

The American Board of Internal Medicine's Longstanding War On Doctors Is Escalating
The ABIM's history proves their present actions are political/financial and not scientific. They are making examples of us "dissenters" to scare the rest of the country's docs to keep quiet.

The unholy alliance of industry captured high-impact medical journals, federal public health agencies, professional societies (ABIM, AMA, APHa etc), and most importantly, the state medical licensing boards directed by the Federation of State Medical Boards (FSMB) are still going hard after us “dissenting” doctors. You know, those of us that very publicly called out the unscientific policies implemented by corrupted policymakers in a directed pursuit of profits and power. Their actions trying to silence us (and to scare other doctors from speaking out) are escalating.
Recently, what I call the “misinformation committee” of the American Board of Internal Medicine (ABIM) voted to strip Professor Paul Marik and myself of our Board certifications. To best understand why they would do this, I think it is important to review what the ABIM is, how it operates, and then detail their absurd attempt to paint us as misinformationists by using disinformation.
Let’s trace my current relationship with the ABIM to today:
At the end of my training, I became Board Certified by the ABIM in three specialties (Internal Medicine, Pulmonary Diseases, and Critical Care Medicine).
What is the ABIM? Well, from this devastating article by Kurt Eichenwald, an accomplished corporate investigative journalist who did a devastating takedown of the ABIM and its officers in a Newsweek piece in 2015:
The ABIM is a purported nonprofit that certifies new physicians as meeting standards of practice. Beginning in the early 1990s, the ABIM ordered certified doctors to be recertified, again and again. Without the ABIM seal of approval, lots of internists and subspecialists can't get jobs and can't admit patients to hospitals. So by taking advantage of that monopolistic power, the ABIM has forced hundreds of thousands of physicians to follow recertification processes that doctors complain cost them tons of money (paid to the ABIM), require tons of time (taken from families and medical practices) and accomplish nothing.
In many doctor’s opinion, this cash grab of the ABIM by selling “certifications” is a corrupt farce. There is no evidence that certifying doctors in this highly costly way does anything to improve the quality of care delivered. The ABIM has not only refused to produce data showing the program improves patient care but also hasn't conducted any studies on that matter. In fact, the ABIM and its related organizations are:
harming American medicine and diminishing the quality of scientific research, pushing physicians to close practices rather than wasting time on expensive and frustrating busywork, and forcing specialists to play a game of medical trivial pursuit. (Even Baron has admitted that he was tested for recertification on topics he never used in his practice.)
But it sure does generate cash for ABIM executives. Note that Board Certification used to simply be a sort of “honor” denoting that the member passed a more rigorous examination in their specialty. That “honor” comes at a price though:
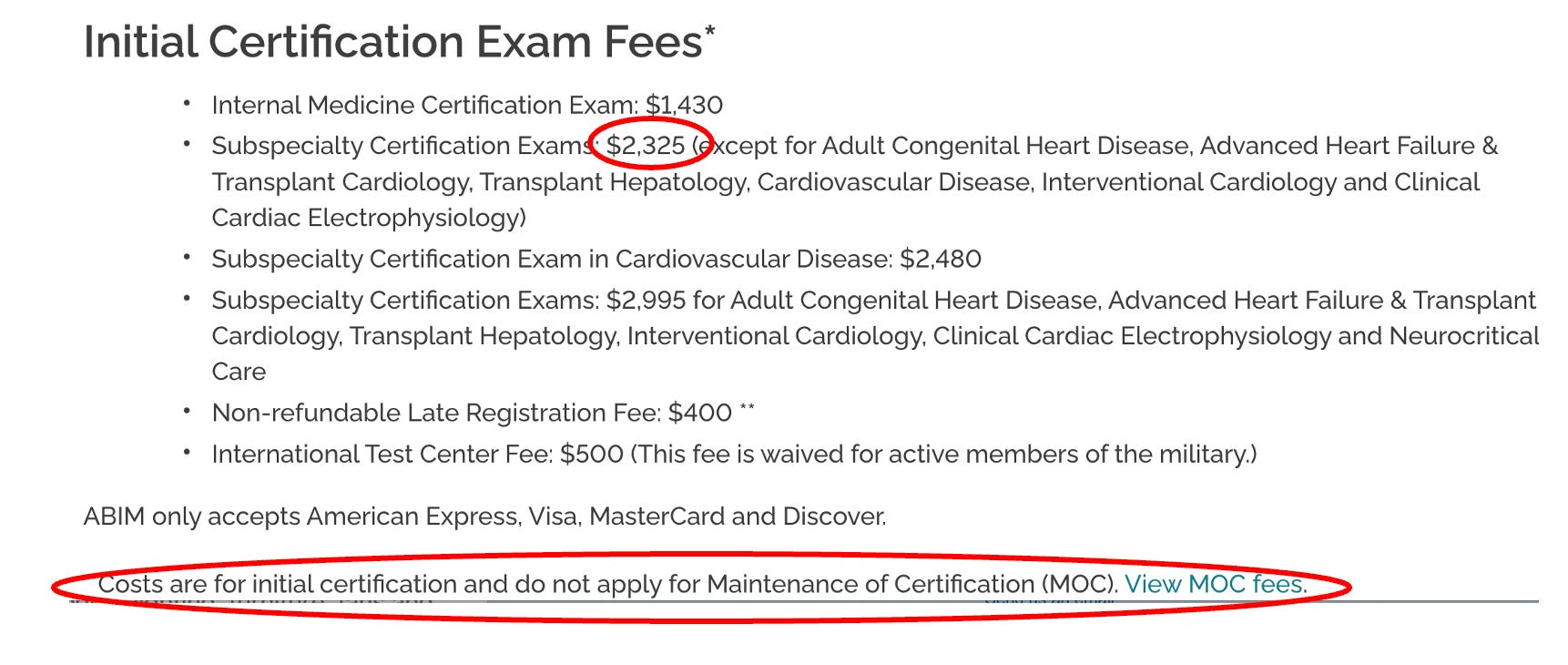
Since I am (was?) Board certified in 3 specialties, lets do some math as this is what it costs me to re-certify every ten years:
$1,430 for Internal Medicine
$2,325 for Pulmonary Diseases
$2,325 for Critical Care Medicine
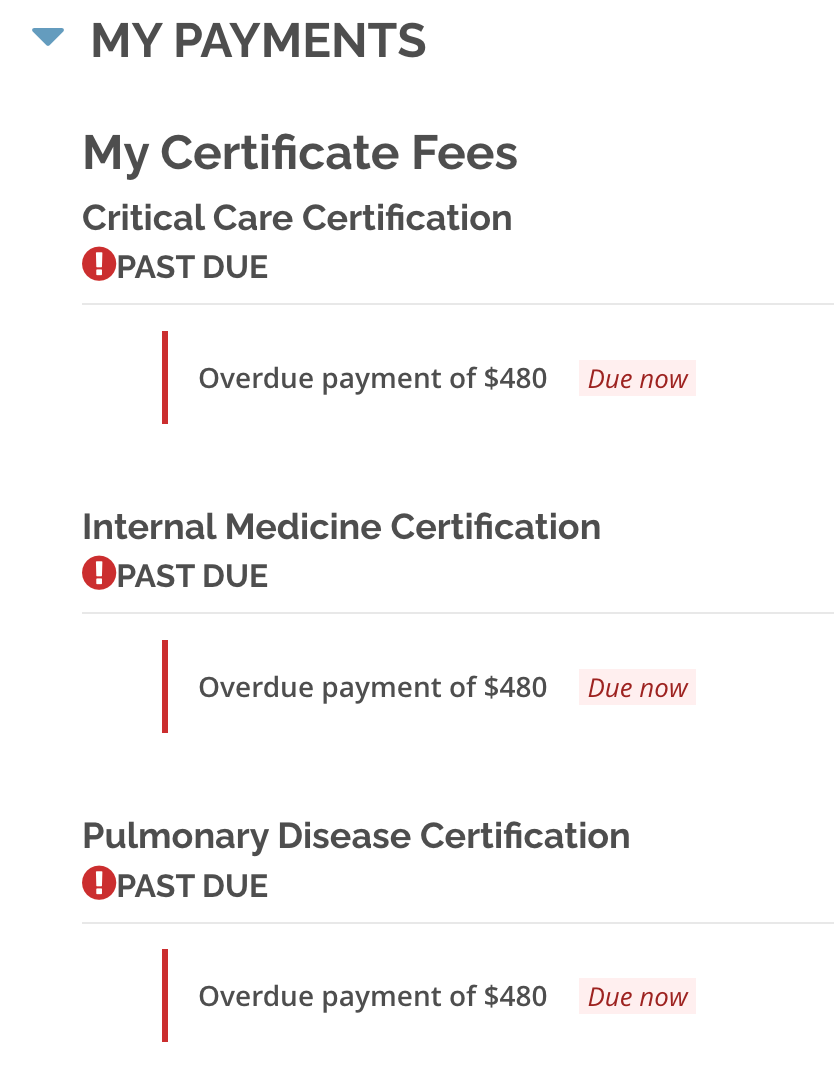
