was in New York City on May 6, just prior to my first Senate Testimony in a Homeland Security Committee hearing brought together and chaired by Senator Ron Johnson where I called out for the critical need for corticosteroids in hospitalized patients, at a time when all national and international health agencies recommended against. The below is why I left to New York, and then why I resigned before coming back.
What happened at the University of Wisconsin is that, after many weeks helping prepare novel physical ICU room layouts along with complex ICU specialist team schedules and structures to deploy in case of a similar massive surge of critically ill patients as was happening in New York City (my hometown), patients started to arrive at UW. First slowly, then more rapidly. Given that COVID was a novel disease to all of us, many were “on fire” trying to learn everything we could about the mechanisms in which the virus was making our ICU patients so ill.. and how best to counteract those mechanisms. And the latter attempt is where my first troubles began.
I want to keep this part brief because it is so sad. Basically, what happened is that very quickly, we (me and my close outside colleagues, in the FLCCC and in other ICU’s in New York and Italy and China) learned that both corticosteroids and anti-coagulation were critical to their survival. The optimal dose, drug, timing or duration for these two strategies were not yet known, but the critical need for them clearly was. Please see my prior post here and here as to how we knew. The problem was that it had not yet been “proven” in some a large, prospective, multi-center, double-blind, randomized controlled trial (RCT), as that is now the only evidence that can make changes to therapeutics in the U.S Health System. The horrific departure of this policy and practice from the long-standing reliance of physicians on the powers of medical knowledge, logic, observation, reason, pragmatism, and the precautionary principle of relying on risk/benefit assessments is now legion. It also quickly led to the most horrific and catastrophic mortality rates of patients in the ICU in history. All because the entirety of U.S academic medicine, over the last 20 years, has been reduced to a “Church of RCT Fundamentalism” (a conversion that was 100% fueled by Big Pharma as they essentially control the funding, design, and.. outcomes of such trials).
This approach was so catastrophic, that not only were centers coming close to and even flat-out running out of ventilators to support patients, one hospital system in New York reported an 88% mortality among their admitted patients on mechanical ventilation. Unprecedented. And they were dying because they were not being treated.. with anything beyond oxygen, fluids, and tylenol (not totally accurate as quite a few doctors I knew were trying different therapeutic approaches, and collecting data the best they could - you know, old-timey medicine stuff). The “official” policies emanating from hospital therapeutic committees were to largely not recommend anything outside of a clinical trial. This “interim guideline” from the American Thoracic Society from that time, should enter the COVID historical doctoring record as being one of the most pathetic. Besides softly recommending hydroxychloroquine only for hospitalized patients with pneumonia (yup - the Ivory tower suggesting an antiviral two weeks into illness, I am not making this up), it made no suggestion for or against 6 other considered medicines. And at UW, I was being repeatedly told and angrily so, “to follow the guidelines” (these were the guidelines being referred to. Sad stuff indeed). Then the Ivory Tower published this chest-pain inducing editorial titled “First Do No Harm” whereby they literally scolded physicians for attempting to treat COVID patients without first waiting for the conclusions of supposedly rapidly enrolling RCT’s, and they wrote to front-line docs observing 88% mortality in their ICU ventilated patients.
They were literally prioritizing medical research ahead of the welfare of patients. In spite of the Helsinki Declaration of 1964 specifically addressing this issue (see Declaration 36). And they did this from the beginning. A horror show. My personal plight fighting the depravity of this approach (as well as the plight of several of my former close colleagues in New York who were trying to do the same) was covered in great detail in this New York Times Magazine article. Highlight of that article was when the Editor of the New England Journal of Medicine called me “lucky” for predicting the critical need of corticosteroids. Yup. Lucky Pierre. The article unfortunately takes on the classic “presenting both sides” approach - you can decide which therapeutic approach you would have wanted as a patient in early COVID. Oh, and keep in mind, this was way before Professor Paul Marik and the FLCCC had identified ivermectin as a highly effective therapeutic in COVID.
I fairly quickly left UW after the first wave of patients, propelled by a series of disturbing incidents:
As the Clinical Service Chief of the Critical Care Service at the time, I led the daily clinical webinar conferences we were having with as many as 50 hospitalists and ICU specialists and residents - these were critical given the massive amount of daily new information, changes to policies, and other unfolding developments. Given my subtle and not-so-subtle advocacy for empiric use of medicines (and avoidance of “early intubation” which many were advocating), my leaders subtly and not-so-subtly “took over” the leading of the calls, emphasizing again and again that doctors should follow that insane non-guidance document above from the American Thoracic Society. It became quickly clear that my clinical expertise and guidance was no longer desired.
