

The Criminal Censorship Of Ivermectin By The High Impact Medical Journals - Part 2
Although Pharma got the high-impact journals to reject all positive ivermectin study submissions, they first got them to retract already published papers despite zero evidence of fraud. Unprecedented.

In my first post on the devastating censorship of ivermectin’s efficacy by the worlds’ highest impact medical journals, I outlined the four censoring methods they used to censor nearly all COVID science that was “inconvenient to Big Pharma’s interests.” They did this as follows:
Rejected all positive trials of ivermectin, even, and especially, the highest quality trials, starting as far back as May of 2020 (Part 1 detailing these actions is here).
Retracted positive ivermectin studies from lower-impact journals after they passed peer-review and/or were already published.
Published fraudulent trials and fraudulent meta-analyses, with the latter approach identical to that employed in the WHO’s corrupt recommendation against ivermectin here. This is a known Disinformation tactic called “the Fake,” defined as “conduct counterfeit science and try to pass it off as legitimate research.” I will review these in my next post.
Published numerous anti-ivermectin editorials, which is also an already named Disinformation tactic called “The Diversion.” Next post.
I just discovered a problem with my posts attacking the high-impact medical journals. They are out of chronological order. Part 1 of this series detailed all the high-impact journal rejections of positive ivermectin studies but, in reality, those rejections only began after those editors had already retracted published, positive ivermectin studies. So, if you haven’t read Part 1 already, read the below first, and then read Part 1.
RETRACTIONS
1. Frontiers in Pharmacology Journal - The retraction of the FLCCC’s comprehensive narrative review paper in February 2021 was our first verifiable indication that Pharma was on the move against ivermectin. Actually, scratch that. Pharma’s first verifiable shot across the bow of HMS Ivermectin occurred on February 4, 2021, two weeks prior to our papers’ retraction. I woke up that day to texts and emails of alarm from the FLCCC team that Merck had posted a fraudulent statement against ivermectin on their website. Clearly written by their PR department, and not, as they claimed, by “company scientists.” Remember this one
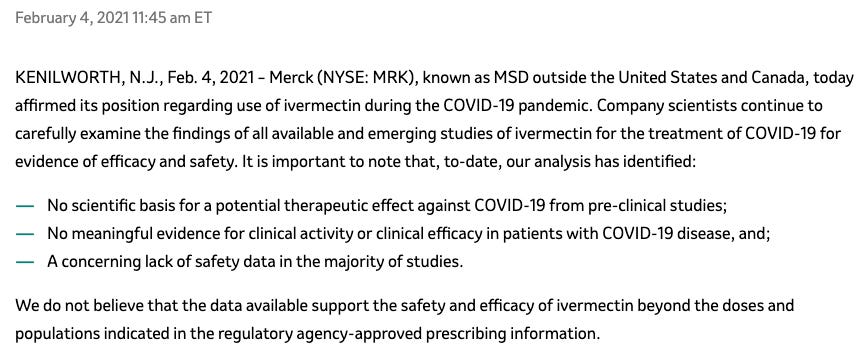
That shook up me and the FLCCC up big time. A corporate behemoth just making up shit up and posting it on their website. No data, no analysis, no authors. Well, it wasn’t just the fact they committed such a brazen act, I mean they are Pharma, but what shook us most was the ridiculous media fanfare that it ignited. They post lies and then corporate media immediately generates headlines across the world, warning Earth’s citizens that ivermectin doesn’t work in COVID. A corporation with a documented history of criminality posting something verifiably false on their website which immediately gets accepted as a global truth. Holy cow.
This was indeed a truly shocking and powerful display of influence and control. I didn’t yet know at the time that Pharma had such immense global media power. I didn’t yet know that an entire generation of science reporters in legacy media had died or resigned or had instead cravenly allowed themselves to be muzzled and/or co-opted to service Pharma’s lies.
But here’s the thing, the FLCCC (i.e the “Bad News Bears” of the pandemic war on science) had just hit two home runs, the first one being my Senate testimony going viral and the second being our paper’s abstract posted on the Frontiers of Pharmacology journals’ website. Then we hit another (“back to back to back home runs!”) after Paul Marik, myself, and Andrew Hill presented all the existing ivermectin evidence to the NIH on January 6, 2021. As a result of that presentation, weeks later, the NIH COVID Treatment Guidelines committee changed their previous recommendation on ivermectin from “do not use outside of a clinical trial” to a more neutral one which said “there is insufficient evidence to recommend or not recommend” use in COVID.