But wait, we are not done yet. These bastards were not making enough money with once-every-ten-year recertification exam fees, so they invented a new program of annual busywork education requirements which they called Maintenance of Certification (MOC) which costs you $220 every year for every certification (plus late fees if you forget). To wit, I went into my patient portal and discovered.. I owe them $480 for each of my certifications!
And get this - that money essentially goes to ABIM executive salaries and pensions and other dubious private investments as described by Eichenwald where he details the insane lengths the ABIM goes to "hide” the compensation and pension data on its executives. What is worse is that ABIM certification has now been made a requirement of employment as a faculty member of academic medical centers and hospitals and is also a requirement to be on many insurance company panels (these actions further strengthen the control of doctor behavior).
Doctors have started publicly slamming the group in industry publications. "ABIM is imposing on us an onerous and ill-conceived tool, one that most physicians agree is irrelevant," Dr. Karmela Chan wrote in Internal Medicine News. "I am glad this conversation is happening, because, frankly, the process was enough to make me want to quit being a doctor." Further, in a recent poll of 2,211 physicians conducted on a doctors-only website called Sermo, 97 percent of the respondents criticized recertification.
Richard J. Baron, the ABIM CEO that sent letters threatening decertification to me and Paul, makes close to a million dollars a year, however that data is almost impossible to find due to the ABIM’s multiple attempts to obscure it as well as its spokespeople avoiding answering any inquiries on the topic. Here is a summary of Eichenwalds findings on the ABIM:
In 2015, they were 5 months late in filing their publicly available financial report with the IRS (that several journalists were very interested in).
The report is full of obfuscations and anomalies of reporting of not only the actual money earned by the executives, and particularly Baron, but his financial conflicts of interest are even better hidden.
A big percentage of the ABIM’s millions was in the form of cash to one former employee.
The ABIM in 2013 had 57 million against liabilities of 105 million - while Baron was going around saying that its assets are three times its liabilities (this was a 100% lie. When I get to the ABIM’s response to our defense letter, remember that what liars do is.. lie).
It lost $4.8 million on $55.5 million in revenues, no small feat and almost entirely due to a bloated payroll.
It also claims it spends no money on lobbying while it spent between 100K to 160K annually to lobby Congress on Medicare and Medicaid (another lie).
The data on top officers compensation is so obscured and fragmented, Eichenwald reported that he had found it much easier to discover executive compensation at Enron, Worldcom and Adelphia - all famous for lying on tax filings. Again no small feat (to be one of the top corporate liars in the U.S).
Officers “double dip” - former CEO Christine Cassel got $741K from ABIM and $247K from the ABIM “Foundation” (slush fund for ABIM officials) and also got $219K in “other compensation” - totaling $1.2 million for one year. (Nice gig if you can get it).
But wait, we are not done. Cassel also got $504K in “deferred compensation” for a total of $1.71 million more that year (six times the median compensation for similar sized non-profits). Six times.
