

Two Texas Children Did Not Die of Measles—By Attorney Aaron Siri and Dr. Pierre Kory
Their deaths were a result of the medical community’s hubris and repeated failures, yet shamefully, the parents were blamed as was (nonsensically) RFK Jr.


At a recent congressional hearing, RFK Jr. was asked a “burning question” about whether he was responsible for the measles outbreak. His response was piercing and addressed two purported deaths from measles – you should watch it:
To further drive Secretary Kennedy’s point, today, Attorney Aaron Siri and I sent a letter to Congress in which we provided critical information concerning both measles infection and the measles vaccine. We also provided the expert medical record review that I published one year ago on this Substack, which detailed the brazen evidence showing that the deaths of the two children were not from measles.
Instead, contrary to the overwhelming media narratives directed at Secretary Kennedy ever since, the deaths proved to be the consequences of grossly inadequate medical care and treatment, which were unrelated to the children’s prior measles infections.
Below is a full text of that letter. My formal medical record review that we submitted to Congress can be read separately and/or downloaded here:
This article was co-authored.
You can follow each author’s work here:
FULL TEXT OF LETTER TO CONGRESS
May 4, 2026
U.S. House Committee on Education and Workforce
2176 Rayburn House Office Building
Washington, D.C. 20515
Re: Follow-up Regarding “Examining the Policies and Priorities of the Department of Health and Human Services” and the Two Child Deaths in Texas
Dear Chairman Tim Walberg and Committee Members,
On April 17, 2026, at the above-referenced full committee hearing, HHS Secretary Robert F. Kennedy Jr. provided testimony concerning measles cases.[1] During your questioning, Chairman Walberg, you asked Secretary Kennedy a “burning question” regarding whether Secretary Kennedy is “responsible for the measles outbreak.” Secretary Kennedy responded as follows:
The measles outbreak began in January 2025 before I took office. Almost 90% of the people affected are over five years old, so … their decision to not vaccinate pre-dated my occupation of this seat....The measles outbreak is not an American phenomena; it is global. It’s happening all over the world. And we’ve done better under my leadership than any country in the world in limiting it. Last year, we had approximately 2,200 cases. Mexico had more than three times that number and they have one-third of our population. Canada had double that number and they have one-eighth of our population. Europe had almost 10 times that number and they only have double [] our population. Many other countries have lost their elimination status. Canada lost it. Britain lost it. These are countries I haven’t visited in years. Many European countries have lost it. Austria and others.
Two little girls died tragically in the Mennonite community in Texas. Mennonites have not vaccinated since 1796. This had nothing to do with me. I went to the funeral of one of those little girls and I spent a day with the family of the other, and both of them told me that when they took their children to the hospital, they were treated as pariahs. They were shamed. They were not given proper treatments. Both families believe their daughters, and their own doctors believe their daughters could have been saved if the hospital gave them proper treatment. The fact that they did not have a proper treatment to give them is regulatory practice by this agency: this agency has been so focused on a single intervention that it does not advise doctors about how to treat people who are actually sick. There’s a lot of people in this country who for religious reasons or other reasons are not going to vaccinate. And I believe that we need to treat them with compassion and understanding and empathy and get them the treatments that they would get anywhere else in the world except for this country.[2]
We write now to provide a fuller picture of these two tragic child deaths in Texas in the Mennonite community—Kaley and Daisy[3]—and to provide more context about measles and the measles vaccine. To date, most sources that have reported on these unfortunate deaths have focused on the fact that the two young girls were unvaccinated. Some shamed their Mennonite parents for not vaccinating their children. Others wielded their deaths as weapons to frighten other parents as well as generate fear regarding unvaccinated children.[4] The media widely and falsely reported that the deaths were caused by measles. The reality is that their deaths were not caused by measles. We have not seen any reports that have told the truth.
And we are sure you will agree that the truth matters. It matters for science. It matters for public policy. It matters legally. And it matters for these grieving families.
Thus, we now provide the details and larger context about these two tragic instances of the loss of a child far too soon—context and facts that the media has not shared and will not share—and, more generally, about measles.[5]
First, attached is a medical record review conducted by Pierre Kory, MD, MPA of these two tragic deaths. In his review, Dr. Kory expands on the testimony provided by Secretary Kennedy and presents clear evidence of what actually caused the deaths of the two children in Texas, and it was not measles. See Appendix.
As Secretary Kennedy’s testimony and these tragic deaths exemplify, when our health authorities focus solely on a single intervention—here, a vaccine—they tend to focus on its benefits (never its risks) and often fail to recognize, diagnose, and treat unvaccinated children for issues unrelated to the vaccine’s target infection. This leads to more tragedy as can be seen in the cases of Kaley and Daisy where their deaths were unrelated to measles but the hospital’s apparent fixation on measles led to the improper treatment of these children. This also leads to blame being cast where it does not belong. Instead of the medical community learning from these two deaths, blame has been and will be cast on the parents and, even more nonsensically, Secretary Kennedy, when the blame for their deaths falls squarely on the mistreatment of these children by the medical community.
This sole focus on the measles vaccine as the “answer” to measles is largely due to the belief that the vaccine has “saved millions of lives” in our country. While this product can prevent transmission of measles and consequently can save some lives by preventing measles deaths, that is not the entire story.
Americans have been repeatedly led to believe that the reduction in measles deaths in the United States was due entirely to the measles vaccine and, had it not been introduced, Americans would have been dropping dead left and right from measles.
