

The "Kory Scale" - A Proposed Metric To Judge The Safety And Efficacy of "Unproven" Therapies Like Chlorine Dioxide
On teaching rounds in my ICU career, I humorously tried to name obvious medical insights after myself in an attempt to create an eponym that would endure beyond my career. Here is my latest attempt.

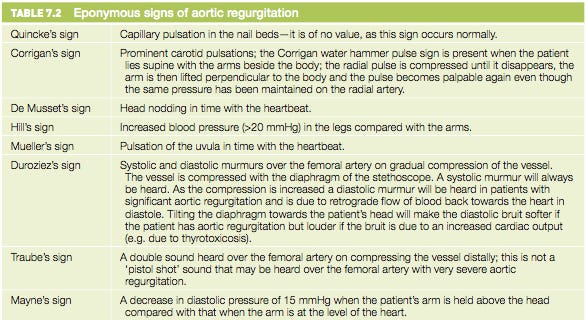
I thought I would have a little fun in todays post. From this paper titled “Medical Eponyms:”
Eponyms are a long-standing tradition in medicine. Eponyms usually involve honoring a prominent physician scientist who played a major role in the identification of the disease. Under the right circumstances, a disease becomes well known through the name of this individual. There are no rules on eponym development. It may take an extraordinary period of time, be different in different languages and cultures, and evolve as more is known about the physician or the disease.
Here are some eponym examples (there are thousands):
As my subscribers know, I have for months now been researching and writing about the science and promise of chlorine dioxide therapy in the treatment of not only infectious diseases but a broad set of others. I am currently juggling about 5 draft posts on the histories of various “pioneers” of not only chlorine dioxide therapy, but earlier, nearly identical orally ingested oxidative therapies from the early 20th century.
Know this history starts with Nikola Tesla’s work on ozone therapy which led to the later collaboration with and contributions by doctors like Dr. Eugene FM Blass and Dr. William F. Koch, both of whom developed oral and/or injected oxidative therapies whose efficacy and mechanisms seem to match that of chlorine dioxide.
I have not published those histories yet because critical information (some of which is likely classified) continues to be imparted to me on a daily basis. However, what has already been revealed is a disturbing pattern of attacks and persecutions on the pioneering researchers and practitioners of oral ingested oxidative therapies. To not miss these critical upcoming posts, I suggest you subscribe:
I am also in the midst of writing a book which I will unsurprisingly call, “The War On Chlorine Dioxide” (draft subtitle: “The medicine that would end Medicine”). OK, a bit overstated but whatever, should pique interest in the topic.
Anyway, the pattern of persecutory behaviors that I am uncovering, based on my research into other erroneously discredited and/or suppressed but highly effective treatments like DMSO, IV Vitamin C, ivermectin, hydroxychloroquine, proxalutamide, strongly suggest that oxidative therapy practitioners were identifying an effective, inexpensive, and safe treatment for a broad set of diseases.
Obviously it goes without saying that the reason I assert this, is that simple, cheap, safe, and broadly applicable treatments for human disease is anathema to the immensely powerful bio-pharmaceutical industrial complex. This is particularly true in the United States (which in the wake of my Covid journey, I now not-so-affectionately call “The United States of Pharma.”)
“The Kory Scale” Proposal
The conceptual underpinning of the Kory Scale is that scores should be directly proportional to the degree, breadth, and viciousness of the attacks generated from “the medical establishment” in response to reports of efficacy of the proposed therapy (i.e. attacks from the AMA, FDA, NIH, DOJ, medical journals, pharma-controlled media, and the military).
History Of Trying To Name Medical Terms After Myself
First, to not come across as an egomaniac, I want to give some fun background as to why I am narcissistically trying to name this scale after me. First off, I thought of it first (I think?). But more importantly, my former trainees (fellows, residents, and students) will recall that I would entertain them on teaching rounds by humorously trying to coin an eponym named after me, typically based on a “silly” and patently obvious finding that I would teach them.