Then there is this doozy of an article which came out this week in The Defender by Children’s Health Defense, detailing the ABIM CEO Richard Baron’s conflicts of interest:

Some of the most disturbing reveals:
“The head of a national medical organization who publicly called for doctors to lose their licenses unless they supported government narratives on COVID-19 treatments and vaccines concealed his relationship with a public relations firm whose client list also included Pfizer, Moderna and the Centers for Disease Control and Prevention (CDC).
Dr. Richard Baron, president and CEO of the American Board of Internal Medicine (ABIM) is a client of Weber Shandwick, investigative journalist Paul D. Thacker reported on Wednesday.
Note that I went after Weber Shandwick in my book, “The War on Ivermectin” where I argue (without proof, although I believe that is coming because I know of a subpoena coming their way) that they created and launched the “Horse Dewormer PR campaign,” highlights of which was the famous FDA tweet and absurd Rolling Stone article:

In late 2021, Baron publicly pushed for doctors who spread “misinformation” about COVID-19 and the vaccines to lose their license and certification.
Last year, Baron partnered with Weber Shandwick to propose a South by Southwest (SXSW) panel titled “When Doctors Prescribe Misinformation.” The proposal was subsequently accepted and the panel took place at SXSW in Austin, Texas, on March 13.
According to Thacker, “Weber Shandwick’s panel featuring Dr. Baron has been widely promoted by the PR firm’s employees,” including Sarah Mahoney, executive vice president, Healthcare Communications, Strategy & Planning for Weber Shandwick, who in a LinkedIn post, wrote she “can’t think of a more important topic right now.”
Although to the unawake the following may seem normal public health practice, but to those of us fighting agency capture by Big Pharma, it is absurd:
The CDC’s National Center for Immunization and Respiratory Diseases (NCIRD) in September 2020 awarded Weber a $50 million contract “to promote the vaccination of children, pregnant women and those at risk for flu and increase the general acceptance and use of vaccines,” according to the PR firm’s website.
Thacker said he believes much of what is labeled “misinformation” in medicine and academic research “is really just corporate PR,” and that “Congress needs to take a harder look at funding for ‘misinformation research.’“
Speaking of taking a harder look at where the funding is coming from for “misinformation research” and the ABIM, it turns out that.. we can’t. Why? Check out this tweet showing a clause inserted into the ABIM’s by-laws in 1998:
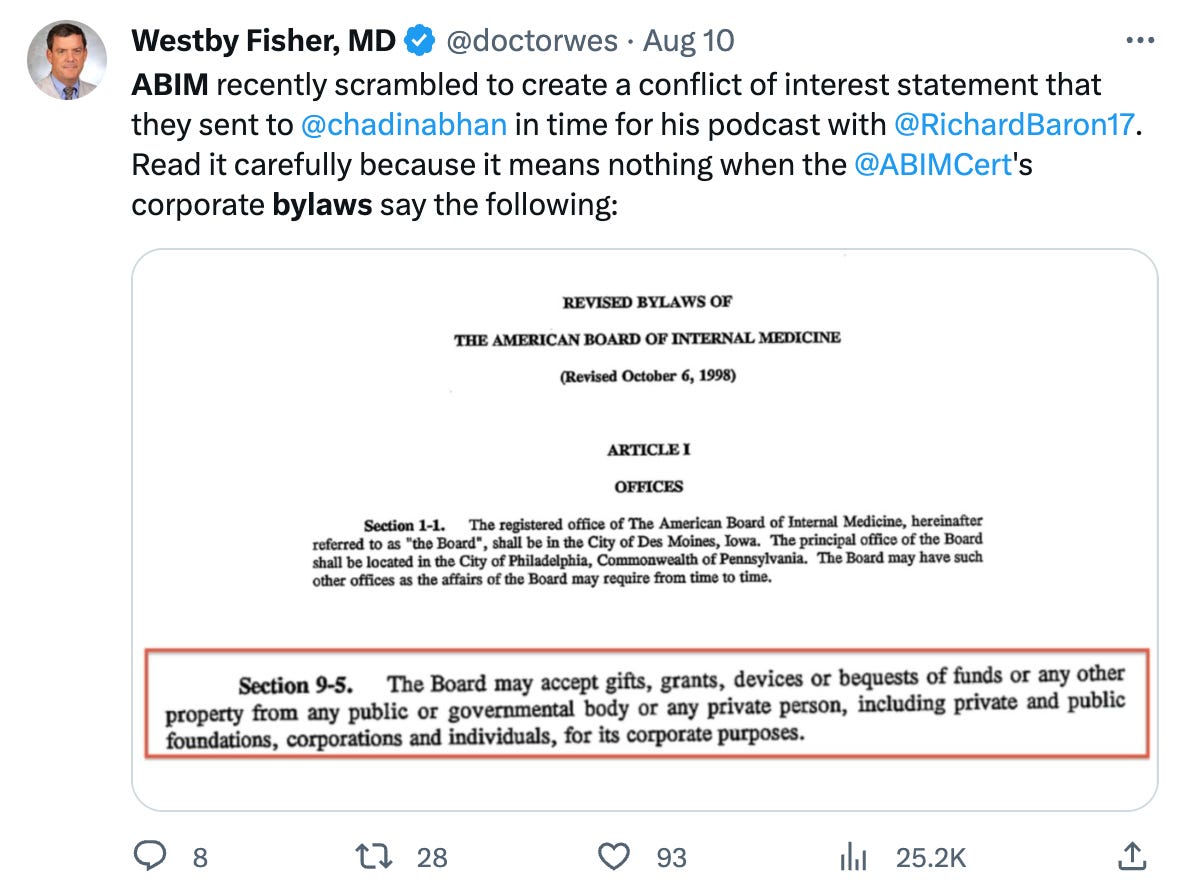
But wait, it gets better, like way better. Also in their by-laws:
Information that is disclosed will be kept confidential except to the:
President and Chair of the Board;
The chairs of the relevant Subspecialty Boards, Test-Writing Committees, and other Committees of the Board, members who serve on the relevant Boards and Committees, and staff working with the respective committees;
The Conflict of Interest Committee members and Conflict of Interest Committee staff,
except as required for the purposes of continuing medical education.