For example, the Washington Post reported in April 2025 that at “current state-level vaccination rates,” which were 92.7% nationally by CDC’s last count, “measles could become entrenched, resulting in hundreds of thousands of cases, where deaths are commonplace.”[6] Prestigious medical journals and publications also fearmonger. For example, in a publication about (ironically) vaccine misinformation, the prestigious Royal Society and British Academy falsely wrote that “at the start of the 20th Century, measles resulted in around 530,217 deaths per year in the United States alone.”[7]
These claims flow from beliefs that attribute mythical properties to the measles vaccine. The reality is quite different.
Decline in Measles Deaths Unrelated to Measles Vaccine
The core of measles vaccine worship is the belief that it reduced the death rate from measles in the United States; and that, until the vaccine was introduced, children in the United States were dying en masse from measles. The reality is quite different.
The following official United States government chart shows a decline in the measles death rate by over 98% from 1900 to 1960, three years before the first measles vaccine was introduced in the United States in 1963.[8] Meaning, the measles vaccine had nothing to do with the over 98% reduction in the death rate from measles in the United States from 1900 to 1960.[9]

This chart comes directly from the official mortality report of the United States government.[10] We did not create this chart. The United States government created it based on data collected when there was no measles vaccine that influenced the way in which health authorities reported these numbers.[11]
Taking a slightly closer look, what this chart and official United States government data show is that in 1900, the rate of mortality from measles was 13.3 deaths per 100,000 individuals.[12] By 1960, it was 0.2 deaths per 100,000 individuals.[13] The same was true for 1961 and 1962.[14] Remember, the first measles vaccine came on the market in 1963.[15]
A similar decline of over 99% in measles deaths occurred between 1900 and 1967 in England and Wales, and it was only after that decline that the first measles vaccine was introduced there in 1968—five years after its introduction in the United States.[16]
If you can accept the reality that this is what the official federal government mortality data shows, then you have to acknowledge that something other than the measles vaccine caused this reduction in the measles death rate. Was it better health care? Cleaner water? Improved sanitation? Better nutrition? It is probably a combination of these and other factors.
What is certain is that the data show that the measles vaccine had nothing to do with the over 98% decline in measles mortality from 1900 to 1962.
Pre-Vaccine, 1 in 450,000 Americans Died of Measles
Many also find it difficult to accept that in the several years before the first measles vaccine was introduced in the United States in 1963, there was, according to the CDC, a total of around 400 deaths from measles each year.[17] Not millions. Not even thousands.
Putting 400 deaths per year into context: based on the U.S. population in the early 1960s, that amounted to one measles death for every 450,000 Americans at a time when nearly every American got measles.[18]
Many also cannot accept that the same factors that caused measles mortality to decline by over 98% from 1900 to 1962, no doubt continued to cause a further reduction in the measles mortality rate after 1962. Meaning, at least a portion of the decline in the 400 deaths per year after the vaccine was available is no doubt attributable to the same factors that caused a steady decline in the measles death rate for decades prior to the introduction of the measles vaccine. Therefore, even without the measles vaccine, the death rate would have, no doubt, continued to decline after 1963.
In pockets of the country with poor nutrition, sanitation, and water, deaths from any pathogen, including measles, can occur at a higher rate. Those conditions still existed in some pockets of the United States in the early 1960s. As living conditions in those pockets of America improved with the introduction of clean water, improved sanitation, and better living conditions, deaths from measles declined, which is what typically occurs when these conditions improve.
Let’s also not ignore that health care, especially the management and treatment of acute infections, has vastly improved since the 1960s. Doctors readily concede this point, unless you are talking about vaccines.
That brings us to the next point about measles vaccine. While it can prevent transmission of the measles virus, and therefore prevent some deaths from measles, that is not the whole story. By preventing transmission, the measles vaccine broke the natural ecological relationship humans had developed with measles over millennia; and unlike other pathogens that have come and gone, humans developed this lasting relationship with measles because, as we will discuss, it appears those infected with this virus have a survival advantage over those who did not get infected.
Measles Vaccine Likely Caused More Deaths of Americans Than It Saved
Most people will find what follows difficult to accept. It requires real intellectual rigor because its implications can cause serious cognitive dissonance.
With that, here it is: Studies show that those who have had measles are less likely to die from heart attacks and cancer and are less likely to suffer from various chronic diseases.
The studies supporting this claim were conducted and published after federal health authorities had already committed to the measles vaccine program. This may explain the reluctance to accept these findings and why this is likely the first time you will learn about these studies. But none of that can change the reality of their existence.
