

The Numerous Mechanisms Of Action Of Chlorine Dioxide In Treating Human Illness
Here I detail the numerous mechanisms of action of chlorine dioxide in the human body which make it a viable treatment in a broad array of human illnesses.

Electron micrograph of Yeast Cell Wall.
REVIEW OF THE MAIN MECHANISMS OF CHLORINE DIOXIDE
Let’s do a brief scientific review of the mechanisms behind “oxidative therapies” which, besides chlorine dioxide, also include ozone, hydrogen peroxide, high dose IV Vitamin C, methylene blue, HBOT, etc.
OXIDATIVE MECHANISMS
How does oxidation work in treating illness, especially infection? To review from prior posts, “oxidating” a compound simply means that it is made to lose electrons. That is done by "an “oxidizing agent” which is able to accept the electrons. When an electron is lost by a compound, it becomes a “free radical” which, among other of its capabilities, can then “steal” a hydrogen atom from the fats (lipids) that are in cell membranes.
When a lipid loses a hydrogen atom, this is called “lipid peroxidation.” It becomes a “lipid radical” which can then grab a hydrogen atom from a neighboring lipid, starting a “chain reaction” which essentially “unravels” the fatty membrane. This leads to disruption of the structure and function of the membrane, increased permeability, loss of membrane integrity, and cell lysis. Boom.
At the risk of repeating myself from prior posts, although the word chlorine is in its name, chlorine dioxide is NOT a “chlorinating agent” like bleach because at no time in its formation or breakdown is a free chlorine ion produced. Chlorinating agents like bleach work by an additional mechanism whereby the chlorine atom enters directly into organic molecules which alters membrane integrity and disrupts enzyme function. The problem with chlorinating agents like bleach is that they produce harmful organic compounds which are carcinogenic.
However, non-chlorinating oxidative therapies such as chlorine dioxide have a comparatively excellent safety profile and is why they are widely used as disinfectants and purifiers in food and water. Although in this post I am solely focusing on its mechansims, I previously reviewed all aspects of the safety of therapeutic doses in this post.
Anti-bacterial mechanisms: chlorine dioxide interacts intricately with sulfur-containing compounds that are abundantly found in various bacteria. This interaction disrupts the metabolic processes of these microorganisms, effectively inhibiting their reproduction and growth. Remarkably, at lower concentrations of 0.25 mg/L, CD can eradicate 99% of E. coli (15,000 cells/mL) within a mere 15 seconds.
Anti-fungal mechanisms: causes significant damage to fungal cell membranes. This damage leads to the leakage of intracellular components such as potassium ions (K⁺) and adenosine triphosphate (ATP), suggesting that ClO₂ disrupts membrane integrity.
Anti-viral mechanisms: ClO₂ inactivates viruses by oxidizing specific amino acids, such as cysteine, methionine, tyrosine, and tryptophan, in viral proteins. This oxidative modification leads to protein denaturation, impairing the virus's ability to infect host cells. ClO₂ reacts with viral components, including proteins and genetic material. These reactions compromise the virus's structural integrity and functionality, leading to its inactivation. In its gaseous state, ClO₂ can penetrate the outer shells of encapsulated viruses, leading to their inactivation.
OXYGEN DELIVERY MECHANISMS
Oxidative therapies can also improve oxygen delivery to tissues by breaking down into oxygen (02) which then diffuses into tissues. They can also stimulate 2,3 BPG which helps hemoglobin more easily release oxygen. They can enhance the flexibility and deformability of RBC’s so they can more easily pass through the smallest blood vessels. Finally they can cause dilation of blood vessels (by stimulating nitric oxide), thus improving blood flow.
Further to this end of improving oxygen delivery, oxidative therapies can reduce blood viscosity (thickness/sludging) which also improves blood flow and oxygen delivery. They reduce blood viscosity via:
Breakdown of fibrinogen and other proteins (hmm, spike protein anyone?).
Inhibition of platelet aggregation (modulation of NO and prostacyclin).
Breakdown of microthrombi and clots (oxidation of fibrin).
Improved metabolic waste clearance (oxidation of toxins and waste products).