So, basically, they can take money from any corporate entity and do not have to disclose it to anyone. Again, nice gig if you can get it.
Back to the ABIM’s history: One of Eichenwalds more disturbing observations about the behavior of the ABIM:
I can attest to the ABIM's pomposity. Starting with my first story about the ABIM, the organization usually has refused to acknowledge I even asked a question. The only other group to do that in my 30-year journalism career was a company that processed payments for child pornography websites. Plus, when I reported on the uprising by doctors, the ABIM ignored the facts and instead investigated me.
Now lets fast forward to Covid. On July 29, 2021, the FSMB (this entity controls the state medical licensing boards, not the ABIM - at least on paper) issued a policy statement that “Physicians who generate and spread COVID-19 vaccine misinformation or disinformation are risking disciplinary action by state medical boards, including the suspension or revocation of their medical license.”
What is interesting is how fast and how rigidly the ABIM followed the FSMB’s lead and enacted their own misinformation policy despite the fact that, as my colleague Meryl Nass has pointed out:
“suddenly claiming that using licensed drugs for COVID, criticizing federal policies for COVID or criticizing the value of COVID vaccines is unprofessional” gives the specialty board the right to revoke a certification—well, that was never part of its contract with me. So pulling my certification for issues that were never specified in the original contract is breach of contract.
I think it would only be a breach if contracts, like our Constitution and the practice of medical ethics, were still “a thing.”
The ABIM apparently liked the FSMB’s “misinformation policy” idea to attack dissenting doctors so much (or were told to like it) that 2 months later, they, along with their colleagues at the American Board of Pediatrics and the American Board of Family Medicine, issued a statement supporting the FSMB’s position, saying, “We all look to board certified physicians to provide outstanding care and guidance; providing misinformation about a lethal disease is unethical, unprofessional and dangerous.” (note that they seem particularly focused on Covid misinformation and not any other disease model or therapeutics. Do you think it could be because Covid vaccines and therapeutics opened immensely profitable markets to Pharma overnight?).
Again from Meryl Nass (please subscribe to her Substack):
Furthermore, the processes the ABIM is using, as described by CEO Richard Baron, MD in his podcast with the New England Journal of Medicine are procedurally unfair. Dr. Baron earns $1 million/year to threaten doctors for a crime that does not exist. Baron, notably, refused to specify where the line was between misinformation and genuine disagreement in that podcast, though he seems to have no difficulty at all drawing the line when it comes to licensees who speak publicly about how to manage COVID. In a truly Orwellian effort, the ABIM and the ABIM Foundation have dedicated the year to ‘building trust’ in medicine.”
In what I suspect was the ABIM’s first enforcement of their shiny new policy, they go after Peter McCullough, Paul Marik, and myself.. on the same day (May 26, 2022) with a letter quoting numerous public statements we made, implying that we needed to defend the substance of such statements with supporting data or risk losing our certifications.
“Game on” I thought, looking forward to the exercise of “debating” scientific data with the ABIM. However, our FLCCC lawyer, Alan Dumoff pointed out that the ABIM’s policy and procedures state that the process of accusing a member of misinformation requires that they first provide evidence to us that what we said was inaccurate. So, we wrote back, pointing out to the ABIM their brazen “error” (yeah right) in not complying with their own policy and procedures.
“Nonsense” they wrote back (in short). Their logic was truly shocking - they say that the fact they provided the substance and references to my public statements means they did their duty (rather than their providing references that would refute my statements which is what their policy states they need to do).
You can read their brazen, illegitimate, dismissive response here:

This letter above demonstrates the unchecked power they have - they alone determine whether they are following their own policy which they so clearly were not. What did I say about liars before?
Anyway, rebut them we did. We wrote a 76 page treatise with 175 references, 11 exhibits, and 22,000 words, marshaling and weaving numerous data sources to support all our public statements that they had a problem with. May it enter the historical record here (I think you Covid vaccine and ivermectin data geeks will find the letter impressive).
We sent that letter over 6 months ago… and finally got an answer a few weeks ago. To understand the misinformation committee’s response, note this statement from an editorial written by Baron where he tries to give examples of misinformation:
A whole range of statements with which many — or even most —physicians might disagree would therefore not trigger our disciplinary process. On the other hand, when someone certified by the ABIM says something like “the origin of all coronary heart disease is a clearly reversible arterial scurvy” or “children can’t spread Covid” or “vaccines don’t prevent Covid deaths or hospitalizations,” we are not dealing with valid professional disagreement; we are dealing with wrong answers.
That last sentence is critical as Baron literally is saying that the ABIM gets to determine what is a valid professional disagreement versus a “wrong answer.” Good to know, especially in regards to the fact that the narrative that “vaccines prevent Covid deaths or hospitalizations” was strongly refuted in our initial response letter.
This issue about drawing a line between misinformation and genuine disagreement is a critical one. From our letter of appeal written by our lawyer Alan Dumoff:
Threshold Issue: What Standard Distinguishes Legitimate Differences of Professional Opinion and Misinformation
We disagree with the Committee’ s interpretation of the data, which we address below, but the initial question is by what standard the American Board of Internal Medicine (“ABIM” or “Board”) evaluates evidence to determine that disagreement with consensus generally, and regarding controversial matters around COVID-19 policy specifically, rise to the level of actionable misinformation. The Board’s policy recognizes the right to legitimate debate, which requires it not merely show evidence supporting a consensus view but that it demonstrate that these professional disagreements are not legitimate but outright misinformation.
If not grounded in an articulated standard, at the very least, the Board must demonstrate that the views at issue are false by citing the fallacies in the actual substance of the evidence provided, not simply by critiquing a few isolated studies divorced from the totality of evidence. Resting solely upon citations to mainstream publications while substantially avoiding the evidence in our Submission, and our detailed critiques of these publications does not provide a basis for the Board to take action against my clients.