In one of these studies, and it was a massive study, the nation of Japan followed over 100,000 of its citizens for approximately 21 years. They found, among other things, that those who had been infected with measles and mumps had a statistically significant lower risk of death from cardiovascular disease, strokes, and heart attacks.[19] For example, men who had measles and mumps (as compared to those who did not have measles and mumps), had a 17% reduction in strokes, 20% reduction in cardiovascular disease, and 29% reduction in heart attacks.[20] Critically, after 21 years, approximately 7% of the men who had measles and mumps had died of cardiovascular disease while approximately 14% of the men who never had measles or mumps died of cardiovascular disease.[21] Meaning, the men who never had measles and mumps were far more likely to die. The statistically significant findings in this study remained statistically significant even after adjusting for all kinds of variables (including age; body mass; family history of cardiovascular disease; alcohol intake; energy intake; smoking; walking; sports; mental stress; education; and history of hypertension, cardiovascular disease, or diabetes).[22]
Cardiovascular disease is the number one killer of Americans, taking the lives of over 900,000 Americans a year.[23] In contrast, as discussed above, according to the CDC, around 400 Americans died of measles annually in the several years before the first measles vaccine arrived in 1963 (and remember that number was declining without a vaccine), and around 40 Americans died annually of mumps in the several years before the first mumps vaccine was introduced in 1967.[24]
Putting this together, what this robust and extremely reliable prospective study spanning 21 years with over 100,000 individuals reflects is that the use of the MMR vaccine to prevent measles and mumps may have resulted in multiple times more annual deaths in the United States from cardiovascular disease than it could have possibly saved from measles and mumps.
That is an incredible reality. Even more incredible is that nobody has done any study showing otherwise. The evidence that “health” authorities have messed with nature to save a few but may have caused far more deaths from heart disease is not something they would likely ever acknowledge.
This Japanese study shows why measles, unlike most pathogens, may not have died out over time through natural selection. It is because having measles appears to confer a survival advantage. Meaning, people who had measles were more likely to survive and procreate and not vice versa.
Similar to the finding regarding heart disease, some studies, although not nearly as robust, have found that eliminating measles appears to have caused a measurable increase in certain cancer rates. For example, the International Agency for Research on Cancer found that those who never had measles had a 66% increased rate of non-Hodgkin lymphoma and a 233% increased rate of Hodgkin lymphoma.[25] These two cancers are expected to kill an estimated 20,540 Americans in 2025.[26] There are even studies documenting children with Hodgkin’s disease experiencing remission when having measles.[27]
Likewise, researchers at the Department of Health Care and Epidemiology at the University of British Columbia and the Department of Biology at the University of Victoria found that those who never had measles had a 50% increased rate of ovarian cancer, which is expected to kill an estimated 12,730 Americans in 2025.[28]
Other studies have reached similar conclusions that measles, as well as mumps, rubella, pertussis, and chickenpox, reduce the rate of various forms of cancers, including a study from researchers at the University of Berne, Switzerland that specifically reviewed these fever-inducing (i.e., febrile) infections and found that the “study consistently revealed a lower cancer risk for patients with a history of FICD [febrile infectious childhood diseases].”[29] And as an article in The Quarterly Review of Biology explained,
Detailed retrospective and prospective clinical studies … supported the conclusion that frequency of the infectious fever episodes and cancer diagnoses are inversely related (Abel et al. 1986; Mastrangelo et al. 1998; Kleef et al. 2001; Kleef and Hager 2006). For example, Grossarth-Maticek et al. (1987) performed a 10-year prospective cohort study of 1353 patients, concluding that episodes of high fever as a typical reaction to an acute illness during the entire life span are inversely related to later cancer incidence. Kölmel et al. (1992), based on 271 controls versus 139 melanoma patients, demonstrated an inverse relation between the number of febrile infections and the incidence of malignant melanoma. Similarly, Wrotek et al. (2009) have reported a lower frequency of fever in a population of 355 breast tumor patients, compared to 244 healthy women volunteers.[30]
This article also explained how a survey of studies of spontaneous cancer remissions found that “approximately 70% of documented cases [of remission] were immediately preceded by an acute infection associated with high fever” and that this phenomenon has “been reported for centuries.”[31]
If that were not enough, studies have found that children who have had measles have far fewer allergies and atopic diseases, such as asthma, and adults who have had measles have a reduced risk of Parkinson’s disease.[32]
The bottom line is that, prior to the introduction of the vaccine, measles was considered a mild childhood infection, like chickenpox. The ecological relationship humans developed with measles through millennia did not eliminate measles; and having had measles confers survival benefits that appear to far exceed the infection’s negative effects.
We raised these studies at a court hearing in which we challenged violations issued by the New York City Department of Health to families that refused to give their child an MMR vaccine. The vaccine expert for the health department was a medical doctor and the Director of Epidemiology and Surveillance in its Bureau of Immunizations. When confronted with these studies, she had no retort.[33] When we reconvened for a second day of hearings in the case, 28 days later, she still had no response to these studies and not a shred of evidence to oppose their findings, nor did the health department offer a shred of evidence to the contrary on appeal despite the fact it offered an extensive affidavit of additional medical information.[34]
Another Unintended Consequence
Another unintended consequence of the measles vaccine is that for anyone infected today in the United States, it has made measles more of a concern. This is because, before the use of the measles vaccine, mothers who were previously infected with the measles virus provided passive immunity to their babies, and that immunity protected them from measles in the first months of life.[35] Moreover, adults were protected because they almost always were infected with measles as children. This natural protection was critical, since measles poses the greatest risk to infants and adults.
The measles vaccine, however, does not afford the same protection as having had measles. A mother who has only had the measles vaccine, as opposed to the natural infection, will confer only limited protection to her baby.[36] As for adults, 2% to 10% of them, depending on which study you look at, will not develop immunity even after two doses of measles vaccine.[37] And for those who develop immunity from the vaccine, a joint CDC and FDA study found that the vaccine immunity wanes over time. [38]
The measles vaccine thus reversed the declining virulence of measles, including by making vulnerable groups—infants and adults—who had generally been protected in the pre-vaccine era, now potentially vulnerable to measles. It also upended the natural decline in the virulence of this virus since 1900 and broke the natural ecological relationship humans had developed with measles which, as we reviewed, studies reflect conferred a survival advantage to those who had measles as children.