My newly minted Chair of Medicine at the time went behind my back and convinced my fellow members of the COVID therapeutics committee to remove intravenous Vitamin C from the University of Wisconsin guideline, after I had successfully scientifically advocated for its inclusion (umm, yes, you read it right.. Vitamin C). She did this on behalf of the Dean of the Medical School at the time (a psychiatrist) who had become incensed when he read a newspaper interview I did where I mentioned that high dose intravenous Vitamin C would likely be critical to improve survival. As soon as I discovered this insane and essentially corrupt action, I immediately demanded a leave. Note that, at the time, the use of intravenous vitamin C was supported by a large RCT, published in a major medical journal which found it led to a massive reduction in mortality in ICU patients with severe lung injury. More recently, a meta-analysis of IV Vitamin C trials in COVID amassed evidence strongly suggesting numerous benefits, including survival. Lucky Pierre strikes again. Moral of the story - this is what happens when psychiatrists decide to dictate the care of ICU patients.
As a native New Yorker I so badly wanted to fight on what was literally at the time, “the medical front lines” of the United States battle against COVID. My email inbox was filling every day with bold headlined emails from all the critical care societies “Critical Care Specialists Needed in New York Urgently”. That’s it, I was going, going, and then I was gonna be gone. I first asked my wife if I could resign, she immediately told me yes, and reminded me how I had become increasingly miserable in the Ivory Tower during my 5 year tenure as Critical Care Service Chief.
This was the email I wrote to my boss asking for the leave.
Humanitarian Leave – I would like to request permission for a leave, for several reasons:
my approach in advocating for a strategy of care for critically ill COVID patients has created discord and tension at a time when consensus and unity are critical. I cannot see how I can be a force in achieving those aims when my clinical judgement and recommendations are in direct opposition to that of divisional, departmental, and Medical School Leadership.
I feel my skill set and effort would be most valuable and have maximum impact if I were to be allowed to support hospitals in New York City that are overwhelmed with critically ill COVID patients
Please note that I am not formally scheduled on a critical care team until the first week of May and I would be willing to return to fulfill that responsibility if desired. Further, I feel that UW Hospital is currently well prepared to care for any surge of patients at this point and my hopes are that an overwhelming surge is being avoided by early and current social distancing practices.
Medical Director/Service Chief position – I would like to offer my resignation from these roles. It has become clear that I am not suitable for these roles.. Just not in my skillset or personality. I deeply apologize for my actions in the past week, actions which were solely intended to rapidly develop an effective strategy of care for COVID patients (I cant remember what they were but I know me and my boss had gotten into our first “argument” during my tenure). The moral distress that I have been suffering over what I “too strongly” perceive as ineffective and inadequate care and needless death has overwhelmed me.
Next night, right after a brief and strained final remote conference meeting with my soon to be ex-Chair of Medicine, I bought a plane ticket to Laguardia.. and off I went.
Please folks, remember:
World-wide Rally for Freedom Day, Sunday January 23 (note we are marching in solidarity with many other countries on that day)
Join us for a March in Washington, DC to protest the numerous harmful infringements of societal and health freedoms that have been implemented in COVID, such as; forced COVID vaccinations of the naturally immune, forced COVID vaccinations of healthy children, and the interference with a physicians ability to care for their COVID patients.
Gather at the Washington Monument by 11:30a.m. Then we will march to the Lincoln Memorial (1 mile) to listen to COVID thought leaders, experts, and activists as they give a series of short, powerful statements. I am one of them.. and I am pumped!
United We Stand, in Peace We March. Bring friends and jackets - and transistor radios in case you come late and/or can’t get close enough to the amplified areas of sound. Given the number of people estimated, cell phone service is unlikely to hold up, even for just radio.
Go to https://defeatthemandatesdc.com/ for details
Finally, I am honored to have been invited by Dr. Chris Martenson and Peak Prosperity to their Annual Seminar as part of a speaker panel including some powerhouse thought leaders. Don't miss it folks. Register using this link: http://peak22.events/kory

"If you want to know how far back this kind of corrupt control of both medical therapeutics and medical education in the United States stretches.. watch this disturbing video about the beginnings of allopathic medicine in the US."
It is heartbreaking to see the you and others who practice medicine destroyed by a corporate drug mafia and hospitals made to serve venture capitalists looking for a maximum return on investment. As you noted the process has been underway for more than a century and it was bound to implode when we have the highest costs and worst outcomes with the sickest, fattest population in human history.
On the bright side the corrupt system is collapsing and we have a clear picture of those who care about human health and saving lives and those who are content with us dying for profits. Never before have so many seen so clearly where the line is drawn and identifying a problem is the first step to fixing it. Big time kudos and thanks for being at the front of the line shining a light for us to follow. Truth will win!!
Yeah. And then you and your team went on to inspire Uttar Pradesh, and many other states and countries around the world. If they'd known how it was going to turn out, Pharma would have much rather left you in place in that hospital, allowing you to use vitamin C, thus minimizing your reach and influence.
Sucks for them,but a good outcome for the world. "Law of unintended consequences."