A diplomate’s medical positions must be plainly erroneous to merit sanction. Departure from consensus is hardly unusual and by itself insufficient. While the Sanctions Notice gives the appearance of having done so, the Committee did not directly engage the numerous imperfections in the mainstream approach Drs. Kory and Marik’s have pointed to in substantial detail. The Committee has not engaged the evidence submitted and demonstrated it is illegitimate, only that it departs from the consensus, that is insufficient to support a sanction.
The point is that the ABIM appears absurdly obsessed with getting doctors to spout only consensus opinions. This is literally unprecedented in science. From Michael Chrichton the author:
I want to pause here and talk about this notion of consensus, and the rise of what has been called consensus science. I regard consensus science as an extremely pernicious development that ought to be stopped cold in its tracks. Historically, the claim of consensus has been the first refuge of scoundrels; it is a way to avoid debate by claiming that the matter is already settled. Whenever you hear the consensus of scientists agrees on something or other, reach for your wallet, because you’re being had. Let’s be clear: the work of science has nothing whatever to do with consensus. Consensus is the business of politics. Science, on the contrary, requires only one investigator who happens to be right, which means that he or she has results that are verifiable by reference to the real world. In science consensus is irrelevant. What is relevant is reproducible results. The greatest scientists in history are great precisely because they broke with the consensus. There is no such thing as consensus science. If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.
I love that last line so much it bears repeating, “If it’s consensus, it isn’t science. If it’s science, it isn’t consensus. Period.”
Now, let’s look at their response to our 76 page letter teeming with supportive data for our statements. Can read their letter in its entirety here but I thought I would just pull the most illustrative sections:
..the CCC (i.e. misinformation committee) concluded that your statements about the purported dangers of, or lack of justification for, COVID-19 vaccines are false and inaccurate because they, too, are not supported by factual, scientifically grounded, and consensus driven scientific evidence. In fact, the overwhelming body of factual, scientifically grounded, and consensus-driven evidence – at and since the time you made those statements – shows that the COVID-19 vaccines are safe and effective for children and for adults
I have heard of the term “evidence-based medicine (EBM)” which is what I practice, but not “consensus driven science” (completely new invention - pernicious indeed). I actually adhere to the original definition and conceptual framework envisioned by the founders of evidence based medicine which was incredibly well detailed by my friend “A Midwestern Doctor” in their brilliant recent post “What Happens To Doctors Who Innovate”.
Anyway, they then listed a few published, peer-reviewed papers supporting their point, blissfully un-acknowledging of the fact that the high-impact journals have been systematically censoring pretty much all negative analyses of the vaccine campaign’s impacts while publishing nothing but positive reports with cherry-picked and/or fraudulent data - so there is no way for the truth about vaccines to win in scientific debates my friends.
The high-impact journal censoring of adverse vaccine data is identical to their censoring of dozens of positive trials of ivermectin, something I extensively detail in the chapter called “The Journal Rejections of Positive Ivermectin Studies” in my book.
It gets even better - they next argue against my claims of lack of safety of the vaccines by, get this, referencing proclamations by the WHO and CDC. They ignore all the immense data to the contrary that I submitted while of course being willfully oblivious to the fact that the CDC and WHO are fully Pharma captured agencies:
Moreover, the vaccine safety data overwhelmingly (overwhelmingly?) contradicts your statements about vaccine risks. See, e.g., Centers for Disease Control and Prevention, “Safety of COVID-19 Vaccines,” https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/safety-of-vaccines.html (updated March 7, 2023) (reporting that “Adverse Events (Serious Safety Problems) Are Rare,” and that “[t]he benefits of COVID-19 vaccination outweigh the known and potential risks”); World Health Organization, “Safety of COVID-19 Vaccines,” https://www.who.int/news-room/feature-stories/detail/safety-of-covid-19-vaccines (March 31, 2021) (stating that “[b]illions of people have been safely vaccinated against COVID-19,” that “mRNA vaccines [for COVID-19] have been rigorously assessed for safety, and clinical trials have shown that they provide a long-lasting immune response”).
The paragraph above should enter the historical record.. somewhere. That will NOT age well. The only thing more absurd to contemplate is whether they know they are lying in their letter or if they are simply referencing propaganda that they themselves swallowed whole? In a way, the former might be more acceptable to me at this point.
Their opinion on how I got ivermectin wrong was similarly brazen - they ignored all the meta-analyses (historically considered the strongest form of data, a fact they seem to have willfully avoided) in favor of listing a handful of trials where ivermectin was supposedly found ineffective, relying mostly on citing “the Big 6” (what I named the chapter describing the fraud behind the 6 largest, Pharma-conflicted and most publicized trials on ivermectin). This was 100% unsurprising.
Check it out:
First, the CCC concluded that your statements about the safety and efficacy of ivermectin and hydroxychloroquine as treatments for COVID-19 are false and inaccurate because they are not supported by factual, scientifically grounded, and consensus driven scientific evidence (there it is again).
Susanna Naggie, M.D., M.H.S., et al., “Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19,” 328 JAMA 1721 (2022), https://www.nejm.org/doi/full/10.1056/nejmoa2115869 (finding in a double-blind, randomized, placebo-controlled study with 1,800 participants that “[a]mong outpatients with mild to moderate COVID-19, treatment with ivermectin, compared with placebo, did not significantly improve time to recovery,” and that “[t]hese findings do not support the use of ivermectin in patients with mild to moderate COVID-19”);
I laughed out loud when they led their argument with the Naggie trial funded by the NIH as it contained the most brazen fraud of the Big 6 Pharma Ivermectin trials. All you need to know about the trial is that they moved the primary comparison endpoint of the trial.. in the middle of the trial. They moved the main comparison from symptoms at Day 14 to Day 28. Note that changing endpoints in the middle of a trial is a supposed never event. Except the same trick was pulled in the Remdesivir trial.