Belief in Measles Vaccine Runs Deep
The simple statistical reality laid out above causes incredible turmoil to many people. Some get angry, while others simply cannot accept reality.
Even some of the most prestigious publications in the world rely on religious beliefs, not evidence, when writing about this product. For example, BMJ, a leading international medical journal, published an article by a distinguished Oxford professor who wrote “Vaccination is a miracle of medicine,” described “vaccine disinformation” as “incorrect beliefs,” and argued that anyone holding incorrect beliefs should be criminally prosecuted.[39] Ironically, under this Oxford professor’s own standard, she would have to be criminally indicted. This is because in her article about vaccine misinformation, published by The Royal Society and The British Academy, she asserts on the very first page that “at the start of the 20th Century, measles resulted in around 530,217 deaths per year in the United States alone.”[40] Looks like it is time for handcuffs because this statistic is categorically false.
According to CDC data, approximately 10,150 Americans died from measles in 1900.[41] That is obviously far fewer than the article’s claimed 530,217 deaths. Compounding this falsehood, the article then attributes the annual decline in measles deaths since 1900 to the measles vaccine.[42] This is also categorically false for reasons you now know. The article also ignores the impact eliminating measles may have had on mortality from heart disease, cancer, and other health issues. Ironically, under the Oxford professor’s own standard, she should be criminally prosecuted for this plainly false information about the measles vaccine.
Critically, overstating the benefits of the measles vaccine can be dangerous. It deprives medical professionals and individuals of their ability to weigh the benefits against the risks for each patient of a given medical intervention. But overstating the benefits of the measles vaccine is the norm. Just as understating its risks is the norm.
Safety of the MMR Vaccine
As for the safety of the MMR vaccine, Merck’s MMR vaccine in use today (MMR-II) was licensed in 1978 based on a clinical trial with 834 children, no control group (let alone a placebo control), and only 42 days of safety review after injection.[43] During the trial, approximately one-third of the participants developed gastrointestinal issues and one-third developed respiratory issues but without a control group, these and other reactions were written off.[44] This means that even if this trial did have enough children (which it didn’t) and reviewed safety long enough (which it didn’t), without a control group, it was useless for determining the vaccine’s actual safety profile.
Just to be clear, MMR-II’s clinical trial did not even use another vaccine as a control. It simply had no control group. To be clear, it did not even test against the first MMR vaccine.
The importance of a proper trial to study the safety of MMR-II also cannot be overstated. This was a novel product. For example, unlike any prior measles-containing vaccine, in the vial of every dose of MMR-II there are, according to the data and even Dr. Stanley Plotkin, hundreds of billions of pieces of human DNA and cellular material from the cultured cell line of an aborted fetus.[45] But even without this novelty, a proper safety trial should have been conducted prior to licensing MMR-II. That never happened.
Over the years, as liabilities from harms related to measles-containing vaccines piled up, the number of companies making and selling this product dropped from at least six companies in the 1970s to only one company by 1986—Merck selling its MMR-II. Remember, MMR-II was one of only three routine vaccines at the time that led to the passage of the 1986 Act which gave Merck immunity from liability for harms caused by this product.[46] It needed this immunity, no doubt, including because after passage of the 1986 Act, the CDC published the Vaccine Information Sheet for this product and admitted that “after MMR vaccination, a person might experience” “seizure,” “deafness,” “long-term seizures, coma, or lowered consciousness,” and/or “brain damage.”[47] As an aside, after Dr. Plotkin was deposed by the undersigned, his subsequent herculean efforts to cover up vaccine harms included having “brain damage” removed from MMR’s Vaccine Information Sheet.[48]
In any event, decades later there was a clinical trial that included Merck’s MMR-II vaccine as a control. It was a trial for a new MMR vaccine to be sold by GSK called Priorix, licensed in 2022 (MMR-RIT). This trial had 6 months of safety review after injection. So, what did this trial find? Sadly, both vaccine groups had a high rate of serious adverse events, emergency room visits, and new onset of chronic diseases (e.g., autoimmune disorders, asthma, type I diabetes, vasculitis, celiac disease, thrombocytopenia, and allergies) as reflected in the chart below which was buried in the supplemental information for this clinical trial:[49]

The damning findings in this clinical trial, showing an incredibly high rate of serious adverse events and new chronic health conditions after receipt of an MMR vaccine in previously healthy children, should have raised alarm bells. Instead, MMR-RIT was deemed safe by the FDA because it had the same level of harm as the control group receiving MMR-II. But to any thinking, breathing, caring person, certainly not safe.
Worse, these serious harms were not disclosed in the package insert given to medical professionals, parents, or the public. Nor were they mentioned in patient-facing materials. Instead, GSK buried them in a supplemental table in a journal article.[50]
* * *
In sum, given the above, it should be patently clear that the decision of whether or not to inject a measles vaccine into oneself or one’s child is an important one and one that is entitled to informed consent. And there undoubtedly will be individuals who decide that, for them or for their child, the risks outweigh the benefits. These people are equally as deserving of respect, adequate medical treatment, and the truth.
