

The Criminal Censorship of Ivermectin's Efficacy By The High-Impact Medical Journals - Part 1
High-Impact medical journal editorial staff were getting orders to censor ivermectin studies from Big Pharma and "philanthropaths" like Bill Gates.

Dr. Marcia Angell, a former long-time editor in Chief of the New England Journal of Medicine (NEJM) resigned in June of 2000 after twenty years in the post. She resigned because of what she described as the rising and indefensible influence being exerted by Pharma at the prestigious journal and its powerful affiliate societies. So she wrote a book about it instead. Some really important quotes of hers from “The Truth About Drug Companies: How They Deceive Us and What to Do About It” are:
“Now primarily a marketing machine to sell drugs of dubious benefit, big Pharma uses its wealth and power to co-opt every institution that might stand in its way, including the US Congress, the FDA, academic medical centers and the medical profession itself.”
The above is exactly why I call our country the United States of Pharma. Notice she mentions the FDA (although the NIH’s complicity is implied by the rest of the sentence). I have been saying since early in the pandemic that the United States Federal Health Agencies are (and have long been) in a state of “total regulatory capture.” Definition of regulatory capture from Wikipedia:
Regulatory capture is a form of corruption of authority that occurs when a policymaker or regulator is co-opted to serve the commercial interests of an industry.
Here are two more quotes from Dr. Angell:
“It is simply no longer possible to believe much of the clinical research that is published, or to rely on the judgment of trusted physicians or authoritative medical guidelines. I take no pleasure in this conclusion, which I reached slowly and reluctantly over my two decades as an editor of the New England Journal of Medicine.”
This one is nuts:
“In 2003, the profits of the top 10 big Pharma exceeded that of the cumulative profits of the other 490 Fortune 500 Companies.”
Whoa.
Dr. Relman, another former editor-in-chief of the NEJM said this, also 20 years ago:
“The medical profession is being bought by the pharmaceutical industry, not only in terms of the practice of medicine, but also in terms of teaching and research. The academic institutions of this country are allowing themselves to be the paid agents of the pharmaceutical industry. I think it’s disgraceful.”
Richard Horton, editor in chief of The Lancet said this in 2015:
“The case against science is straightforward: much of the scientific literature, perhaps half, may simply be untrue.”
As Dr. Aseem Malhotra (one of the most prominent physician COVID truth tellers that has remained employed) recently tweeted a quote from an interview he did:
“We have a wealth of evidence of the fraud that’s been committed by the pharmaceutical industry over the years’ ‘the real scandal is that doctors & medical journals collude with industry for financial gain & the regulator fails to prevent misconduct by industry.”
I want to clarify the point above about “not being able to trust half the science in medical journals.”I want to be clear that he is referring, in my mind, largely if not solely to what I call the “high-impact medical journals” and not all science journals. You should know that each journal is ranked by what is called an “impact factor” defined by Wikipedia as:
A scientometric index calculated by Clarivate that reflects the yearly mean number of citations of articles published in the last two years in a given journal. As a journal-level metric, it is frequently used as a proxy for the relative importance of a journal within its field; journals with higher impact factor values are given the status of being more important, or carry more prestige in their respective fields, than those with lower values. While frequently used by universities and funding bodies to decide on promotion and research proposals, it has come under attack for distorting good scientific practices
Lets look at the top 5 in the world today:
With the exception of the Annals of Internal Medicine, all the journals on the above list will feature heavily in this and my next post detailing their criminal collusion throughout the pandemic. One journal not on the list above but that should be included is the Cochrane Library. Not because of their impact factor but because they are considered the premier journal publishing the highest form of medical evidence called a “systematic review and meta-analysis of clinical trials (SRMA).” I will argue below that, beyond the corruption of the ivermectin evidence by the WHO detailed in my two previous posts here and here, it the Cochrane library’s rejection of Andy Bryant and Tess Lawrie’s SRMA followed by their publication of a fraudulent SRMA that can be blamed for the most deaths.
One of the most important powers of these journals is that they can drive headlines like nobody’s business. When a Pharma friendly study gets published in one of those journals, it launches a PR media campaign that no amount of commercials or advertisements could accomplish. Conversely, if Pharma wants to prevent an effective generic drug or vitamin from being adopted widely, they pay researchers to design, conduct, and publish fraudulent studies in these journals. When such a study is published, it triggers an equally effective “negative” PR campaign warning the world and its doctors against using such “dangerous” and “ineffective” therapies.
Big Pharma and BMGF (he gives money to a lot of medical journals) essentially control the high-impact journals. They figured out the importance of doing that many decades ago as numerous former editors have reported above. By doing that, Pharma can get the world to use ridiculous therapies like Remdesivir, Paxlovid and coronavirus vaccines while ignoring and recommending against the use of Vitamin D, hydroxychloroquine, and ivermectin.
This post will detail the numerous, indefensible, and highly irregular rejections from publication of well-designed, positive trials of ivermectin. My next post will detail their use of a novel tactic whereby they got lesser impact journals that published positive studies of ivermectin to retract those studies.