Anyway, in a presentation by Naggie, in this secondary endpoint, you can see that ivermectin was superior at Day 14 to a high degree of Bayesian “statistical significance” but the “statistical significance” was not reached at Day 28 (I use quotes around statistical significance because it is an erroneous concept when doing Bayesian statistics but that is what they did anyway when they pre-specified a threshold of above 0.95 as “significant”). Can anyone tell me why they moved the endpoint to Day 28 in the middle of the trial:
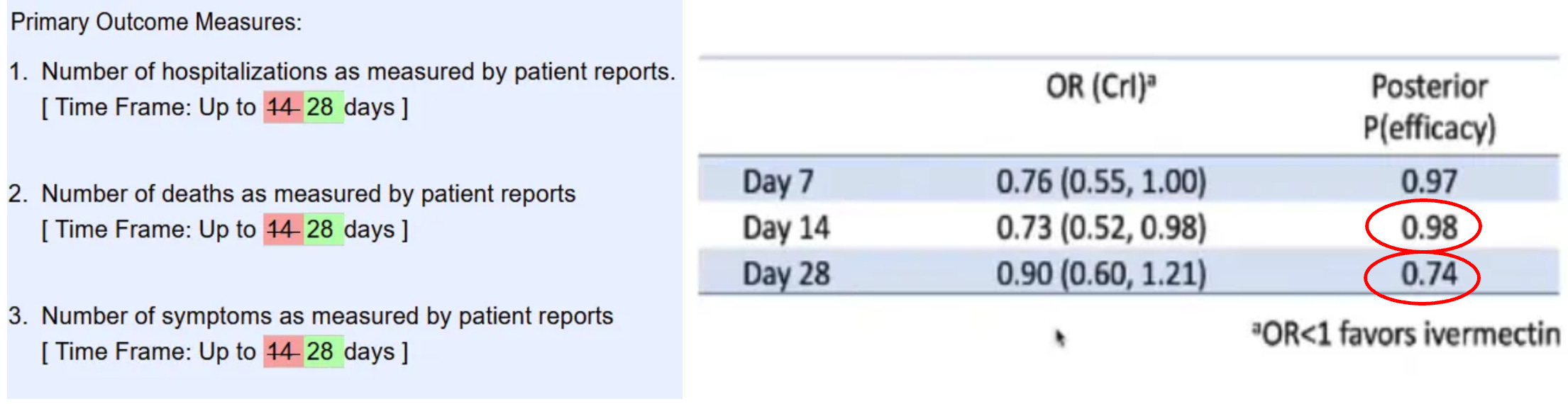
With this brazen maneuver (and many others) it allowed Naggie et al to publish this conclusion: “these findings do not support the use of ivermectin in patients with mild to moderate COVID-19.” Not-so-fun fact: Naggie also sat on the NIH covid treatment guidelines committee where she voted to not recommend ivermectin right before she and her University received tens of millions.. to study ivermectin in Covid. You want more? She also owns stock in a competitor to ivermectin (monoclonal antibodies for Omicron) and has received money from numerous other Big Pharma companies including Gilead. Lets get back to the letter…
Rather, the CCC seeks to accomplish precisely what you assert ABIM should be doing: seeking to “further the professional integrity of medicine by encouraging evidence-based debate” (emphasis added).
Indeed, as set forth in ABIM’s False or Inaccurate Medical Information policy, physicians have an ethical and professional responsibility to provide factual, scientifically grounded, and consensus driven scientific evidence (there it is again). As discussed above, by touting the effectiveness of ivermectin and hydroxychloroquine as COVID-19 treatments and casting doubt on the efficacy and safety of COVID-19 vaccines with such seemingly authoritative statements, you have made statements that are inimical to ABIM’s ethics and professionalism standards for board certification.
In light of all the evidence and circumstances, the CCC determined to recommend that your board certification be revoked.
There is only one silver lining here. One - the impending loss of my certifications does not affect me materially because I have a private fee-based practice due to my need for complete autonomy and lack of restrictions in empirically treating the vaccine injured with various repurposed and alternative therapeutics. I thus cannot and will not accept insurance, and secondly, my academic career is over - no longer will I ever enter back into the system of medicine.
About the only opportunity this whole attack has created is one where I get to defend myself on appeal in a debate with three academic white coats of their choosing. Bring. It. On.
Although the outcome of the debate is assuredly pre-determined, I know it will satisfy a deep yearning many of us dissidents have had for going on 3 years now - to debate someone, anyone, anywhere. Crush them with data. Make ‘em look silly although I will be the only one who knows it happened. It will let me vent my disgust at how they have widely disseminated corrupted scientific evidence and policies while simultaneously ignoring the clinical observations and expertise of frontline doctors who have treated thousands of actual Covid patients.
I will then toss in a little lecture about how RCT’s have long ceased to be a credible means of proving anything in science given that in modern medicine only “Big RCT’s” count and that all “Big RCT’s” require such massive funding that the bias of the funders outweighs any objectivity such trials can profess to attain. I will also remind them that throughout modern medial history, the findings of RCT’s and retrospective observational trials are identical, yet academia has been taught to systematically ignore observational trials. Reason: only massively funded entities can conduct a “Big RCT” while any committed clinician willing to give up nights and weekends can conduct an observational trial. Pharma cannot allow research to be conducted that they have no control over - so they took over the journals and medical school curriculums which now literally teach that observational controlled trials can only be considered “hypothesis generating” and thus their results should not be acted on. Nonsense.
I will also remind them that they are violating international law and human, civil, and political rights as argued by Meryl Nass in another of her excellent posts regarding her own persecution by her state licensing Board:
International law is on our side. A total of 172 countries are parties to the International Covenant on Civil and Political Rights:
According to the 1948 Universal Declaration of Human Rights, Article 19,
"Everyone has the right to freedom of opinion and expression; this right includes freedom to hold opinions without interference and to seek, receive and impart information and ideas through any media and regardless of frontiers."
According to the 1966 International Covenant on Civil and Political Rights,
"Everyone shall have the right to freedom of expression; this right shall include freedom to seek, receive and impart information and ideas of all kinds, regardless of frontiers, either orally, in writing or in print, in the form of art, or through any other media of his choice.”
And the Nebraska Attorney General protected doctors and pharmacists in Nebraska from their Boards, explicitly allowing them to prescribe HCQ and IVM. His opinion is a tour de force, which goes into detail about why the CDC, FDA and NIH guidelines are contradictory, unscientific and should not be followed. It should be cited in every case.