Thus, we ask, first, that you immediately cease spreading, or allowing to be spread, the false claim that these two young girls died “from measles” as that is not the truth (see Appendix), and, second, that you acknowledge that a singular focus on vaccination to the exclusion of other preventatives and treatment is inappropriate and inadequate. It might be great fodder for fear mongering but the American public and these two grieving families deserve better—they deserve the truth.
Very truly yours,
Aaron Siri, Esq.
Elizabeth A. Brehm, Esq.
Expert Medical Review by Pierre Kory, MD, MPA
I have long reviewed medical records of patients harmed by poor medical care. Here, I expand on the testimony provided by Secretary Kennedy and I present clear evidence of what actually caused the two girls’ deaths in Texas and. It wasn’t measles.
I obtained and conducted a thorough review of the medical records of the two girls. Both of the girls died in an ICU of end-stage lung failure. As a pulmonary and critical care specialist who has researched and managed lung failure for my entire career, I am highly qualified to serve as an expert reviewer for these cases.[51] I served as the Chief of the Critical Care Service and Medical Director of the Trauma and Life Support Center at the University of Wisconsin for over 5 years.
While drafting this expert summary report, I aimed for a sober, objective, and professional approach to be read (and likely heavily critiqued) by the public, but also added extensive “rolling” commentary for the layperson so that my evaluation is understandable.
To be clear, it is my professional opinion that neither child died of measles. It’s not a close call; they did not die of measles.
CASE #1 - Kaley, Age 6
The records and findings related to Kaley’s case are straightforward.
Kaley was a six-year-old, previously healthy girl who contracted measles along with her four siblings (all of whom weathered the illness just fine under the care of Dr. Ben Edwards). As her rash was clearing, she began to develop signs and symptoms of “secondary bacterial pneumonia,” a not uncommon complication of almost any viral infection. To wit, one of my three daughters fell ill with the same after she contracted influenza at age 14; however, in her case, she recovered from it two days after receiving an appropriate antibiotic.
In Kaley’s case, her worsening respiratory status led her parents to bring her to Providence Covenant Children’s Hospital in Lubbock, Texas, on February 22, 2025 at 12:08 PM.
The hospital correctly diagnosed her with secondary bacterial pneumonia and then treated her with two antibiotics, ceftriaxone and vancomycin. This was a blatant deviation from the standard of care in treating hospitalized patients with “community-acquired pneumonia (CAP),” the guidelines for which have long recommended a different combination, e.g., ceftriaxone and azithromycin (or a quinolone).
Only azithromycin and quinolones cover mycoplasma pneumonia, a prevalent cause of community-acquired pneumonia (which is why the guidelines recommend them). Neither ceftriaxone nor vancomycin will treat mycoplasma because they work by disrupting the cell walls of bacteria. Mycoplasma does not have a cell wall.
Vancomycin, the antibiotic they chose instead of azithromycin, is used to treat “hospital-acquired pneumonia” as it is one of the only antibiotics that covers MRSA (methicillin-resistant staph aureus). This common organism inhabits hospitals and medical facilities. Kaley was from a rural Mennonite community and had not been in any hospital.
Despite her persistent and increasing deterioration in respiratory status, which eventually led to requiring intubation and mechanical ventilation, this deviation from the standard of care went unnoticed and uncorrected until just over a day before she died, when the test for mycoplasma returned as “positive.”
Azithromycin was then immediately ordered. However, from the chart, it appears it took ten hours before she received her first dose (documentation of the exact time may be missing). She passed away less than 24 hours later, 4 days after being admitted. The time of death was 06:43 on February 26, 2025. My opinion as to the cause of death is that it was from an overwhelming lung injury called Acute Respiratory Distress Syndrome (ARDS) caused by mycoplasma pneumonia. The sole reason why she died from mycoplasma was because the initial antibiotic regimen violated the standard of care in the treatment of hospitalized community-acquired pneumonia because they neglected to treat her upon admission with azithromycin (i.e., a “Z-Pak deficiency”).
Note that azithromycin has excellent penetration into lung tissues and is highly effective at treating mycoplasma. Again, had they started azithromycin on Day 1, as has been recommended for decades, she would still be alive today.
The above findings were articulated by me in an interview on March 19, 2025,[52] but were subsequently ignored and/or distorted by the mainstream media. A reporter from USA Today reached out to Rebuild Medicine (my non-profit[53]) with questions. This is the exchange between my Executive Director, Steve, and the reporter, Eduardo:
From Eduardo: Good morning, Steve! Yes, we were more so looking for proof around the determination of medical error. Are any of these records being inspected elsewhere? Or is there litigation on this?
From Steve: …Dr. Kory, a pulmonologist and former ICU doctor, refers to the attending physician not following the guidelines of the major medical societies for treating mycoplasma pneumonia. Two examples of guidelines are Table 4 of the American Academy of Family Physicians guidelines for Community-Acquired Pneumonia. And the Infectious Disease Society of America Guidelines: Dr. Kory also discusses the errors in more detail in this interview. I recommend watching this if you haven’t seen it. It is about 15 minutes long. We don’t know if others have reviewed the records. The girl’s family has said that they intended to allow CHD access to the records and make the conclusions public so others could learn of the errors and ensure they are not made again. We are not aware of any litigation plans. I’m glad to arrange a conversation with Dr. Kory if you’d like.