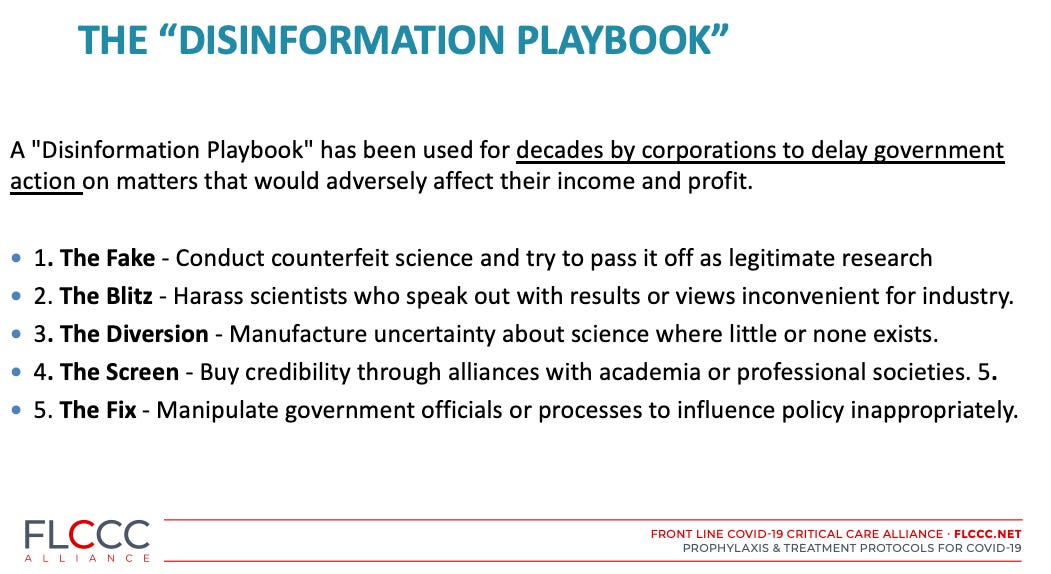
Now, what I find interesting is that in the “Disinformation Playbook” article by the Union for Concerned Scientists in 2017, they described 5 main Disinformation tactics used by Pharma to attack emerging science that is “inconvenient to their interests.” The tactics were named using famous American Football plays as below:
These “journal censoring” tactics must be added to the Disinformation Playbook. I propose we name it “The Zone,” defined in American football as a defensive play where “a player is able to observe what the quarterback (truth teller) is attempting to do, anticipate where a pass may be thrown, and perhaps intercept the pass. Zone defenses tend to produce interceptions of passes or outstanding collisions with receivers (welcome to my life) after they have made pass receptions.” Nailed it.
I would argue the “Zone” of censorship operated across three main types of information disseminators; legacy media (radio, print, television), social media (Twitter, Instagram, Linked in, etc), and the medical journals.
The reason why I remind you of the three main categories of information dissemination is because I maintain that all, and I mean all, of the media propaganda (later post) and media censorship of ivermectin was made possible solely by the actions of these high-impact medical journals. Dr. Flavio Cadegiani, my FLCCC colleague and friend, this calls them the “Editorial Mafia.”
Further, by the Editorial Mafia dictating what scientific studies, fraudulent meta-analyses, and negative editorials were published, this then allowed national and international health agencies to issue corrupted recommendations against the use of ivermectin. These recommendations then led to the majority of the worlds’ doctors to refrain from using or even trying ivermectin.
The high-impact journal editors did four things to suppress the evidence of efficacy of ivermectin in COVID:
1) Rejected all positive trials of ivermectin, even (and especially) the high quality ones, starting as far back as May of 2020. (that is what this post is about).
2) Retracted positive ivermectin studies even after they passed peer-review and/or were already published (these actions were unprecedented in our careers as physicians and researchers). That is what my next post will be about.
3) Published fraudulent trials and fraudulent meta-analyses, with the latter technique identical to that employed in the WHO’s corrupt recommendation against ivermectin here. This is a known Disinformation tactic called “the Fake,” defined as “conduct counterfeit science and try to pass it off as legitimate research.”
4) Published numerous anti-ivermectin editorials, which is also an already named Disinformation tactic called “The Diversion.”
The rejections and retractions were the most damaging because any positive trial of HCQ or IVM published in a high-impact medical journal would have changed the entire trajectory of the pandemic. That is because the high-impact journals have the power to “move the needle” in terms of not only creating major media headlines but also in guiding health care policies by national and international health care agencies.
Recall how corticosteroids (my first Senate testimony in May 2020) later became the standard of care in COVID hospital patients overnight, immediately after the UK RECOVERY trial results from Oxford were reported in June of 2020. I can still fondly recall all of my former trainees and colleagues texting me the next day to say “we should have listened to Pierre” in regards to my testimony 6 weeks earlier. But that was before ivermectin. With rare exception, none have reached out to me in many months though. The silence started after ivermectin but became deafening when I (and later the FLCCC) came out against the vaccines.
Know that high-impact journal censorship of “inconvenient science” began very, very early in the Pandemic. In this definitive documentary that first proved the lab-made origin of the virus, world renowned scientists went on the record stating that their papers showing that the virus was man-made were getting rejected quickly from journals they had long published in. That was the “Editorial Mafia’s” first crime.
Then came the Surgisphere fraud published in the Lancet which drew the first blood against HCQ. Then David Boulware published his inept trial of HCQ prophylaxis and when we asked questions about his conduct of the trial and presentation of the data, he started misrepresenting to us about what exactly happened. My brilliant colleague David Wiseman went after him in this pre-print paper which I co-authored (but David did most of the work). For my subscribers, recall that Dr. Boulware was a central figure in the corruptive influence of the TOGETHER Ivermectin Trial given his indefensibly inaccurate and damaging quotes to New York Times reporters. He too has blood on his hands.