Whoa. FLCCC 3, Merck/Pharma 0. Now imagine that it started to get even worse for Pharma (which never happens). As a result of my testimony, our paper, and the NIH recommendation change, a support for a generic, repurposed medicine was building. Their “market position” was being pushed back. To make matters worse, the FLCCC’s early combination prevention and treatment protocols were being increasingly disseminated, not only in the U.S, but around the world, from India to Ukraine and beyond. FLCCC 4, Merck/Pharma 0. Not looking good for Pharma.
Yeah right. The lead didn’t last very long.
What I think really triggered Merck’s move was that, as a result of the above efforts, ivermectin prescriptions by American physicians were shooting through the roof. Losing early and badly, Pharma started throwing at our heads, high and inside. Again, it was deeply intimidating to see just how quickly they were able to ignite a bonfire of negative press against ivermectin across the world’s media. Whoa. Note that at that time there was not a single “large, rigorous” trial showing that ivermectin did not work (those fraudulences would come later). Instead… all the trials were positive wherever you looked. Scary stuff if you are in an industry that is salivating over an emerging $100 billion plus market that, if ivermectin were “proven” (notice the quotes) to work, it would absolutely obliterate the profit potential of.
So instead they just posted a statement by their PR Department that ivermectin doesn’t work without providing any supportive data or scientist author names. One of the statements even tried to inject doubt as to ivermectin’s safety, a drug they knew was one of the safest in history. Not subtle. How did they get away with this? Well, maybe it was the fact that it was met with zero scientific criticism from academia or major media or our “trusted public health agencies.”
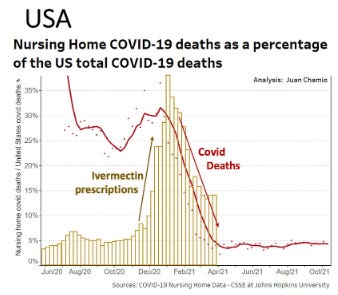
If a rapid rise in ivermectin prescriptions was happening in the US, the same thing was likely happening in other countries (such was the power of the little ‘ole FLCCC?) Although I don’t have that data, Merck absolutely did. Look at the rise in U.S ivermectin prescriptions that occurred in the wake of our paper (Nov 13, 2020) and my Senate testimony in Ron Johnson’s hearings (December 8, 2020.) Now look at what was happening just before Merck posted their criminal statement on February 4th, 2021. Spurious correlation?
Others in the FLCCC were not as disturbed by Merck’s attack on ivermectin because they interpreted Merck’s insane move as validation that we were “over the target.” They were confident that we were onto something and that we were winning because Merck was running scared. I wan’t so sure.
The reason I say this is because during that period I first began to have thoughts of concern for my well-being. I was worried as the father of three teenage girls who was just becoming aware of Pharma’s documented record of mass killing in the wake of toxic product launches (Vioxx, Avandia, Zyprexa, Topomax, Oxycontin etc, and here we were starting to “poke the bear.” A very big and very bad bear. I started making more of a point to lock the house. I kept a bat closer to where I sat or slept at night. Yes, a bat. So stupid.
Now, what I have learned since that time is that nothing gets Pharma to engage in Disinformation more so than where there is a documented rise in prescriptions of a repurposed drug. Noth-ing. I learned this mostly from when the later, “horse dewormer” PR campaign against ivermectin was launched around August 26th, 2021. See the below record of weekly ivermectin prescriptions in the US in August of 2021 and look back to the prior hump in February preceding the Merck statement above:
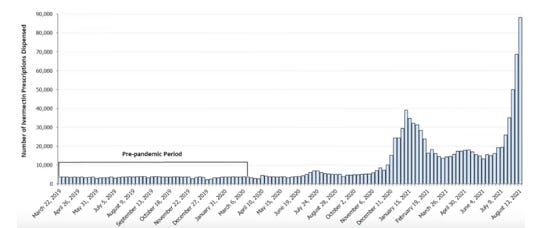
Methinks they hired a more powerful PR firm between the two humps because the horse dewormer campaign was way more devastating in impact compared to the lame Merck website statement. Plus, by the time of the horse dewormer campaign, Pharma had published the first of a series of fraudulent trials and meta-analyses in high-impact journals to support the campaign, which is why I think the corruptive actions of the “Editorial Mafia” are the foundational cause of millions of preventable deaths.