The above text also included links to several CAP guidelines, yet, in the USA Today article subsequently published about the case,[54] the reporter 1) attacked my credibility by stating that I “spread[] misinformation during the COVID-19 pandemic”, 2) did not even mention the treatment guidelines for community-acquired pneumonia that we had sent him, and 3) included parts of this below statement that the hospital released in response to my video interview. The mendacity of the below statement is astonishing:
“A recent video circulating online contains misleading and inaccurate claims regarding care provided at Covenant Children’s. Patient confidentiality laws preclude us from providing information directly related to this case. What we can say is that our physicians and care teams follow evidence-based protocols and make clinical decisions based on a patient’s evolving condition, diagnostic findings, and the best available medical knowledge. Measles is a highly contagious, potentially life-threatening disease that often creates serious, well-known complications like pneumonia, encephalitis and more.”
In sum, Kaley did not die of measles but rather because of the gross negligence of the hospital to properly diagnose and treat a very common cause of bacterial pneumonia.
CASE #2 - Daisy, Age 8
Daisy’s medical records that I reviewed totaled 291 pages and came in 6 separate PDF files, none of which were in chronological order. It represented the total record for two separate admissions to the ICU of University Medical Center and one to Providence Covenant Children’s Hospital, all located in Lubbock, Texas.
My assessment here begins with my determination of the cause of death during Daisy’s last admission. Then, I will provide details of the multiple poorly managed hospitalizations (understatement) that she suffered over the 4 weeks leading up to her death.
Cause of Death
Daisy’s cause of death was ARDS secondary to hospital-acquired pneumonia caused by a highly antibiotic-resistant E.Coli “superbug.” Based on the progression and trajectories of Daisy’s illness, I believe that she contracted the infection from her first ICU admission, which is what caused her to return to the ICU 2 days after that discharge.
Although the ER physician started Daisy on antibiotics (again with ceftriaxone and vancomycin – but here, the vancomycin was a good choice because she just got out of an ICU), however the admitting ICU team discontinued them.
One of the tragedies (there were multiple) of this case is that the ICU team in charge of Daisy’s care when she was re-admitted never considered the possibility of hospital-acquired pneumonia (HAP) until day 6 of 8. For an adult ICU specialist admitting a patient with an infection who was just discharged from an ICU, empiric treatment for hospital-acquired organisms is so basic and routine that it is shocking that they failed to do this.
In a minor defense of the pediatric team caring for Daisy, there are no published national treatment guidelines in pediatrics with specific antibiotic recommendations for the empiric treatment of hospital-acquired pneumonia (there is one from the University of North Carolina (UNC) however). The first adult guidelines for HAP were published by the American Thoracic Society in 2005. Here we are 20 years later, and, aside from UNC, the field of pediatrics has not gotten around to doing the same. I found a paper by the Cochrane Library that proposed the methodology for creating one, but although published in 2019, it has not yet been completed. The American Academy of Pediatrics should be ashamed.
The problem for the hospital in Daisy’s case is that the absence of a treatment guideline is not why she died. Their error was much more basic. They simply failed to send a sputum culture on admission. Had they done so, they would not only have identified the organism by Day 3 but also would have learned the antibiotic it was sensitive to and thus could have started appropriate antibiotic therapy immediately. Her death on Day 8 would have likely and easily have been prevented. Although they did send a urine culture, a blood culture, a viral PCR respiratory panel, and a PCR for MRSA and Staphylococcus (all of which were negative), they did not send a sputum culture—for a child with pneumonia.
For the sake of brevity, each time I detail a deviation from the standard of care in the below review of all three hospital stays, rather than explaining why it violates the standard in depth (and because I trust it will be evident to even laypeople), I will call it a failure. The failure to send a sputum culture in a patient with pneumonia who recently spent days in an ICU is Failure 1.
The failure to send a sputum culture had another tragic consequence - it allowed the care team, based on the viral respiratory panel being negative (which does not include measles PCR, by the way), to instead 1) assume that measles was the underlying cause on Day 2 and then, 2) immediately stop antibiotics in a seriously ill and infected child. Failure 2.
In the 8 days of her second hospital admission, Daisy only received 5 days of antibiotics, and that is because, despite a rising white cell count in her blood, they did not restart antibiotics until Day 4, when she spiked yet another fever. Failure 3.
Further, during the three days Daisy received no antibiotics, she was given high-dose steroids. Please note that steroids, when paired with appropriate antibacterials, improve outcomes in pneumonia, but giving them without appropriate antibacterials worsens outcomes. They presumably did this because their working diagnosis was “measles pneumonitis,” not bacterial pneumonia. The doctor in charge kept writing things like: “severe pulmonary sequela of measles infection around 3 weeks ago” and “we are concerned that the true extent of her lung injury due to measles is unknowable and it may be an end-stage process given the span of illness and the fact she truly is an outlier.” I don’t know what that last part means except that the clinical reasoning is unclear, and a broader “differential diagnosis” was not generated—at all.
I have long taught my ICU residents and fellows the two guideposts that governed my care plans for critically ill patients. The first is, “If what you are doing is working, keep doing what you are doing.” This means that if their clinical trajectory was one of slow or steady improvement, sending endless diagnostic tests or adding therapies just because they were still ill is most often unnecessary.
The second is, “If what you are doing is not working, change what you are doing.” In this situation, I would re-review all the clinical data and further explore any causes I might be missing, or I would add on treatments that, although not standard, might offer benefit. I would try anything that might turn someone around, as long as the risk/benefit profile was favorable (when someone is persistently deteriorating, risk/benefit ratios change rapidly such that almost any treatment that holds the possibility for benefit is worthwhile to prevent death).