Our dear colleague Dr. Norman Fenton and his team performed an analysis of England mortality data and found that the UK government was mis-categorizing vaccination status so badly that it hid the evidence of its inefficacy and toxicity. It still sits on a pre-print server.
Similarly, experts from prestigious Universities analyzed U.S and European databases and found increased all cause mortality among the vaccinated, particularly among children. Their paper still sits on a pre-print server.
Jessica Rose and Peter McCulloughs paper on myocarditis rates after the COVID vaccines was withdrawn by the publisher after publication because they didn’t like the conclusion. There is still nobody speaking out against Elsevier for unethically censoring science. Not one person from the pro-vax side thinks censoring science is wrong. It’s stunning because it is so objectively unethical. Nobody can defend this so everyone is instead silent about it.
And it is getting worse. The other day a paper was posted that found for every hospitalization supposedly prevented by COVID jabs, up to 98 serious adverse events would be suffered by young people between the ages of 18-29. Chances of getting published? Zero. Publishing “Pharma-inconvenient science” is nearly impossible nowadays.
Now, had the high-impact journals published even one positive trial for IVM or HCQ, millions of lives could have been saved. But that is not what happened. Those journals specifically blocked from publication any paper with “statistically significant” results supporting the use of IVM or HCQ. Never forget this. Ever. It is these Editorial Mafia actions which fueled the twin mass killings by COVID and the vaccines.
Millions died due to the fact that no early treatments or preventatives were recommended across all the advanced health economies. Contrast how those economies fared compared to all the low and middle-income countries where IVM or HCQ are commonly used in prophylaxis programs for malaria and/or parasites and were thus widely used. It’s not even close.
Beyond the fact that IVM or HCQ would have blown up the markets for Pharma’s pipeline drugs like Paxlovid and Molnupiravir, recognize they also threatened the many billions going into the vaccines.
I maintain that the editors of the high-impact journals had standing orders to not publish positive data on repurposed drugs. So the editorial mafia rejected and retracted positive studies while publishing fraudulent studies and editorials. Lets start with the rejections.
REJECTIONS OF POSITIVE IVERMECTIN STUDIES BY HIGH-IMPACT MEDICAL JOURNALS
1. The rejection of Tess Lawrie et al’s “Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines” by the Cochrane Library is to me the single most damaging action taken against ivermectin. Recognize that the Cochrane library was for decades considered the gold standard amongst academia for SRMA’s. Note that I said “was the gold standard.”
Because, you guessed it, they got captured by Pharma and Gates. In 2018, mass resignations of Cochrane Library Board members occurred due to what one said was a “growing top-down authoritarian culture and an increasingly commercial business model” that “threatens the scientific, moral and social objectives of the organization.” I am sure the fact that Gates becoming a donor two years earlier had nothing to do with it. Yeah right. Further, Gates’s money supports many if not all of the journals in the list above and below. Shocker I know.
As per Tess, immediately upon seeing my ivermectin testimony, she became intrigued and immediately started her own expert review of the RCT evidence I presented in Senator Ron Johnson’s landmark Senate hearings. Tess knew that speed was of the essence to save lives. Note that Tess and her team are world experts in this type of work - between Tess and her colleagues Andy Bryant, and Therese Dowsell, they have published approximately 120 Cochrane Reviews. All she had to do was get Cochrane to accept her proposal and publish her review. Had she succeeded, this would have neutered the ability of Andy Hill, Andrew Owen, and the WHO to issue their corrupt recommendation against ivermectin as I detailed in previous posts here and here.
Understand that if there is a medicine that has a Cochrane Library review supporting its use in a disease, it becomes established as the standard of care. Out of the entire worlds’ scientists, Tess knew that a systematic review and meta-analysis of the evidence supporting ivermectin published by the Cochrane Library would result in all global health agencies recommending its use and would immediately have saved hundreds of thousands of lives. So, Tess proposed to Cochrane for her team to do a “Rapid Review of Ivermectin.” They initially accepted her proposed study protocol! She had a green light.
But not for long. They changed tune fast, likely due to pressure from Gates or one of their Big Pharma funders. My money is on Pfizer.
What happened next is that all of a sudden, the Cochrane editors informed Tess that a “Rapid Review” was inappropriate and that a “Full Review” protocol should be followed. She quickly agreed to do so and submitted a Full Review protocol as her team, in anticipation, had actually already completed the work.
Pressure was on. The corrupted Cochrane Library was in a bind. Unsurprisingly, they then started accusing her of “conflicts of interest” because of her video plea to Boris Johnson that she had posted on YouTube in early January of 2020 (which was essentially her telling Johnson the results of the review she had completed so that he could immediately consider implementing a policy for use in the UK). Note her doing so in no way presents “a conflict of interest.” Tess does not make money from ivermectin. In fact, an expert of her level is morally and professionally obligated to share such findings to the public, especially during a global pandemic mired in that wicked winter surge of 2020-2021.
She reminded the Cochrane editors of that in a brilliant email referencing established principles of researchers. Yet, to preserve the opportunity to publish such critical data in the vaunted Cochrane library, she offerred to step down as an author if they continued to have concerns of her “conflict of interest."