Without the journals and their craven non-whistle-blowing editors, none of the above would have been possible. If only Marcia Angell had not retired twenty years ago. Forgive me for I foreshadow.
Thinking back to that time, before I knew what I just related above, it pains me to have to remind myself of the depth of naiveté I still possessed, even after the Merck statement and the sudden retraction of our paper which I will detail below. I am embarrassed to admit it, but despite those impressive opening salvos in the war, I still did not know “we” were at war. Or if I did, I did not know it was global. Because I still expected the WHO to fully end the pandemic the next month with a worldwide recommendation for ivermectin in the prevention and treatment of COVID. The pandemic would soon be over!
But hear me out as to why I still had hope at the time. Recall that in June 2020, we had the experience of the WHO issuing a recommendation for corticosteroids which became the standard of care overnight. This occurred weeks after my first Senate testimony advocating for corticosteroids in Senator Ron Johnson’s historic hearings in May of 2020. Which, I might add, was months after the FLCCC had been screaming at the world to use corticosteroids in hospital patients. I know, I know, it wasn’t because of us but still, such a sudden and global recommendation had happened once, why couldn’t it happen again?
Ugh. Let’s get back to the story of our paper’s shocking retraction. After my testimony and the posting of our paper on a pre-print server, we knew we needed to publish in a medical journal. And quickly. We were in mid December 2020 when I learned of a then well-regarded journal called Frontiers in Pharmacology that was putting out a special issue called “The Use of Available Medicines in COVID-19.” Perfect.
Fun fact: the scientist who suggested the topic for this special issue was a guy named Robert Malone. Yes, that Robert Malone. I reached out to Robert as he was the Guest Editor of the Special Issue. He was interested in our paper and thus invited our group to submit it to his issue. He selected four colleagues of his to review the paper, three of them being senior scientists at the FDA, DOD, and NIH. The fourth was an ICU specialist in the Bronx.
Robert was awesome - he commandeered a rapid peer-review of our paper over the Christmas Holiday 2020 by harassing the reviewers repeatedly to submit their initial reviews as well as their subsequent and numerous requested revisions. Admittedly, I was the one making Robert harass them, but only for speed because we knew people were dying and that the publication of the paper would have a major impact in stemming the rising tide of dead COVID-19 victims.
Three long rounds of rigorous peer review ensued and it was finally accepted by all the reviewers for publication! Yesss!
Frontiers in Pharmacology quickly posted the abstract on their website where it became the most viewed abstract in the history of that journal, and one of the most viewed at almost any of the Frontier’s journals. There was a lot of attention on our paper.
This is where everything went sideways and fast.. Week after week went by without the journal sending me a proof to approve. It was an on-line journal! Come on man, just copy-set the paper, I will review it and then you publish it! The world will be saved!
That is, historically and tragically, not what happened. To make a long story short, after weeks of harassing the journal representatives, I finally wrote an exasperated email in which I accused the journal of scientific misconduct and stated that the FLCCC was prepared to go public with our complaint unless our suspicions could be satisfied. Robert wrote a less inflammatory email right after mine, asking the journal to clarify why, not only my paper, but also another one that Robert had submitted on famotidine was being held up.
Pretty quickly, the chief editor of all of Frontier’s journals (Frederick Fenter - never forget his name) got involved and set up a meeting with Robert. At that meeting, he reported that “someone had complained” about our paper’s conclusion, which was to “globally and systematically deploy ivermectin in the prevention and treatment of COVID-19.” He said that as a result of the complaint, he sent the paper to some anonymous reviewer… who recommended to retract the paper.
Let’s review how crazy this was. Historically, the only reasons for a paper to be retracted is when evidence of fraud or scientific plagiarism is uncovered. In our case, after passing peer-review by 4 experts, suddenly some shadowy, anonymous 5th reviewer disagrees and instead says to retract the paper. And the editor listens to that reviewer. What?