Modulation of lipid profiles (oxidation and clearance of lipids).
In regards to the Sars-CoV2 spike protein, from this paper, “ClO2 has the ability to oxidize the cysteine residues in the spike protein of SARS-CoV-2, inhibiting the subsequent binding with the Angiotensin-converting enzyme type 2 receptor, located in the alveolar (lung) cells.”
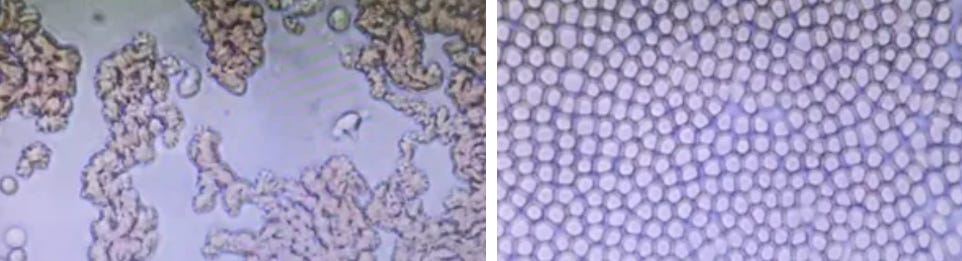
Check out the dis-aggregation of red blood cells after being exposed to chlorine dioxide for 12 minutes as per this experiment using photomicrographs:
ANTI-INFLAMMATORY MECHANISMS
From this masterful review article in the University of Guadelajara journal on mechanisms of chlorine dioxide, they report even more broadly systemic therapeutic mechanisms:
low concentrations of ClO2 can protect erythrocytes (red blood cells) from oxidative stress while inhibiting myeloperoxidase (MPO)-mediated excessive hypochlorous acid (HClO) production, thus reversing inflammatory responses and macrophage activation.
increases the expression of heme-oxygenase (HO-1), protects cells from death caused by hydrogen peroxide (H2O2), enhances the expression and activities of antioxidant enzymes, such as superoxide dismutase, catalase and glutathione peroxidase, and contributes to the resolution of the inflammatory process.
It promotes apoptosis (programmed cell death) in neutrophils, which helps resolve inflammation effectively
It has demonstrated anti-inflammatory responses by inhibiting macrophage activation in humans, thus reducing inflammation
Here it is important to review the different types and functions of macrophages (our immune system’s first line of defense against toxins and pathogens):
Monocytes are bone marrow derived precursors of tissue macrophages that are critical effectors of wound healing, clearance of bacteria and cellular debris and induction and resolution of inflammation. Macrophages that are associated with classical inflammation are termed M1 and those cells produce factors such as TNF-α, IL-1 and other proinflammatory factors. Macrophages that are associated with reversal of inflammation and suppression of immune responses are termed M2. In the context of ALS pathogenesis, the M2 macrophage phenotype within the spinal cord is associated with normal function, whereas the appearance of new M1 type macrophages within the spinal cord is associated with disease progression.
These data suggest that systemic macrophage associated inflammation may play a significant role in ALS disease progression.“ In this study of a chlorine dioxide precursor in ALS, they report “these mechanisms of downregulation transform inflammatory monocytes/macrophages from a proinflammatory to a basal phagocytic (wound healing) state.”
TAURINE-CHLORAMINE PATHWAY
Taurine-chloramine is a product of activated neutrophils and represents the most relevant functional product formed under the influence of chlorine dioxide. This molecule activates nuclear factor erythroid 2 (Nrf2), (this transcription factor regulates the inducible expression of numerous genes for detoxifying and antioxidant enzymes), and inhibits production of pro-inflammatory cytokines.
In a study of a different precursor, they report, “Of importance, a single dose of NP001 (a patented formulation of chlorite) caused a dose-dependent reduction in downregulation of CD16-expressing inflammatory macrophages in blood.”
In this study, they found that the above WF10 (another patented formulation) exerts potent immune-modulatory effects through generating endogenous oxidative compounds such as taurine chloramine. Proliferation and IL-2 production of anti-CD3 stimulated PBMC were inhibited by WF10, as was the nuclear translocation of the transcription factor NFATc.