One example was when I would teach my trainees something I tried to coin “The Kory Sign,” which was a sign that I claimed would predict the success of a patients ability to be liberated from a mechanical ventilator with 100% specificity.
Know that taking patients off ventilators is a core skill of an intensivist and one that I taught on a daily basis for almost two decades. Liberating a patient from a mechanical ventilator at the right time is absolutely critical to their recovery and survival because immense amounts of data have shown that for every extra day a patient spends in an ICU or on a ventilator, outcomes and survival rates worsen.
So, a good intensivist has to be able to take a patient off a vent “not too early” and “not too late.” “Too early” led to emergency re-intubation and its complications, i.e hypoxia, paralysis, sedatives and now an even longer course on a vent because they “tired out.” Taking a patient off “too late” led to higher incidences of sedative induced encephalopathy (ICU delirium), muscle disuse atrophy, infections, stress ulcer bleeds etc..
So, what was this “Kory Sign” that predicted success of liberation with such incredible accuracy? Basically, it was when I walked into the room of an ICU patient and found a fully awake patient who was able to focus and connect with my own gaze (i.e. their sedatives had completely worn off) and who, despite not being able to talk due to the endotracheal tube still down their windpipe, would be gripping the handrails of the bed and pointing to the tube using facial and finger gestures which tried to communicate something like, “Hey Doc, can you take this fucking tube out?” Know that I have never seen someone need re-intubation after displaying “the Kory sign.” A little ICU humor, sorry.
I also tried to invent a different, somewhat sillier “Kory sign” which indicated readiness for a patient to be transferred out of the ICU, i.e. meaning the patient no longer met criteria for the intensive monitoring required in critical illness or organ failure. Know that ICU beds suffer from the stresses of short supply and great demand, thus decisions to admit and discharge were critical to both hospital and community functioning.
This sign, when displayed, meant that the patient was stable enough for the lower monitoring capabilities of a regular hospital ward. So, what was that sign? That was whenever I walked into the ICU room of a patient on morning rounds and they would be lying in bed with their legs crossed at the ankles. When I saw that, I would say - “Kory sign”! “Transfer to regular hospital ward”!
The reason that sign was so instructive is that truly critically ill patients never have their legs crossed in bed. Only calm, mentally organized, and physiologically stable patients lay back like that. Note that an earlier version of “the Kory sign” was when I walked into the ICU room and found patient holding up and reading a fully opened newspaper (as long as the paper was right side up that is).
Understand that these self-eponym proposals were not ego exercises but instead were attempts at keeping my trainees engaged and stimulated (and laughing) given that ICU rounds on average took between three and five hours (which is torture to the residents and fellows who had worked through the previous night).
Now lets further discuss this third, more serious Kory eponym proposal since the last two “never took off,” (at least I don’t think they did but I wouldn’t know because I don’t practice or teach ICU medicine any longer).
The Kory Scale
Again, as above, the conceptual underpinning of the Kory Scale is that scores should be directly proportional to the degree, breadth, and viciousness of the attacks generated from “the medical establishment” in response to claims of efficacy of the proposed therapy (i.e. attacks by the AMA, FDA, NIH, DOJ, medical journals, pharma-controlled media, and the military).
I propose that the higher the score, the more effective, safe, affordable and broadly applicable to the treatment of human diseases an “unproven” therapy will be.
At the risk of stating the obvious, one reason why I assert that there is a strong relationship between the amount of persecutions by authorities and the degree of efficacy that a treatment holds, is that obviously ineffective or dangerous therapies do not generally need to be persecuted in such a broad and coordinated manner. In such cases, they either “never take off” (i.e become popular with a rapidly broadening wave of physician and patient support), or they “die off on their own” (i..e fall out of use organically because they aren’t clinically impactful), or they can be eliminated by those same authorities with only one or two “restrictive” actions.