Most important is that this reviewer did not detail anything specific to revise, just that they “felt” the data presented did not support our conclusions and that it should be retracted and further, that no opportunity to revise the paper should be offerred. The lack of an offer to revise the paper was, to me, the definitive proof of their malevolence. Standard practice in scientific manuscript submissions is that when a peer-reviewer has a problem with a paper’s analysis or conclusion, they instead make a suggestion to revise it by providing their opposing interpretation of the data or with some superior knowledge of the topic instead.
Sensing tragedy, I made a lame, pathetic plea by revising the paper to a more muted conclusion, hoping to satisfy Fenter and his anonymous reviewer (Hi Bill!). See how naive I was? But I was convinced that even a softened paper would be massive in impact. And as weird or megalomaniac as this sounds, I knew the world depended on the paper for its salvation. Ugh. Yucky I know.
But imagine being in a state where your knowledge or expertise could literally save a world in devastation. Despite mountains of self-doubt, I could not convince myself otherwise. I knew this paper had to get published or people would die. Lots of them. The world depended on this paper’s conclusions. I swear I was as unsettled as you are at this thinking and its implications.
But then the reality of the world hit hard. Frederick Fenter declined to allow me to revise the paper, and instead suggested that we instead revise and re-submit the paper as a new submission for another round of peer-review. I laughed as hard then as you are now at this ludicrous proposition. What, so they could sit on it again for months and then reject or retract again? Clown world.
But this retraction was absolutely unprecedented in our careers. The FLCCC had collectively published over 1,500 scientific manuscripts over 4 decades and had never had a paper retracted after passing peer review with no complaint of fraud or plagiarism. That is the point of peer review. And the paper had undergone a series of revisions until it was finally accepted by a consensus of 4 experts. Until it wasn’t. Here is an article in the Scientist reporting on this scandal. Do not expect to find the truth in that article.