With the above in mind, I was encouraged by the one instance in which I found the team “thinking outside the box” and trying a somewhat experimental treatment. They decided to give Daisy intravenous immunoglobulin (IVIG). One trial from China in 2015 found that IVIG improved outcomes in children with severe pneumonia (not measles-specific),[55] and another study found that IVIG batches tested in 2021 contained measles-neutralizing antibodies.[56] While I respect that they tried something “off protocol,” the problem was that they did not give her the IVIG until Day 7, one day before death, and further, it was a treatment for the wrong disease.
Also, it was not until one day after re-starting antibiotics (Day 6) that they sent a sputum culture (Failure 4 - standard practice is to send a culture at the same time you start antibiotics). This was also the first time that the thought that she might have HAP appeared in the record. This thought led them to then change her antibiotic to one that is routinely used for possible HAP (ceftazidime). Problem: The adult guidelines would have dictated that they start Imipenem or Meropenem, but since they don’t have a pediatric guideline published yet, I will not count this as another failure.
Two days later, on Day 8, Daisy died of refractory hypoxemia - they could no longer get oxygen into her blood via her lungs despite numerous heroic mechanical ventilation maneuvers.
A few hours after Daisy’s death, the results from the sputum culture they sent on Day 6 was reported in the record and they were jaw-dropping: they showed 4+ growth of “E.Coli,” a nasty bug generally found only in our GI tract. If you are not familiar with what 4+ means, see this chart below, which explains the “semi-quantitative growth scale” for bacterial cultures:
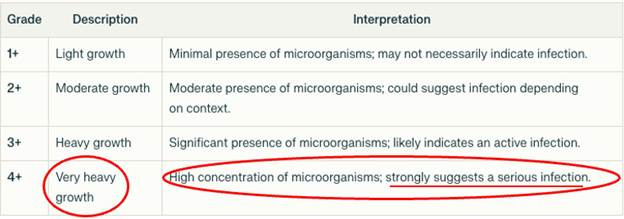
It gets worse: next came the panel of susceptibilities to a slew of antibiotics: Ampicillin - Resistant, Ampicillin/Sulbactam - Resistant, Aztreonam - Resistant, Cefazolin - Resistant, Cefepime - Resistant, Cefoxitin - Resistant, Ceftriaxone - Resistant, Cefuroxime- Resistant, Ciprofloxacin - Resistant, Levofloxacin - Resistant, Piperacillin - Resistant, Tetracycline - Resistant, Tobramycin - Resistant, and finally and tragically, Ceftazidime- Resistant.
Daisy’s infection was sensitive to only a handful of antibiotics, one of which was meropenem, which is what would have been recommended by the Adult HAP Guidelines. Daisy had numerous risk factors for HAP (previous antibiotics, previous ICU, immunosuppressed, really sick, mechanically ventilated). In conclusion, an appropriate differential diagnosis for Daisy’s pneumonia did not occur until Day 5, and a sputum culture was sent too late for them to discover that the organism that Daisy was dying from was resistant to the antibiotic they had selected.
In the two hospital admissions Daisy underwent the week before the above “final” admission, the same pattern of error-prone care and missed opportunities to save her life was present.
Hospital Admission At UMC 2 Days Before Daisy’s Final ICU Stay
In this hospitalization, which began on March 21, 2025, 6 days before the above admission, Daisy presented with typical symptoms of pneumonia along with a chest x-ray showing a left lower lobe process, classic for bacterial pneumonia. Her admitting diagnosis was “viral illness with probable secondary bacterial pneumonia.” Just as in Kaley’s case at Covenant Hospital, UMC also decided to treat Daisy with the same inexplicable and standard-violating combination of ceftriaxone and vancomycin. Failure 1. However, Daisy did not suffer the same fate as Kaley because whatever bug was making her ill at this point appeared to be sensitive to this combination, plus her mycoplasma test later turned out to be negative. This was a near miss though.
Although the mother was unaware that Daisy had a subtle rash on her back on admission, the ER physician suspected it was measles and sent off a PCR test, which returned positive on the day of discharge. Daisy had measles too.
She was pretty sick lung-wise at first because she required admission to the ICU for oxygen support. However, her oxygen requirements decreased pretty quickly, her appetite improved, her rash began to “heal and fade,” and she was discharged home on oral antibiotics on Day 4. They prescribed her oral cefdinir, which was a fine choice, because she had responded to ceftriaxone in the hospital (a similar antibiotic).
Problem: in the discharge note, the doctor documented that “the parents appeared concerned” with the discharge and then reported that he/she had “reassured them.” Privately, Daisy’s father told me that was the same day her measles test came back positive, and he thinks that is why they sent her out so quickly. He felt she “didn’t look too good” and was concerned. It seems her father was correct based on the fact that she quickly began to get worse after arriving home such that, 2 days later, on March 26, 2025, she had to return to the ER to be readmitted with what turned out to be the fatal E.Coli pneumonia episode detailed above. It appears to me that Daisy was beginning to fall ill with E.Coli pneumonia as she was being discharged (resistant to the cefdinir she left with).
Admission to Covenant Hospital Two Days Prior to the Above UMC Admissions
I will now go back in time so I can provide the timeline from the beginning of Daisy’s illnesses.