Well, that is, unless the ineffective and/or harmful therapy is popularized and promoted by the pharmaceutical industry (like mRNA vaccines, Paxlovid, Remdesivir, Molnupiravir etc). There, the inverse of the Kory Scale needs to be applied, i.e. you need to assign scores to what befell the “critics” (not the advocates) of those therapies. This will conversely allow you to estimate the inefficacy or harms that Pharma is trying to suppress.
Before I go further, I have to admit that this new term is similar to an already existing medical eponym called “The Simmelweiss Reflex.” Per Brave browser AI:
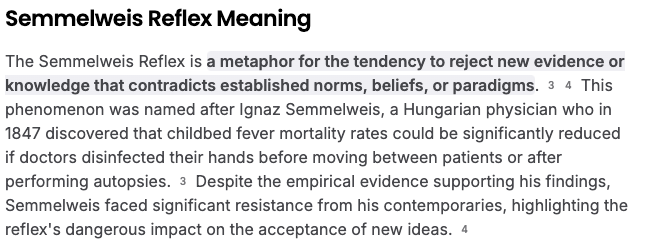
Fun fact: Semmelweis was Hungarian… and so am I (my father is from Hungary).
I do think there is a distinction between the “Simmelweiss Reflex” and the proposed “Kory Scale,” in that the former describes a situation where the medical pioneer endures persecution and ridicule before their discoveries later become proven and gain widespread recognition.
The “Kory Scale” is simply a real-time tool used to judge the “likely” efficacy, safety, and applicability of any as yet “un-proven therapy” (loaded term) in the treatment of human disease. Most therapies that score high on the Kory scale will NEVER get proven or widely adopted due to their common traits of either;
not having the potential to produce obscene profits (too inexpensive to make or are already widely available)
having the potential to liberate people from chronic illness thus eliminating decades of pharmaceutical product sales
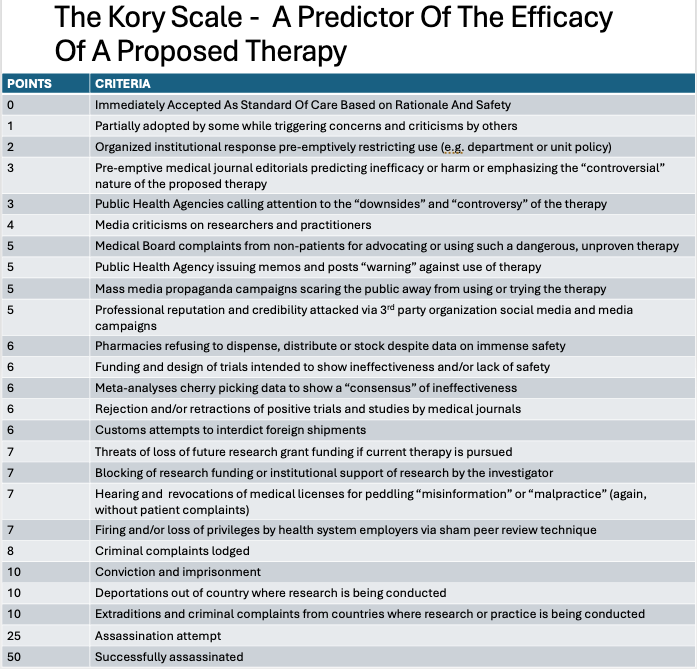
The “Kory Scale”
Here is a first, very rough, draft of the Kory Scale (I invite my subscribers to suggest revisions, edits, additions, especially with the arbitrary and inconsistent points assigned the various persecutory actions).
Know that in Covid, many (but not all) of the above actions were taken against researchers and advocates for hydroxychloroquine, ivermectin, proxalutamide, chlorine dioxide as well as for those against mRNA “vaccines,” Remdesvir, Paxlovid, Molnupiravir etc.
My thinking right now is that you total up the score for each action to obtain an overall score. The higher the total score, the more likely the therapy is “threateningly effective.” As you can see above, I assigned more points based on the viciousness and/or malevolence of the actions taken. Obviously the scores are completely invented and unvalidated and likely inappropriate (e.g. what score should I assign for a therapy whose leading practitioner and/or advocate was assassinated? A 100? A 1000?)