After our paper got retracted, Frontiers then put a hold on all the papers under review in Robert’s special issue. Robert and his co-editors had a tense meeting with the journal editors as well as an outside expert who was brought in to review all the papers. During these discussions, it became clear to Robert and his colleagues that the whole process was fraudulent and that the “expert” was not making scientific or ethical sense. Outraged, they immediately resigned en masse as described in this article in the Scientist. The special issue was dead.
After the FLCCC was rejected, we licked our wounds and quickly submitted to a different journal. I knew the editor of that journal because he had initially invited us to submit to him, but unfortunately it was just after I had tragically chosen Frontiers in Pharmacology. I actually knew the editor from my youth and so trusted him but still wanted to verify that he wouldn’t pull the same nonsense as Frontiers. He deeply reassured me by his acknowledgment of the unfairness of what happened and his “knowing” lack of surprise at what we endured in the face of “an advancement in science” as he characterized it. It was clear he knew of the “Simmelweis Reflex.”
So, he simply asked that I submit to him the Frontier’s peer-reviewer comments, including the history of our revisions. He carefully reviewed them and then immediately accepted our paper for publication!
Shockingly, it quickly became one of the most popular papers in recent history using the altmetric score (a “popularity” score which was only invented in 2011 so I don’t want to overstate its importance). At the time it was the 11th most popular paper out of the last 22 million publications (now it is #58).
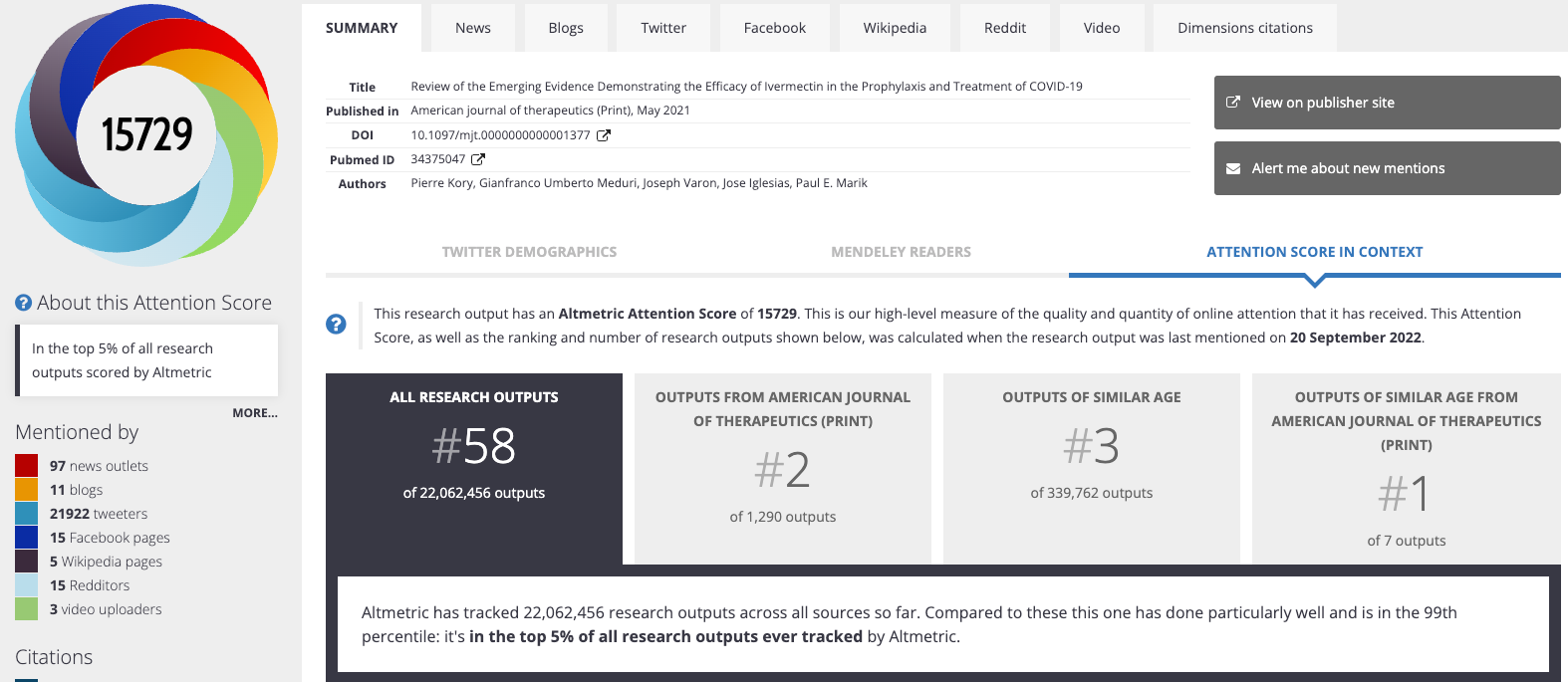
Tess’s later review paper became even more popular. As you can see below, as of today, hers is the 8th most “popular” scientific publication in the past decade. #8 out of the last 22 million scientific publications.
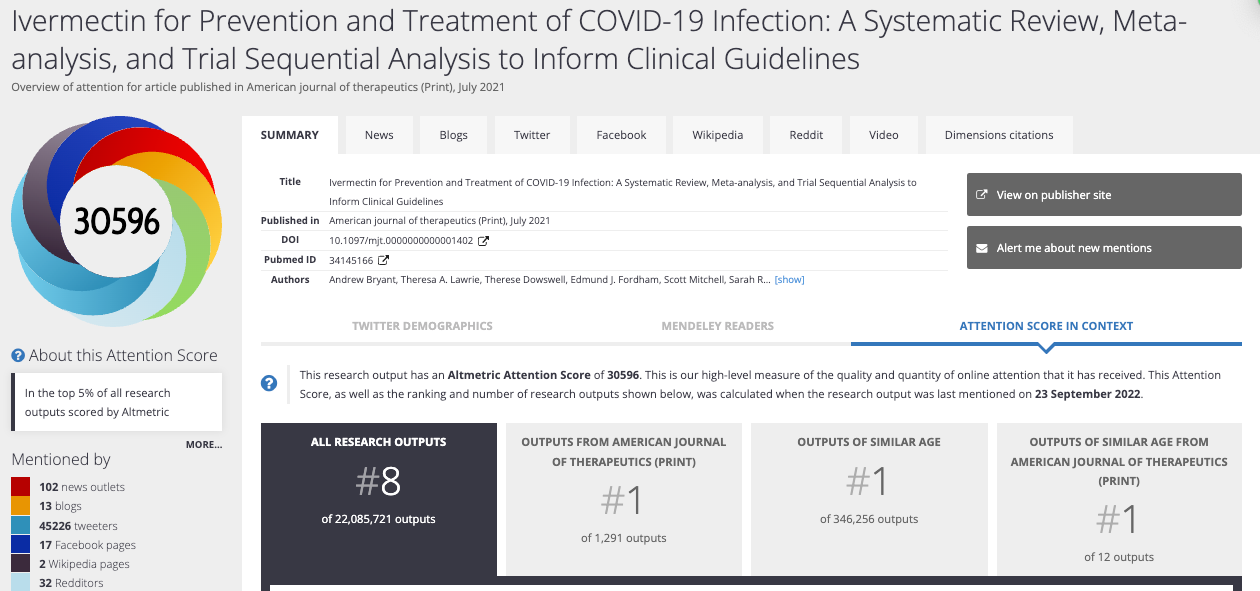
Yet no-one has ever heard of her (or our) paper. And, unsurprisingly, neither moved the national or international regulatory agencies or corporate media to acknowledge. This is why I stress that the whole “game” is based on “high-impact medical journals.” Anything outside of those top journals is ignored by wider society.