Her defense to Cochrane editors fell on deaf (or dumbed) ears. They simply told her to go publish in another journal and instead assigned the Full Review work to a German team led by Popp et al. I don’t know Popp but don’t have to. Popp proceeded to employ the identical tactics that the WHO research team did, a brazenly manipulated review which came to a very different conclusion than Tess’s team, i.e. instead, after dismissing most of the evidence base, they concluded that the evidence for ivermectin was of “very low certainty” and thus insufficient to support a recommendation.
Tess’s team masterfully tore apart the fraudulent Cochrane review here. It’s a must read for science and stat geeks. Note it remains on a pre-print server. Yup. Also, their critique should be updated to incorporate the Cochrane review teams latest fraudulent action, that of including the TOGETHER trial in their review despite the fact it did not meet their protocols inclusion criteria as uncovered recently by the brilliantly detailed Alexandros Marinos here. To get a sense of how brazenly corrupt the Cochrane review authors acted (with the approval of the journal mind you), read Alex’s title and sub title of his post;
The Cochrane Review on Ivermectin Violated Its Own Inclusion Criteria for 76% of the Patients It Included
5 of the 11 included studies, covering 2582 of the 3409 patients included in the systematic review did not qualify for inclusion, based on a novel criterion used to exclude many other studies.
“Gold standard” eh? Whatever. Clown world.
Let’s get back to Tess and her team. The below is from a colleague of Tess’s named Edmund Fordham whose email to me puts the Cochrane library’s actions in a powerful context. Read on:
Cochrane works in a different way from other journals. The critical thing is the acceptance of the review “protocol.” They do peer review the final result, but mainly for conformity with the protocol. So long as the protocol is observed, then you are essentially guaranteed publication. It’s not like a journal receiving manuscripts speculatively. The reviews are prepared in Cochrane’s RevMan software, then the final version is converted to a PDF in software controlled by Cochrane (so you can’t impersonate the imprint). But the text is very formulaic and authors have very little latitude; the sections must follow a prescribed set of headings.
So the real panic at Cochrane was they had to find a way to reject our protocol. Since they had in fact accepted it, before Tess’ famous Zoom with Hill, their only option was to say the topic was unsuitable for the Rapid Review format - which they did. They wanted a Full Review instead. So we sent the Full Review protocol (apart from constraints on format, the main difference is that data extraction must be done by two reviewers independently - which we had done already). So then they had to invent accusations of Conflicts of Interest against us which were not there; then they invited the German Government consortium to do the “Cochrane Review” to eliminate us - said consortium having previously made clear they only wanted the software infastructure and had no intention of registering their protocol as a Cochrane review. The 148 page “nothing burger” of Popp et al. was the result (I will list this under “the Fake” below -PK). They have recently updated the review including TOGETHER and I-TECH which were registered retrospectively - having previously said this was an exclusion criterion, as Alex Marinos’ latest post makes clear. So it’s transparently clear that Popp et al. are only interested in Pharma-sponsored medicines and happily conflate “regulatory approval” with “clinical efficacy.”
Cochrane was clearly under major pressure in January 2021 as soon as the bust-up between Tess and Andy Hill became known.
If you are one of those editors of Cochrane and are reading this, know that your actions led to the deaths of millions. Try to rationalize and defend yourself by saying you had no choice. Good luck with that. All you had to do was blow one whistle. But you didn’t.
Rejection #2.
Dr. Eli Schwartz is a world renowned Professor of Tropical Diseases at one of the top universities in Israel. His sophisticated double blind RCT effectively “proved” the anti-viral properties of ivermectin against SARS-CoV2 when he found that both viral cultures and PCR tests cleared faster in those treated with ivermectin. This is what he wrote to me after I asked him when his landmark paper would be published (many months ago):
Hi Pierre, the sequence of submissions were: NEJM, Lancet- eclinical medicine, and Clinical Infectious Disease. The rejections came within a few hours. At that time I did not submit it to medRvix (pre-print server) to avoid rejection based on "already published information." Now, we submitted it to Clinical Microbiology and Infection and in parallel to medRvix.
It would have been a world-changing study. To this day, one of the most important papers proving the anti-viral efficacy of ivermectin still sits on a pre-print server here.
Rejection #3
Retired Professor and now friend Hector Carvallo submitted a paper to JAMA showing massive impacts of an early treatment protocol he devised centered around the use of ivermectin, dexamethasone, aspirin, and enoxaparin, i.e. the IDEA protocol (all now validated as effective). See the initial response from the Editor-in -Chief below. What is important to note is that it did NOT get rejected immediately, which traditionally was a very good sign that the journal is interested in your study (rejections, when they occur, result in an almost immediate auto-reply letter).
Notice the date of the letter. Wow.
April 9, 2020
Dear Prof CARVALLO:
Thank you for submitting your manuscript, "IVERMECTIN AND CORTICOIDS:," received on April 9, 2020, to JAMA. Your manuscript has been assigned the following manuscript number: JAMA20-6173. Please refer to the manuscript number and corresponding author in all subsequent communications.
You may check the status of this manuscript by selecting the Check Manuscript Status link on the following Web page. You will be required to enter your password. If you are unable to locate your password please click the "Unknown/Forgotten password" link.
Please do not share this email with anyone.
https://manuscripts.jama.com/cgi-bin/main.plex?el=A1e5BPQJ7A1Dbya3F6A9ftdKuZXKqSIZZbenT5ReNmhzgZ
* We agree to consider your manuscript with the understanding that its content, figures, and tables have not been published or submitted elsewhere in print or electronic format and will not be submitted elsewhere during the period of review by JAMA.