In another study of the NP001 proprietary formulation of pH stabilized, purified chlorite, they found that in the presence of heme-associated iron, presumably from the nicotinamide adenine dinucleotide phosphate (NADPH) oxidase complex on the surface of phagocytic cells, it is converted from a prodrug through a hypochlorite intermediate, to an intracellular form of taurine chloramine (TauCl). TauCl is a long-lived effector molecule within macrophages that down-regulates NF-kB expression and inhibits production of pro-inflammatory cytokines in part through activation of heme oxygenase-1 (HO-1). A phase 1 controlled trial of NP001 in patients with ALS demonstrated the safety, tolerability, and dose dependent down-regulation of monocyte activation.
IMPACTS ON THE ZETA POTENTIAL
Increase of Zeta Potential in RBCs (red blood cells)
Effect of CDS on RBCs: The administration of CDS increases the overall charge of the surrounding environment, leading to an enhanced Zeta potential in RBCs. This increase in charge is primarily due to the oxidizing properties of chlorine dioxide, which interacts with the cellular membranes and modifies their electrical characteristics.
Enhanced Cell Repulsion: When the Zeta potential of RBCs is increased, it enhances the repulsive forces between individual cells. This prevents aggregation or clumping (a condition known as rouleaux formation), promoting better flow and circulation within the bloodstream. Improved circulation ensures that more oxygen and nutrients are delivered to tissues and organs.
Improved Cellular Function: The increased Z potential also contributes to healthier RBC membranes, facilitating better nutrient transport and waste removal. This overall improvement in cellular function can enhance the oxygen-carrying capacity of the blood.
Pathogen Elimination: One of the key benefits of CDS lies in its ability to eliminate pathogens. The oxidizing properties of chlorine dioxide enable it to target and disrupt the cell membranes of bacteria, viruses, and other harmful microorganisms. This mechanism effectively neutralizes pathogens without causing substantial harm to healthy tissues, differentiating it from traditional pharmaceuticals that may indiscriminately affect both pathogens and host cells. Human cells work at around 1000-1500mV ORP while pathogens are not able to withstand 100mV due to being a size-selective oxidant (Zoltran et. al )
Note: Many dosing regimens are reported. The minimum effective dose is unknown; even small amounts of CD can improve health. Benefits have been reported with only a few doses a week.
ANTI-CANCER MECHANISMS
Chlorine dioxide has been shown to have in-vitro anti-cancer cell effects, stimulates an in-vivo anti-cancer cell immune response and is also effective when injected intra-tumorally, or via a combination of oral, enema, and IV administration.
I have read a draft of a paper on a number of other mechanisms against cancer cells, written by an advanced applied chemist colleague named Tom Henshaw. It is still in draft form and I hope to share it with you all soon when it is either completed or published.
If this post whet your appetite for learning more about chlorine dioxide and you appreciate the time and effort I put into researching and writing my posts, please consider a paid subscription.
Thanks for your expert review of the literature on chlorine dioxide and chlorite's mechanism of action Dr. Kory. I will be posting about a new chlorine dioxide product soon that will also contain sodium chlorite, but at a much different proportion to chlorine dioxide than the MMS1 that people have generally been using for the last 15 or so years. In my opinion it has many advantages over MMS1, CDH (my first product) and CDS for most uses. Once it's out I would love to hear your thoughts on it. Take care
Dr Kory thank you for all of your time, research, expertise. You have been instrumental since 2021 in turning my long covid around - Covid in 2020 with long covid and vaccine injured in 2021- formerly in healthcare so despite hesitation felt mandatory for my job- Tragic. (Happy news: aboutto go hike in the Grand Canyon!) You mentioned hyperbariac oxygen treatment in this post and curious what you or others think about an oxygen concentrator to replace hyperbariac chamber? (Hyperbariac just so expensive but I have found hyperbariac oxygen at 2 atmospheres really helpful not so much the softshell home version) Possibly answered my own question with that last comment. Keep up the amazing and much appreciated investigative work!