I also plan on reminding them that the FDA got its ass handed to them in court last week during a hearing of Paul Marik, Mary Tally Bowden and Robert Apter’s suit against the FDA. From an Epoch Times article on the hearing:
“FDA explicitly recognizes that doctors do have the authority to prescribe ivermectin to treat COVID,” Ashley Cheung Honold, a Department of Justice lawyer representing the FDA, said during oral arguments on Aug. 8 in the U.S. Court of Appeals for the 5th Circuit.
The statements “don’t prohibit doctors from prescribing ivermectin to treat COVID or for any other purpose” Ms. Honold said.
“FDA is clearly acknowledging that doctors have the authority to prescribe human ivermectin to treat COVID. So they are not interfering with the authority of doctors to prescribe drugs or to practice medicine,” she said.
So, if the FDA recognizes we have the authority to prescribe ivermectin, then assuredly we are allowed to have the opinion that it is a valid therapy. However, the ABIM will not allow an ABIM certified physician to publicly express this opinion or recommend this practice. Maybe the ABIM should have a little chat with the FDA?
The nonsense doesn’t end with the ABIM, as they are only one prong of this campaign. How is this for some comic relief, published last week in one of the top journals in the world where they found that almost all the Covid misinformation in the U.S on social media can be traced to 52 doctors.

I was honored to discover that yours truly made the list! In their quoted examples of misinformation in Table 4, I have taken the liberty of owning up to the posts attributed to me, all of which I stand by to this day:
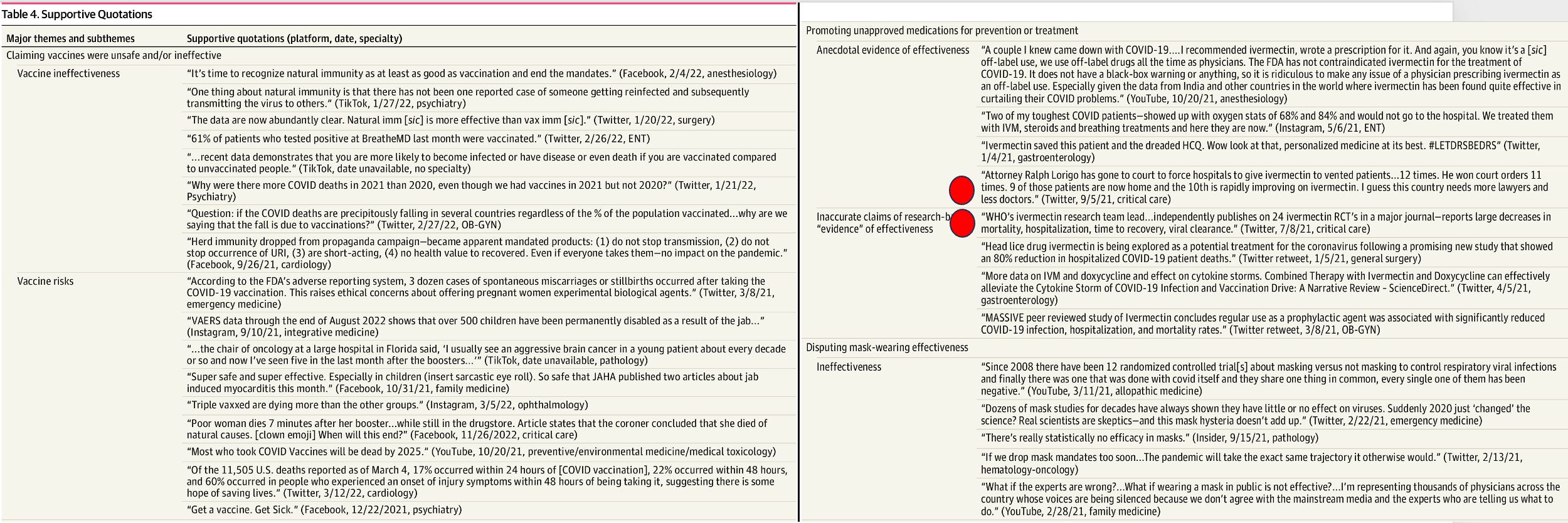
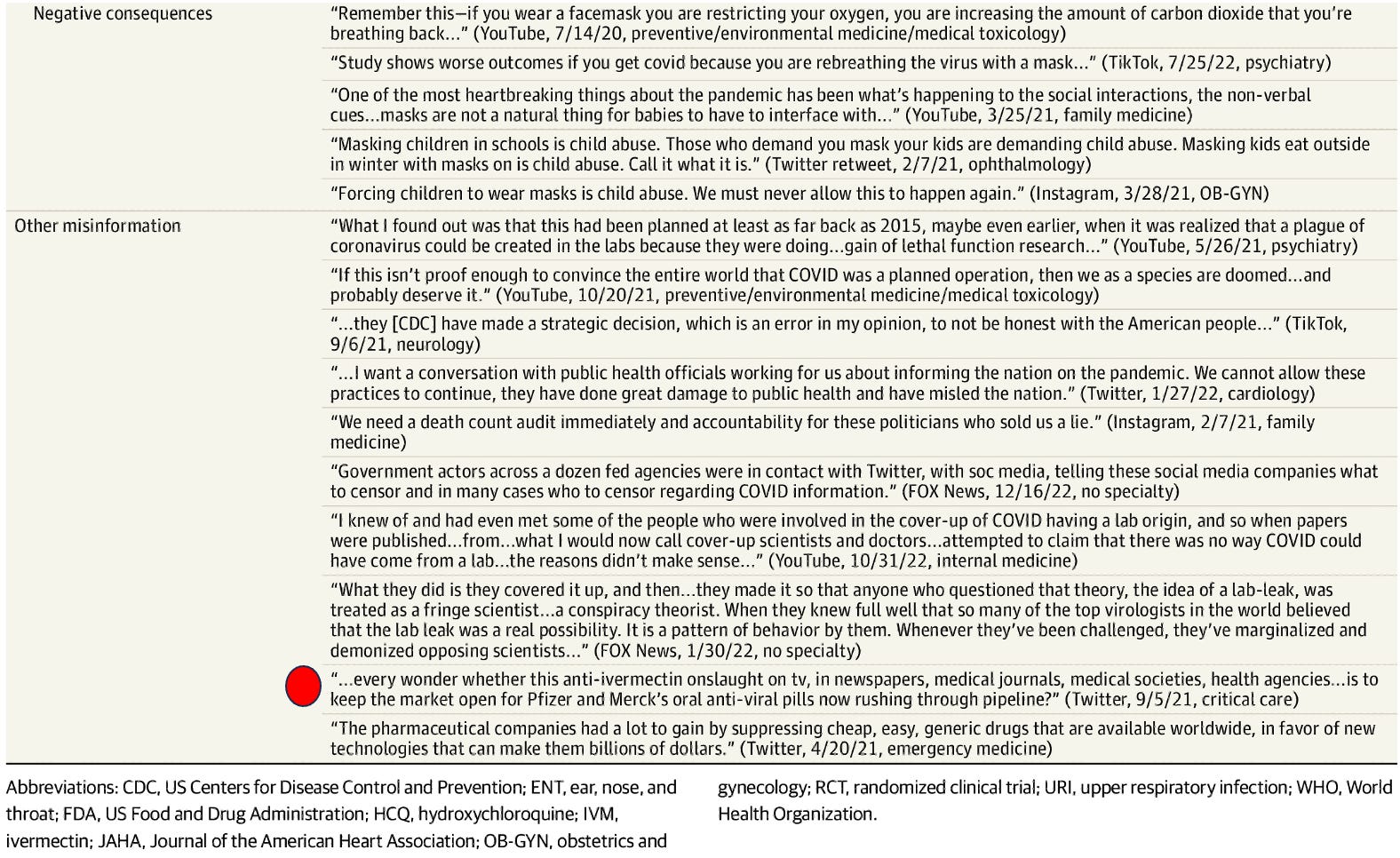
The comic relief of this article comes from the fact that the authors decided that what constituted mis-information in Covid were the beliefs that:
The virus was concocted in a lab (true), natural immunity is equal or better than vaccine immunity (true), ivermectin and hydroxychloroquine are effective (true), the vaccines are ineffective, toxic and lethal (true, true, and true), that federal agencies were working directly in the service of Pharma (true) etc. I hope we never forget this absurdity of a peer-review paper.
I think I will finish with this excerpt from a recent Wall Street Journal Op-Ed touching on the Missouri vs. Biden case where the administration is being sued for its systematic censoring of U.S citizens on social media by every intelligence and health agency in our Federal government :
This is where the decision of U.S. District Judge Terry Doughty sheds light. His detailed recounting shows a Washington energetic in protecting Americans from Covid opinions, expertise and claims that conflicted with its own, at a time when it served politicians to show they were trying to save Americans from encountering a virus that couldn’t be avoided. When government has a message to deliver, especially when the political stakes are high, it won’t be content just to push its own message, it will try to silence others. Fighting back will always be necessary. The only surprise in our age is how thoroughly the “liberal” position has become the pro-censorship position (that last line is a doozy).