* If you have not already done so, please provide copies of any manuscripts on closely related topics or with possibly duplicative material that have been previously published or are under consideration for publication elsewhere.
* The information in your manuscript should not be distributed or released in hard copy or electronic form, except through presentation at scientific meetings, unless and until the manuscript is published.
* The fact that your manuscript is under consideration by JAMA is confidential and should not be disclosed to anyone except coauthors and contributors.
Every effort will be made to expedite the review of your manuscript and to notify you of our decision as soon as possible. If you have questions or concerns, please contact the editorial office at jamams@jamanetwork.org or 312-464-4444. Our business hours are Monday through Friday, 7 AM to 5 PM Central Time.
Thank you for the opportunity to consider your work.
Sincerely yours,
Howard Bauchner, MD
Editor-in-Chief, JAMA
Email: Howard.Bauchner@jamanetwork.org
Phone: (312) 464-2400
Fax: (312) 464-5824
Despite this optimistic sign, within hours he receives the dreaded “auto-reply” rejection email below. Wow again.
April 9, 2020
Prof Hector Eduardo CARVALLO
A.A. Eurnekian Hospital
POST GRADUATE
L. N. Alem 349
Ezeiza, Buenos Aires 1804
Argentina
RE: IVERMECTIN AND CORTICOIDS:
Dear Prof CARVALLO:
Thank you for submitting your manuscript to JAMA. Each manuscript is thoroughly evaluated by the JAMA editorial staff, who assess the manuscript's quality and its priority for publication. Those manuscripts judged unlikely to succeed through stringent external review or whose subject matter does not meet our current editorial priorities are rejected at that point.
More than half of the approximately 7000 manuscripts submitted to us annually are rejected after such in-house review, and less than 9% of manuscripts are eventually accepted for publication in JAMA. Based on our evaluation, I regret to inform you that we will not pursue the manuscript you have submitted for publication.
While we realize that you may be disappointed with our decision, we hope that providing you with this information promptly will allow you to submit your manuscript to another journal without the delay entailed by the external review process.
Thank you for the privilege of reviewing your work.
Sincerely yours,
Howard Bauchner, MD
Editor-in-Chief, JAMA
Email: Howard.Bauchner@jamanetwork.org
Phone: (312) 464-2400
Fax: (312) 464-5824
Confidentiality Note: This communication, including any attachments, is solely for the use of the addressee, may contain privileged, confidential or proprietary information, and may not be redistributed in any way without the sender's consent. Thank you.
The above actions are highly, highly irregular. I have never been told by a journal they will consider my manuscript for review and then get rejected on the same day. Typically, if the journal is interested in your work, peer reviewers are assigned, and although this is no guarantee at all it will get published it puts your paper’s publication at least within the realm of possibility. It is extremely weird for them to open a door to publication and then immediately shut it. Good times.
Based on this action, Hector knew the “fix was in” such that he did not even bother to submit his later, even more historically impactful trial on ivermectin. I want to highlight the fact that Hector was one of the first in the world to discover the efficacy of ivermectin in prevention (well, not really true, as it was probably the same time as the group of French nursing homes in April of 2020. But the French report was simply “hypothesis-generating” of course.
Hector proved it by conducting a large, prospective observational controlled trial in Argentina among health care workers who volunteered to take ivermectin prophylactically. He found that among the 788 workers taking ivermectin, not one (0%) got sick while 237 of the 407 (58%) controls did. Like the other rejected papers above, the publication of his study would have singlehandedly changed the entire pandemic. Note his findings were later validated by Kerr and Cadegiani’s huge study (159,000 patients) on IVM prophylaxis in Itajai as well as Professor Waheed Shouman’s RCT in Egypt. Note these are just three of the over a dozen studies all finding massive protection against COVID if you take ivermectin prophylactically. Subscribers, you know what a Forest plot is so I wont explain it again. See below:
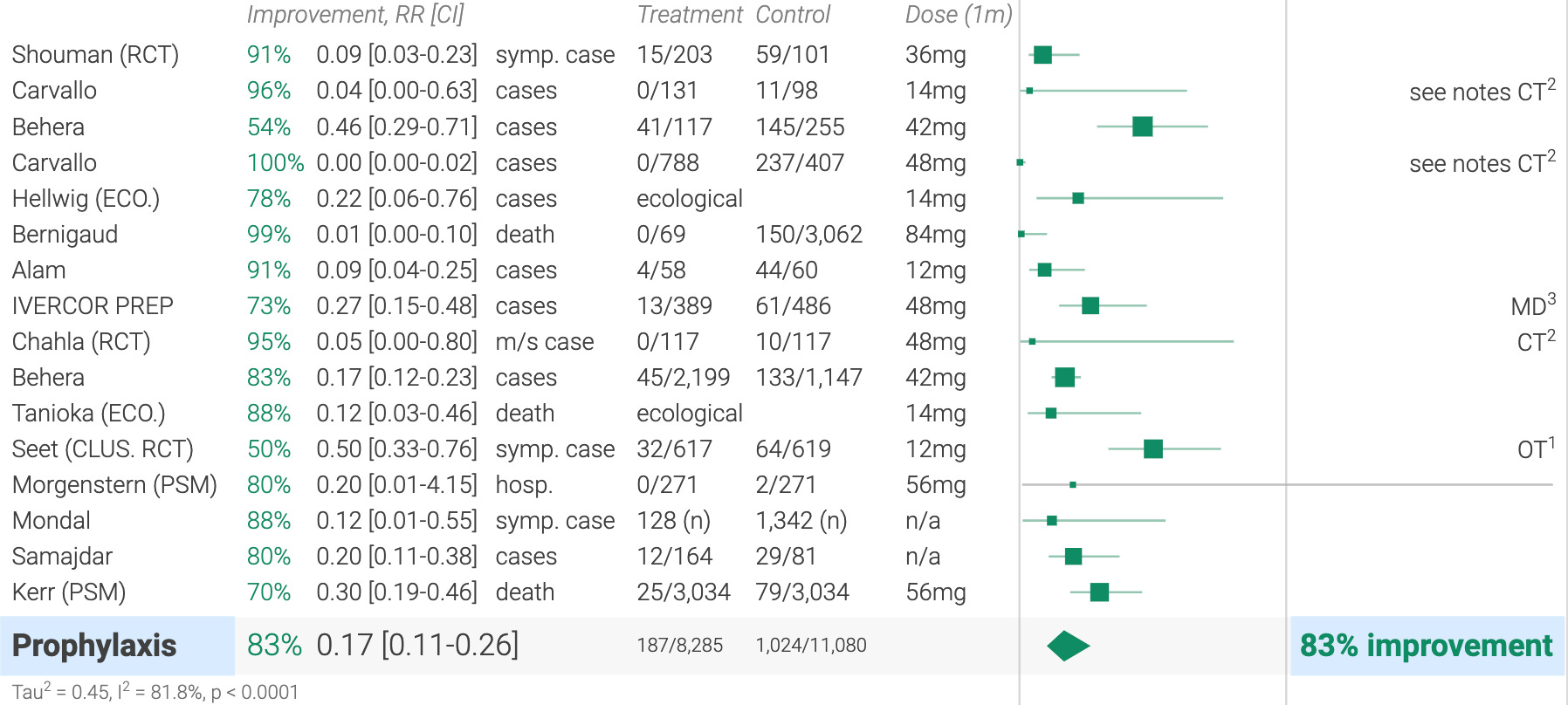
Probably a good time to remind everyone that when the WHO performed their review of ivermectin to form their recommendation, this sentence appeared in their document, “studies on the use of ivermectin in prophylaxis were not included.” Yup.
Hector ended up publishing his trial in a low-tier journal that I have never heard of. Science is broken.
Rejection #4.
Professor Waheed Shouman of Zagazig University in Egypt conducted an even higher quality randomized controlled trial of ivermectin in the prevention of COVID. He found massive reductions in the incidence of infection among those treated with ivermectin. A high quality study from a reputable university. This is what he wrote to me:
Dear Professor Pierre
I hope you great safe times. Yes, our paper was rejected 3 times
1st one, NEJM. It was revised in fast track and was reviewed by 2 or three reviewers. They gave us great ideas that we used to formulate our paper again. Truly they were very helpful although they rejected it. One of the reviewers said it is terrific and very good but the methodology was somehow weak as we needed most of the contacts to do a swab, plus they needed cluster statistics and gave some excellent instructions. 2nd journal after working on the paper guided by NEJM revisions, was Frontiers in Medicine. Frank rejection without revision. Third, EMRO journal. There they rejected after a long delay without revision .
Thank you very much
Yours,
Waheed Shouman
Note his mention of “a long delay without revision.” Like the post-peer reviewed retractions I will cover in my next post about the Editorial Mafia, this behavior is equally unprecedented and it happened to others as well. Basically, the Editorial Mafia started getting ivermectin papers submitted to them, so instead of the quick auto-reply rejecting the paper, they instead “sat on it” for a while. I cannot tell you how damaging that is to researchers. At least with a quick rejection, you can just lick your wounds and try with another journal. But please realize that it is against scientific journal policy for you to submit to two journals at the same time. So you are not allowed to submit to a new one until you are rejected from the one you just submitted to. The journals know this.
I asked my friend and partner Paul Marik, the most highly published practicing intensivist in the history of our specialty whether this had happened to him during the hundreds of papers he has published throughout his career. He told me it happened once, when a journal held on to his paper for 6 months before rejecting. However, he noted that it occurred during a time when manuscripts were submitted in paper, not electronically.
Shouman wrote me back a few months later:
Dear Professor Kory
Thank you for your strong persistent defence for a drug that we won't sell to fill our pockets. But defence is for the needs of human beings. Thank you because this is the soul of our most respected career, Medicine. Even if 10% improvement, for sure it is much more, in treatment and prophylaxis, it means the world deserves to use ivermectin. Our team was the first to conduct a prophylaxis study as you mentioned before and in your last excellent review and analysis in close family contacts. As I found you using the clinical trials as the reference, I'd like to inform you we published it by 1st of february 2021 in Journal of Clinical and Diagnostic Research after a long journey with many journals and 5 months with this journal.
I attach a pdf version of the published article
Yours Sincerely
Waheed Shouman
With the utmost respect to Professor Shouman, his paper, although published and although historic, simply took too long and ended up appearing, again, in a journal no-one has ever heard of.
Rejection #5.