Calculating The Kory Scale For Ivermectin And Chlorine Dioxide
Lets first try to estimate the efficacy of ivermectin in Covid using “the Kory Scale.” Obviously, this is just a thought exercise and not meant to (or could ever be) comprehensive. Recall that after my “ivermectin testimony” in the U.S Senate went viral:
Within 2 days the Associated Press published a hit piece against me, the FLCCC and ivermectin (4 points),
Within 6 weeks, my review paper was mysteriously retracted despite having passed three rounds of rigorous peer review (6 points)
Within 3 months, the WHO recommended against using it outside clinical trials (despite finding in their analysis that it reduced mortality by 82% and willfully excluding the wickedly positive prevention trials (6 points)
The FDA posted weird negative “memos” conflating the dangers of animal products with human ivermectin (3 points)
Large ”rigorous” trials were conducted and manipulated to conclude ivermectin was ineffective in Covid (6 points x 7 trials = 42 points)
Retail pharmacies around the country refuse to fill valid prescriptions of one of the safest medicines in history (6 points)
A highly positive ivermectin trial was accused of being fraudulent, creating a narrative that “all positive trials of ivermectin were fraudulent” (6? points)
Pressures put on the lead ivermectin researcher for the WHO to self-retract his own highly positive meta-analysis based on 24 RCTs (6 points)
A massive global, highly coordinated PR campaign was deployed to convince all that ivermectin was a “horse dewormer,” triggered by a coordinated series of actions by the FDA (tweet), CDC (memo), and NIH (Fauci on CNN). (15 points - 5 each)
I received 11 complaints to my medical licensing board about being a misinformationist (5 points)
I was fired from my independent ICU contractor job due to outside pressure being placed on my employer (conjecture) 7 points
Same happened to my FLCC colleagues: Dr. Meduri was forced to retire from the VA (7 points), Dr. Marik was denied privileges based on fabricated accusations (a hospital technique called a “sham peer review” - 7 points) and Joe Varon had his hospital investigated and shut down (unrelated or not, timing was suspicious - 7 points)
Intermittent negative hit jobs on me, Paul Marik and the FLCCC were published, timed with the publication of the manipulated trials (5 points)
The American Board of Internal Medicine publicly went after me for violating a brand new “misinformation policy” they invented which ended with their revocations of all three of my specialty Board certifications (7 points)
To be honest, I could go on and on, especially if I include points for what happened to all of my colleagues around the country and world - endless hearings, suspensions, revocations and firings (but no assassinations). Total Kory Scale Score Range for ivermectin is approximately 100 - 150 :).
The Kory Scale For Chlorine Dioxide
So, with our validated (yeah right) new metric, and at the risk of foreshadowing (since I have not published the full histories of the chlorine dioxide pioneers yet), let’s calculate the Kory scale score for chlorine dioxide and/or other highly similar oral “oxidative” therapies which preceded chlorine dioxide.
Again, I will provide the references and sources for all the below claims in upcoming posts.
William F. Koch - Research shut down (7 points), harassed by the FDA and numerous professional societies (5 points), smear campaigns appeared in the press and medical journals (5 points and 5 points). Ultimately he was assassinated by poisoning the same year as Blass (next). 50 points. His wikipedia page claims he was a charlatan (5 points)
Dr. Eugene FM Blass - murdered by assailants outside his lab (purportedly the KGB), work stolen and handed over to the Russian bioweapons program (50 points)
Anonymous confidential informant scientist - informally deported from three countries (Nigeria and Uganda and the UK), received numerous threats to his life and career, partners were jailed in the UK (50+ points).