P.S I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amount of time I spend researching and writing my posts, so again, thanks. - Pierre
P.P.S - Proud to report that my book is gaining Best Seller status on Amazon in several countries and is climbing up the U.S Amazon rankings… Link:

My Board Certification with ABEM will end in 2025. In their eyes, that will end 30 years of Board Certification, but I don’t work in an Emergency Department anymore and made my decision not to recertify after they sent us out a “warning” email about “misinformation and disinformation” on Covid 19 and how it could cause us to lose our ABEM certification, I responded with a 4 1/2 page certified letter to the members of the Board which ended with the promise that if I found out they had done this to any of my colleagues, I would contact that person and help them sue ABEM. Do they really think they can take away my 4 year residency, oral and written Boards and repeat written Boards? Do they really think my 30 years of knowledge and experience will suddenly dissipate into the air because they said so? And don’t get me wrong. For the first 18 years, I lived and breathed Emergency Medicine. I was on a state Board of Directors for 10 years. I was on the ACEP Council for 18 years. When I was a resident, I was the Speaker of the Resident Council. I was on National and State Committees. I eventually left and owned an Urgent Care. I loved what I did. But I am not their whore. I will not pay them and play their little game while they and ACEP gaslight us so they can keep their Lobbyist office in D.C. and collect dues from over 40,000 Emergency Physicians. When Covid was raging, I prescribed Ivermectin and Budesonide Inhaled treatments. I took it myself when I had Covid. I haven’t suffered a fraction of what Dr. Kory and others have suffered in their careers, but this whole episode in our history has changed me forever. I currently practice Addiction Medicine.However, I believe this will eventually turn around. There’s too many studies all over the world, too many people who originally drank the lemonade that are now questioning, and too many vaccine injured patients. I think eventually Dr. Kory, Dr. Marik and McCullough, along with countless others, will be vindicated when these “certifying bodies” start to back pedal on advice of legal counsel.
“Bring. It. On.”
😎💪🍿👊
You are such a badass, Pierre. Love it.
I’m beginning to think licensing and certifications need to become extinct as they are merely used as a way of enforcing ideological and pharmaceutical conformity. Just as being smeared by the mainsleeze media is now a badge of honor (https://margaretannaalice.substack.com/p/letter-to-a-mainstream-straddler), so is losing your license/certification for independent, evidence-based critical thinking that exposes the lies masquerading as The $cience™.
Not that you need any more ammunition, but feel free to pilfer as desired from my letter about AB2098 and another challenging the thought-policing of public health and the religion of astroturfed “scientific consensus”:
• “Letter to the California Legislature” (https://margaretannaalice.substack.com/p/letter-to-the-california-legislature)
• “Letter to US Legislators: #DefundTheThoughtPolice” (https://margaretannaalice.substack.com/p/letter-to-us-legislators-defundthethoughtpolice)