Professor Olufemi “Femi” Babalola of Nigeria conducted a double blind RCT showing numerous statistically significant reductions in important endpoints among ivermectin treated patients. He sent it to the WHO. He shared with me the communications he had not only with the WHO but also with numerous subsequent journals. In the below you will see Andrew Hill appear, clearly at a time before he was fully captured as he is quite open about mentioning that ivermectin papers are getting rejected everywhere.
Jan 6, 2021, 6:22 AM
MS ID#: BLT/2021/285400
MS TITLE: Ivermectin shows clinical benefits in mild to moderate COVID19: A randomized controlled double blind dose response study in Lagos.
Thank you for the manuscript you have submitted to the Bulletin of the World Health Organization. This manuscript is being considered. To follow the progress of your paper please go to: https://submit.bwho.org and log in to your Author Area.
If you have not registered with the system please click on 'Create a new account'. If
you require any assistance with the registration process, please contact the editorial
office at bulletin.submit.ask@who.int.
We thank you for your interest in the World Health Organization and the Bulletin.
Yours sincerely
Bulletin of the World Health Organization
The submission was rejected within days of this (notice the same dynamic happened with Professor Carvallo, the “yes we are interested, whoops, no we are not” dance). But Femi, the corresponding author did not receive the rejection:
Jan 9, 2021, 6:22 AM
MS ID#: BLT/2021/285400
MS TITLE: Ivermectin shows clinical benefits in mild to moderate COVID19: A randomised controlled double blind dose response study in Lagos.Dear Editor,
I received an e mail from your editorial office on the above named article yesterday January 7 ( US CST) rejecting the above said manuscript WITHOUT REVIEW. We were advised to send the paper to a "specialized or regional journal" as it was unsuitable for the Bulletin of WHO.
My supposition was that ALL authors and co-authors received the said E mail.
I therefore did not consider it necessary to share the rejecting without review e-mail
On this basis of your rejection, i communicated your decision to the first and corresponding author, Prof OE Babalola. We then successfully submitted the article to another medical journal for review and publication.
I am, however. surprised to learn that Prof OE Babalola did not (or has not ) received the e mail rejecting the manuscript.
More surprising is the fact that i cannot locate the e mail sent by your editorial office to me, rejecting this manuscript.
Was the e mail recalled ? I may have to contact G mail to know what transpired.
It will be appreciated to if you could clarify what transpired and what happened to the e mail sent to me, and if or whether it was sent in error.
There is a lot of public interest in the submitted work as shown by response on MedRxiv. We want the paper reviewed and published as soon as feasible with the journal that wants it.
I eagerly await your clarification on this matter.
Sincerely yours,
Prof AAL Ajayi MD, PhD
What the hell is this? Here you have the WHO trying to pull some nonsense by not sending the rejection correctly? I don’t even know what to name this bizarro tactic. Suggestions welcome :).
Now, since Femi was one of the Principal Investigators of a registered RCT of ivermectin, he was in contact with Dr. Andrew Hill’s team employed by Unitaid/WHO (err, Gates). Here is Andy writing to all the PI’s, note the bolded sentence below:
Dear Everyone,
I was contacted by a Senior Editor of the journal Lancet eClinical medicine. They published the results from the Spanish trial of ivermectin.
Here is a link to the journal website.
https://www.thelancet.com/journals/eclinm/home
(I think it is important to note that although this was published in the Lancet, it was a trial of just 24 patients (who does that?) and although some benefits were found, it was a statistically negative study in regards to its primary outcome).
The editor would be interested to receive new manuscripts for randomised clinical trials of ivermectin.
Dr Arianna Colosio a.colosio@lancet.com
I know that several research groups have had problems publishing randomised trials of ivermectin. This could be a way forwards.
Best Wishes,
Andrew
Dr Andrew Hill, Senior Visiting Research Fellow, Department of Pharmacology and Therapeutics, University of Liverpool, 70 Pembroke Place, Liverpool L69 3GF, United Kingdom
Femi writes back:
That's good news Andrew. I wish I knew that when our submission was rejected by the editor of Bulletin of WHO. But we have since submitted to QJM, and we have reasonable feedback from the assessors to which we have responded. Fingers crossed.
2. Were your young ones able to utilise the raw data I sent?
Femi
Olufemi Emmanuel Babalola, Professor of ophthalmology, Consultant ophthalmologist Rachel Eye Center, IP HOD Surgery, Bingham University, Jos/Karu, Vice President, MEACO, President, Guild of Medical Directors
Andy Hill speaks truth for one of the last times apparently:
Thu, Feb 4, 2021, 10:08 AM
Hi Femi,
There are so many ivermectin papers rejected. We sent the meta analysis to clinical infectious diseases and they sent straight back in 24 hours with a straight rejection! The editor at Open Forum for Infectious Diseases has reviewed and it should be accepted next week.
Well done with your paper. Maybe these will become easier over time. My team will be looking at the raw datasets next week. Thanks for sending
Best Wishes,
Andrew
Then on April 20th, Dr. Babalola submits his paper to the prestigious Indian Journal of Medical Research. They respond by saying the study is being considered for publication. Then, over a month later, he receives this reply (during the height of the Delta wave in India).
Fri, May 27, 12:25 PM
Dear Sir/Madam,
We express our inability to consider your article for publication. Thank you for submitting to the IJMR.
Editor-in-Chief
This new “delay then deny” tactic is starting to gain steam around the world apparently.