Jim Humble - informally deported from Guyana, ridiculed by the world’s media for years, also received threats (25 points)
Mark Grenon - survived two assassination attempts, he and his family were extradited and imprisoned in early Covid on false charges by the DOJ on the bidding of the FDA (150 points)
Unnamed missionary colleague of Grenons in Africa who was treating malaria - legs blown off by an incendiary device planted in his hotel (25 points)
Howard Alliger - forced to leave company for unclear reasons, daughter company later moved away from chlorine dioxide research (5 points - this score is low because Alliger never studied orally ingested chlorine dioxide, focusing instead on topical and mucosal applications many of which have reached the market).
Vladimir Pasechnik - bioweapons researcher and chlorine dioxide expert was murdered in 2001 likely by the KGB after becoming an international whistleblower on the Russian Bioweapons program (100 points)
David Kelly - another bioweapons expert who was murdered (“suicided”) months after the start of the US’s invasion of Iraq (100 points).
In 2019, Amazon.com removes all books on MMS by Jim Humble and Kerri Rivera, Facebook deletes all pages and chat groups focused on chlorine dioxide and Youtube scrubs videos on chlorine dioxide with millions of views (20 points)
Dr. Patricia Callisperis - a Bolivian surgeon friend and colleague who is a chlorine dioxide expert. She received anonymous phone calls meant to intimidate her to stop researching and talking about chlorine dioxide during Covid (5 points)
Enno Frye - adjunct professor and researcher who conducted and published a highly positive study of 500 malaria patients treated with chlorine dioxide in Cameroon. After he obtained funding from the UN for another trial in Senegal, narcotics were planted on his person and he was falsely imprisoned in Italy for three years. His paper was later retracted and the media and journal and his University claimed the trial never took place (30 points)
Dr. Mitch Liester, Psychiatrist at the University of Colorado and an expert in chlorine dioxide. He knew it would be effective against Covid and so he submitted a study proposal to CU’s Institutional Review Board in 2020, including immense amounts of data regarding the safety of ingestion of chlorine dioxide at the proposed treatment doses. He was quickly rejected based on the FDA’s position that it was toxic.
Dr. Pierre Kory - happily researching and writing Substack posts for free to his subscribers, letting them know of the potential of chlorine dioxide while trying to promote the conduct of more research into the compound (0 points for this activity so far which is why it is a good time to remind all that I am happy, inspired, and not suicidal).
Kory Scale Score For Ivermectin - 100-150 points
Kory Scale Score for Chlorine Dioxide - over 500 points
If you appreciate the time and effort (and the personal and professional risks I am taking) in researching and writing on chlorine dioxide, support in the form of paid subscriptions is appreciated.
P.S I want to again emphasize that I am not recommending treatment with chlorine dioxide via oral ingestion to anyone as these posts are simply intended to help open and guide research into the treatment of human diseases with this promising compound.
P.P.S As a last exercise, if you are still engaged on this topic, I propose you watch this documentary of Dr. Stanislaw Burzynski and his anti-neoplaston therapy for cancer. Let me know what score you would assign the efficacy of his therapy according to the “Kory Scale”

Something that may interest you Dr. Kory:
The Film Rain Man Was Likely Forged to Pre-Program the Populace For the Upcoming Explosion in Vaccine Induced Autism.
1986: Congress Grants Immunity Shield to Vaccine Makers for Venom Injection Damage | Film Rain Man Begins Production
1988: Rain Man Released to Educate, Condition, & Normalize Autism
1986—2025: Number of vaccines administered explodes to 78 - and rising - from birth to two years of age. Autism diagnoses explode right along with them.
Before the film few even knew what the term meant because it was so rare it was seldom reported, much more on this here: https://tritorch.substack.com/p/autism-pre-conditioning-and-normalization
I love Dr. Burzinski! This was a great film and I have followed his trials since the 1980’s when I was an ICU nurse dealing with patients with AIDS in SF. I knew Fauci was a fraud back then- should have been tried for murder back then. And here we are… Just referred a patient to Dr. B last month. Thank you for citing him. Hope you talk about Dr. Willner, too…