The Lancet - Respiratory Journal
This novel practice of retracting peer-reviewed papers continued. Recall from Part 1 that Tess Lawrie and Andy Bryant’s review proposal was rejected by the Cochrane Library after initially being accepted and before actual submission. They were then told by Cochrane to submit to another journal.
Now, although I already wrote about Cochrane’s rejection in Part 1, I just came across an email from Tess which explains in greater detail how that rejection went down. So, I am adding to my prior post here as I found it sort of chilling. Tess wrote that Cochrane’s sudden turn-about was triggered only after she alerted them that Andy Hill would no longer be an author. Obviously she did so only after she discovered Andy had severe conflicts of interest (recall he admitted to her on a recorded zoom that he was allowing his sponsors to manipulate his paper).
From Tess to her and now my colleague Edmund Fordham:
On Jun 15, 2022, at 6:40 AM, Tess Lawrie <tess@e-bmc.co.uk> wrote:
Thanks Edmund, if i can just correct the point on Cochrane accepting the rapid review protocol - it went down like this: We submitted the protocol on Friday 15th Jan to Cochrane’s Toby Lasserson and Paul Gardner, I had the meeting with Hill on the 18th Jan and wrote to Toby on the 19th (after requesting a call on the 18th) about Hill’ competing interests, saying that he could no longer be involved in our review.
After that Toby went quiet and I reached out to Karla Soares Weissner to find out what was going on. I got a reply on the 25th jan - will forward all this correspondence with you. Revisiting it, I realize that it makes for fascinating reading. We should write it up for substack. Incidentally, I recorded the meeting I had with Toby during the first week of feb where I recall him looking rather uncomfortable too as he scraped the barrel for reasons as to why he was facilitating the German review and not ours.I have never re-watched this meeting - perhaps now is the time.
Dr Tess Lawrie
Director/CEO
C: EBMC Ltd /EbMCsquared CiC W: www.e-bmc.co.uk / www.ebmcsquared.org
Wow. That was the rejection from the Cochrane Library. Now, let’s talk about the ensuing “retraction” from The Lancet Respiratory, a very highly regarded journal. Tess et al’s submission to that journal was initially accepted and then sent out to experts for peer-review, also using 4 experts (some journals only use two). The paper passed their extensive peer-review and thus should have been deemed “accepted for publication” as per traditional, long-standing procedure. Problem: there is no longer such as thing as the traditional, long standing procedure in Science during COVID.
To wit, here is Tess writing to a senior health official in Australia (an evil health bureaucrat who has blocked ivermectin at the highest levels in Australia throughout the pandemic). She tied to explain to him what happened to her paper after he so “innocently” inquired:
March 22, 2021
Dear Prof. Skerritt,
The Journal’s decision was as follows:
" Unfortunately, after some lengthy discussions with the editorial team, we do not feel that we can pursue the paper at The Lancet Respiratory Medicine. It was felt that there is just not enough evidence at the moment on ivermectin to be confident in a study such as this at this time, and we would encourage waiting until several more studies are published to help improve confidence in the paper. We don't doubt that this is an important paper, and would likely be widely picked up, and as such, we want to make sure that it includes as high-quality evidence as possible to ensure we spread a message that is strongly supported by the evidence. Therefore, on this occasion, we have decided not to publish your manuscript, but would perhaps consider an updated paper that includes more published evidence later down the line.