Now, the next one is even more frightening. Recall that pre-print servers have saved millions of lives by getting data from trials of numerous repurposed drugs out quickly. We built our protocols by selecting effective compounds based on their mechanisms, in vitro, in vivo, and clinical data, with the latter often informed using pre-print server data. Povidone-iodine, melatonin, Vitamin D, etc.
What is scary is that Femi tried to post a newer study on ivermectin to the most popular medical pre-print servers called medRxiv. Recognize that pre-print servers.. are pre-print servers. As long as the study involved original data collected by the investigators, the study gets posted after a cursory review of the paper (for ridiculous claims) along with a review of the academic or research backgrounds of the authors. If you pass the smell test, your trial gets posted. Period. Well, unless it is a study of ivermectin apparently:
medrxiv@cshlbp.org via sendgrid.net
Tue, Sep 28, 2021, 3:12 PM
MS ID#: MEDRXIV/2021/263947
MS TITLE: A RANDOMIZED CONTROLLED TRIAL OF IVERMECTIN MONOTHERAPY VERSUS HYDROXYCHLOROQUINE, IVERMECTIN, AND AZITHROMYCIN COMBINATION THERAPY IN COVID- 19 PATIENTS IN NIGERIA
Dear Dr. Babalola,
Thank you for submitting your manuscript to medRxiv and for your email. We are experiencing high volumes of submissions and sincerely apologize for the delayed processing of your manuscript.
We regret to inform you that your manuscript will not be posted. A small number of papers are deemed during screening to be more appropriate for dissemination after peer review at a journal rather than as preprints.
Please be assured that this conclusion is not a judgment on the merits of the work described.
Thank you for your interest in medRxiv.
Best regards,
The medRxiv team
A pre-print server rejected a positive RCT of ivermectin from being posted in a pandemic. I am too tired to test out my “two clicks to Bill Gates” trick, but I am pretty sure if I did, I would find evidence of a donation to medRxiv by BMGF. Can someone let me know if I am right?
Now, from one of Hungary’s top COVID experts, Dr. Szuzsanna Rago who invited me to give a lecture at a symposium she had organized. She has impeccable credentials:
Researcher, primary care physician, IVERCOV project leader in University of Debrecen, Hungary (responsible for ivermectin clinical trial in Covid patients and for the development of the Hungarian ivermectin generic drug.):
Dear Pierre,
Thanks for all your energy you put in fighting for early treatment in Covid-19. I follow your work at FLCCC. Last video Tess Laurie (you and Paul Marik) made as a letter to Andrew Hill is just great and for me is heartbreaking. We also did everything here in Hungary to introduce ivm treatment in Covid but the mainstream “science” coming from the western world was enough for our professors, high ranked doctors and authority to reffered to and it pushed us back to the shadow. I still keep healing our patients anyway.
Although in numbers it is very low, Hungary leads the Covid death rate in Europe.
Yesterday our ivm meta-analysis conducted by 3 universities of Hungary by my lead was rejected at editor level from Infection journal. The editor did not even send it to reviewers….
We analyzed ivm efficacy on SARS-CoV-2 viral clearance in mild-moderate Covid. The result is (of course) significant in favour for ivm, the evidence level turned very low because only 3 studies fitted in our PICO. But the result is positive. The deadline of our search was 1/2021, so a year ago. And we are still not able to publish it.
Could you please recommend a journal who would accept our ivm paper without any censorship?
Thanks a lot,
Zs
Zsuzsanna Rago
Hungary
Science is dead. Or at least any science that has financial implications against or for Pharma interests is dead. We need a parallel system of journals which have zero influence by Pharma. We need institutions we can trust and those journals are not. They are dead to me and Paul after careers of believing in everything they published. No longer can we read them knowing that what appears in those journals is only and I mean only, what Pharma “allows to appear” in those journals. The NEJM, Lancet, BMJ, JAMA, Cochrane Library all have blood on their hands.
As the world came under attack by a novel and highly transmissible respiratory virus, the medical journals had a critical, life-saving responsibility to publish any and all studies of treatments that were either potentially effective or substantively effective in either preventing or treating the disease. They abdicated their primary responsibility. Millions have died as a result.
I just want to say how much I appreciate all the subscribers to my Substack, and especially the paid ones! Your support is so greatly appreciated.
P.S. I opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.S We are organizing the world’s first conference on understanding and treating Spike protein induced disease (i.e long haul COVID and vaccine injury syndromes). Tell your doctor to come. Link below:

P.P.P.S. I am writing a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for:
CVS is now a major part of Pharma marketing/advertising. Called to refill a simple antibiotic prescription. I had to endure minutes of a CVS recording promoting the new APPROVED Covid booster and 14, FOURTEEN, other vaccines available now!
Disgraceful, horrifying, shameful. Thank you for your great work, Dr Kory. Dr Angell is a treasure.
Philanthropaths!!!! Thank you, Pierre 😄💗🙏
For those who don't know the source, here is my three-part series, "Anatomy of a Philanthropath":
• “Part 1: A Mostly Peaceful Depopulation” (https://margaretannaalice.substack.com/p/anatomy-of-a-philanthropath-dreams)
• “Part 2: Downloadable Digital Dictatorships” (https://margaretannaalice.substack.com/p/anatomy-of-a-philanthropath-dreams-947)
• “Part 3: Yuval Noah Harari: Not the Man We Think He Is?” (https://margaretannaalice.substack.com/p/anatomy-of-a-philanthropath-dreams-3fd)