Daisy had a history of chronic tonsillitis and was being scheduled for a tonsillectomy. A month before her death, as per Dr. Richard Bartlett, Daisy was diagnosed with mononucleosis and developed persistent fevers, which continued throughout the month, including during all her hospital admissions. Daisy’s father told me that at one point in the first few weeks, she was also diagnosed and treated for strep at another facility. Then, late in the third week of her illnesses, she was admitted to Covenant Children’s Hospital in Lubbock, stayed one night, and was discharged. Two days later, she was admitted to UMC for the first of her two hospital admissions there.
The reason her one-night stay at Covenant prior to her UMC admissions is relevant is because had she been appropriately treated there, she would never have ended up at UMC, and all of the above would have been avoided.
Briefly, on March 18, 2025, Daisy was at a community health clinic where they found her to require oxygen, so she was sent to the ER. She complained of difficulty breathing, abdominal pain, nausea, and inability to eat and was found with thrush on exam. She had a recent Tmax of 103.7. A CT scan of the abdomen and chest was done, which found splenomegaly and a left lower lobe pneumonia surrounded by a small amount of fluid (e.g., a pleural effusion).
Daisy was given IV ceftriaxone (no azithromycin), corticosteroids, a breathing treatment (albuterol), and a painkiller (Toradol). This occurred in the ER and I have not had access to the records from the ER, only the hospital stay. Daisy was then admitted to Covenant Children’s Hospital with the diagnosis of pneumonia with a “plan to transition to oral antibiotics in the a.m.” Failure 1 for the absence of azithromycin in her regimen. (Note: this is the third hospital at which this failure has happened in my reviews of these cases). No sputum culture was ordered, although a blood culture was. Failure 2.
Daisy was given oral amoxicillin and IV ceftriaxone (unnecessarily redundant coverage but not a failure), Motrin, and Tylenol (although not ideal, this is not a failure because, although the literature strongly supports the fact that fever reducers are harmful in children with infections, their use is so ubiquitous, it is unfortunately “the standard of care” and has been for decades). By the next day, Daisy’s oxygen levels had improved, and she was eating decently, so Covenant Children’s discharged her. The problem is that the only medication she was discharged with, per the record, was the anti-fungal drug nystatin for the thrush—no antibiotics for her pneumonia, despite the note in her record from the previous day clearly stating that the plan was to “ transition to oral antibiotics in the a.m.” Failure 3.
It is unclear to me what Daisy’s healthcare providers were thinking. The only possible defense is that someone forgot or was unaware of what the CT showed (it appears the ED is separate from the hospital), and instead went by the chest X-ray (CXR) they did in the hospital, which, tragically for Daisy, did not reveal the pneumonia, which is not surprising because CT’s are far superior at diagnosing pneumonia than CXR’s. It is also unclear why one would do a CXR on Daisy the same day she had a CT.
I suspect the CXR caused the problem because it only revealed bronchial wall thickening. It missed the lower lobe process seen on CT. The radiologist stated in his report that “bronchial wall thickening can be seen in asthma or viral illnesses.” This was likely the reason they did not discharge Daisy on antibiotics.
Summary Of All That Happened to Poor Daisy
Daisy became ill with mononucleosis a month before her death, soon followed by a strep infection and then thrush. Fevers persisted throughout, and then three weeks after the mono diagnosis, she was admitted to Covenant Children’s, diagnosed with left lower lobe pneumonia, and treated successfully. However, she was sent home without oral antibiotics. Unsurprisingly, two days later, she was admitted to UMC’s ICU with measles and a worsening of her left lower lobe pneumonia, which was again, despite errors in antibiotic selection, successfully treated; she was then discharged (on an appropriate antibiotic) despite concerns by her parents over her condition. The measles rash was clearing at this point. Then, two days after discharge, Daisy was re-admitted to UMC’s ICU with a worsening CXR (now involving her right lung) and severely worsened oxygenation. Although the ER gave Daisy broad antibiotic coverage, instead of suspecting a severe hospital-acquired bacterial pneumonia and sending a sputum culture, the ICU team’s presumptive diagnosis was that her lungs were failing from measles pneumonia, and so her antibiotics were stopped. She was instead given corticosteroids for “measles pneumonitis.” She continued to deteriorate despite their re-starting antibiotics on Day 4 and giving IVIG on Day 7. She died on Day 8 from what a few hours later was discovered to be a large amount of E.Coli in her sputum that was highly resistant to the antibiotics she was on.
I largely (and atypically for me) left out the many strong emotions I felt while writing this review. However, these cases are being widely and repeatedly portrayed as “measles deaths” by a biased press in an attempt to regenerate enthusiasm for vaccines by instilling exaggerated fears of measles which is, in most cases, benign and most complications can be easily treated with competent medical care. If the media continues this fear-mongering by using cases of non-measles deaths, public trust will plummet even further than it already has post-Covid.
Pierre Kory, MD, MPA

{kind=link}
Thanks, Dr. Kory. I could hardly read through some especially knowing when I was a child everyone got measles!!! Both kinds and lived. I started first grade 1953! I don’t remember one child dying in the schools I attended in KY for 6 years before we returned to our home state Alabama. Also some had measles before they started school. It wasn’t a big deal back then. I think good hygiene, sanitation and clean water made a big difference but didn’t stop us from getting them. It reads like malpractice to me. “Do no harm”! That means little children also. We are worse off with the vaccines. Thanks again for all that is being done to help us be a healthy nation again.
Please, there wasn't an uptick in measles until Biden let in some 30 million people, unvetted.