From Tess to Skerritt:
The findings of our review suggest that ivermectin may have a significant impact on excess deaths from covid. We graded the evidence as low to moderate certainty very conservatively using the GRADE approach. We have had our grading independently checked by an experienced Argentinian team who routinely do evidence grading for the World Health Organization and they graded the evidence on deaths as moderate certainty using the WHO’s standard operating procedure. Moderate certainty evidence means that ivermectin probably significantly reduces deaths from covid. There are no interventions currently granted emergency use authorization that can be said to have this effect. I would also like to point out that is more evidence on ivermectin safety than any other intervention currently in use against covid."
I would like to point out that after the Ebola crisis the WHO issued a statement about sharing results in times of health emergencies. I refer you to it here:
https://www.who.int/medicines/ebola-treatment/blueprint_phe_data-share-results/en/
They emphasize the importance of pre-prints as a way of facilitating the sharing of important information that can save lives. They also say that "Journals should not hinder the sharing of data that could help mitigate the impact of such emergencies.” Unfortunately, this seems to be the case with ivermectin, where at least 4 reviews of the evidence and many studies remain on pre-print websites, as authors struggle to get them published.
I attach a few here, as well as the evidence to decision framework document that has been prepared according to the methods I usually employ when employed as a guideline methodologist by WHO.
If you have any question, please do not hesitate to contact me.
Kind regards,
Tess Lawrie
Dr Theresa Lawrie
Evidence-Based Medicine Consultancy Ltd Bath, United Kingdom
+44 7826 939464
So, Tess satisfied all 4 expert peer-reviewers of her paper. Further, to achieve this, she softened her conclusions greatly, to do so. Note that she had graded the trials evidence quality as conservatively as possible so as not to be accused of “over-interpreting.” One of the safest medicines in history with a “low to moderate certainty” that it reduces mortality based on 18 randomized controlled trials. Yet the Lancet Respiratory editors rejected it, saying… “there need to be more trials done.”
Recall that Remdesivir was launched across the U.S and world based on one trial which showed zero, and I mean zero, impact on mortality. Similarly, Pfizer sold billions of Paxlovid based on just one trial, which also showed no impact on mortality.
Behold Pharma’s “one and done” regulatory fast track system that they have built over decades with lots of influence and cash. Meanwhile, for poor little ivermectin: 18 RCT’s is not enough. Fun fact: ivermectin now has 91 controlled studies, 41 of them randomized, including 134,052 patients. The average estimate of benefit based on all these trials range from an average of 62% in treatment to 83% in prevention. Still, it is not recommended by any advanced health economy in the world. Clown world.
After the editors balked, Tess followed our lead and submitted her paper to the same journal as we had, The American Journal of Therapeutics. Although headlines were launched after this publication, none were in major media. People kept dying as not enough new doctors were being taught to use it to treat COVID.
Now, If you think we are done with the high-impact journal retractions, it is only because I split this post into two parts. The next post details even more insanely corrupt retractions than the above. Stay tuned. Subscribe if you haven’t.
I just want to say how much I appreciate all the subscribers to my Substack, and especially the paid ones! Your support is so greatly appreciated.
P.S. I opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.S We are organizing the world’s first conference on understanding and treating Spike protein induced disease (i.e long haul COVID and vaccine injury syndromes). Tell your doctor to come. Link below:

P.P.P.S. I am writing a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for:
Brilliant piece. This medical layman fails to comprehend how Ivermectin saved enough millions of lives to win the Nobel Peace Prize then later got demonized as 'horse paste' and unfit for human consumption by America's FDA. Had Ivermectin (and other successful early approaches) been employed early on, millions of lives might have been saved around the world - this, months before the first so-called 'vaccine' ever got injected into the first arm.
'Mass murder', on the part of those who censored life-saving treatments? The shoe fits.
C'mon, legal profession... Get off your duffs. there HAS to be a class action suit somewhere in this.
I don’t know how this could be pulled off, but I would love to see a study/paper submitted to peer-reviewed journals with Paxlovid substituted for ivermectin, and when the paper is accepted, the authors reveal that the drug tested was actually ivermectin, and the journal would be forced to proceed with publishing what they had already accepted lest their bias be revealed.
Perhaps Peter Boghossian, James Lindsay, and Helen Pluckrose can give some pointers on how to submit hoax papers—although it’s probably a lot easier to get away with in the social sciences ;-) (https://www.nytimes.com/2018/10/04/arts/academic-journals-hoax.html)