

Shedding of Covid mRNA Vaccine Products - A Review Of The Scientific, Regulatory, and Clinical Evidence
Shedding of Covid mRNA Vaccine Products - A Review Of The Scientific, Regulatory, and Clinical Evidence
In collaboration with A Midwestern Doctor, we compiled all of the scientific, regulatory, and clinical evidence that mRNA vaccine recipients can cause symptoms in others via shedding of spike protein.


This version has been updated to include a “Table of Contents” which allows a direct link to the topic of interest.
INTRODUCTION: A CALL FOR STOPPING THE MRNA VACCINE CAMPAIGN
PUBLISHED EVIDENCE SUPPORTING SHEDDING PHENOMENA
3a. Evidence For Shedding Via Breast Milk
SUMMARY OBSERVATIONS OF OVER 1000 CLINICAL REPORTS OF SHEDDING
4b. Susceptibility to Shedding
4c. Characteristics of Shedders
4i. Rarer Symptoms
5b. Sexual Partners
5c. Blood Supply
INTRODUCTION: A CALL FOR STOPPING THE MRNA VACCINE CAMPAIGN
This document provides evidence from regulatory documents, a review of the scientific literature of nanoparticle and gene therapy technology, published clinical studies and reports, and over 1000 compiled clinical case testimonials, many of which support the reality that clinically significant shedding of spike protein from the vaccinated to others is occurring.
We believe this knowledge — that mRNA vaccine shedding is occurring — may be the most powerful means by which the mRNA vaccine booster program is stopped, given it is clear that shedding is far more common after a booster rollout. If the mRNA vaccine program is not stopped, it is likely facilities may follow in the footsteps of the Miami private school which, in 2021, prohibited students from attending the school within 30 days of vaccination.
We believe one of the best strategies going forward is to actively petition for a federal law to be passed mandating that for a gene therapy product to enter the market it must:
1) Have studies conducted that properly evaluate all potential routes of shedding for any gene therapy product (making it illegal to ignore current FDA guidance on gene therapy products);
2) Have the studies be made available to the public as well as to the potential recipients, given the therapy can affect the general population and thus violates the principles of informed consent and bodily autonomy;
3) Have clear guidance for those who receive the product so they can protect others from being shed upon (e.g., Roctavian sheds in the semen for six months, and as a result its recipients are instructed not to donate semen or impregnate someone for six months);
4) Have the product be pulled from the market if outside investigators discover the manufacturer’s data was wrong and the product does indeed shed, or it is discovered that recipients are not following the measures necessary to mitigate the gene therapy’s shedding.
Support in the form of paid subscriptions is greatly appreciated and will help further support the large amounts of time I have put and will continue to put into this research.
REGULATORY PRECEDENT AND DEFINITIONS
It first must be recognized that COVID mRNA “vaccines” are gene therapy products as defined in the FDA’s 2015 document on Gene Product Shedding Studies and by a similar European Medicines Agency (EMA) document:
“Gene therapy products are all products that mediate their effects by transcription and/or translation of transferred genetic material and/or by integrating into the host genome and that are administered as nucleic acids, viruses, or genetically engineered microorganisms.
The FDA document defines shedding of gene therapy products as:
“The release of viral or bacterial gene therapy products from the patient by any or all of the following routes: feces (feces); secretions (urine, saliva, nasopharyngeal fluids, etc.); or through the skin (pustules, lesions, sores).”
The FDA document also recommends shedding studies be done for all gene therapy products in both humans and animals.
It is well known that gene therapy products have a risk of shedding given that for the first ever approved gene therapy product, called Luxturna, the manufacturer warns in their insert below:

Other approved gene therapy products have also been found to shed. Roctavian was found to shed into semen and the FDA advises those who receive it to not donate semen or impregnate someone for at least 6 months after administration.
Another gene therapy product called Zolgensma was also found to shed for a month, and its package insert advises that during this time, to be careful of how feces from the patients are disposed of to avoid exposure to others.
Finally, Pfizer knew, or at least considered, that shedding was a possibility with its COVID mRNA product, given that they specifically excluded people “exposed” to the vaccine via inhalation or skin contact. Starting on p. 67 of its protocol, the investigator is instructed to report various "environmental exposures" as follows:
1) “A male participant who is receiving or has discontinued study intervention exposes a female partner prior to or around the time of conception."
2) “A female family member or healthcare provider reports that she is pregnant after having been exposed to the study intervention by inhalation or skin contact."
3) "A male family member or healthcare provider who has been exposed to the study intervention by inhalation or skin contact then exposes his female partner prior to or around the time of conception" (note this refers to “secondary shedding” as defined later in the document)
4) "A female is found to be breastfeeding while being exposed or having been exposed to study intervention (i.e., environmental exposure). An example of environmental exposure during breastfeeding is a female family member or healthcare provider who reports that she is breastfeeding after having been exposed to the study intervention by inhalation or skin contact."
In a review paper on shedding, the author concludes: This clearly means that any contact, including sexual contact with someone who has received the vaccines, exposes those who have not received the vaccines to the “intervention”, i.e. mRNA [or its gene therapy product].
Shedding Via Nanoparticles
With regard to COVID vaccines, the “products” that are at risk of being shed from one person to another are 1) the synthetic vaccine spike protein 2) lipid nanoparticles, 3) naked mRNA, 4) polyethlene glycol (PEG) or 5) suspected contaminants (DNA plasmids).
More important than the fact that COVID mRNA vaccines are gene therapies, they are also categorized as “nanoparticle technology” given that the mRNA is delivered to the cell within lipid nanoparticle (LNPs).
Nanoparticles exist in both natural, biological forms (called exosomes) as well as synthetic ones such as the LNP of the mRNA vaccines. Importantly, synthetic mRNA vaccine LNPs have the same structure as the natural exosomes they seek to mimic.
Exosomes are tiny extracellular vesicles of endosomal origin, typically 30-150 nm in diameter, containing a complex cargo of contents derived from the original cell, including proteins, lipids, mRNA, miRNA, and DNA. They are formed through the fusion and exocytosis of multivesicular bodies into the extracellular space. Exosomes are constantly produced by all cells in vitro and in vivo, and are changing research due to their interesting functions within the human body, including inter-cellular communication and signaling.
Exosomes form a critical communication network the body relies upon (e.g., mothers have exosomes in their breastmilk, which make it through the digestive tract and deliver mRNA to their developing babies playing a critical epigenetic role in guiding their healthy development).
As a gene therapy, the mRNA vaccines work by delivering mRNA within synthetic LNPs into the cell, which instructs the cell to make spike protein. The spike protein is then pushed to the cell surface at which point they bud off into exosomes that traverse the body.
Exosomes are defined as biological nanostructures of 40–150 nm in size while the LNPs in the mRNA vaccines range from 100-400 nm in size. The smaller the size of an LNP or exosome, the more widely they distribute and the more easily they can both exit and enter the body.
A critically important aspect of exosomes and LNPs is that they can cross the biological barriers shielding various parts of the human body, such as the blood-testes barrier and enter the testes in animal models. Another review paper stated: "these ultrafine particles are capable of entering the body through skin pores, debilitated tissues, injection, olfactory, respiratory and intestinal tracts.”
MECHANISMS OF MRNA VACCINE SHEDDING
Evidence Supporting the Mechanisms of Shedding
It is our opinion that shedding occurs primarily by the emission of spike-containing exosomes within exhaled breath. Other mechanisms are possible, such as DNA plasmid integrating into the microbiome and then shedding via the breath, SARS-CoV2 persistence in the vaccinated and then shed (either directly or via parts of the virus in exosomes), altered pheromones in vaccinated individuals that affect those around them, or LNP breakdown and shedding of PEG. However, a discussion of the validity of these alternate hypotheses lies beyond the scope of this document. For an exploration of these, see this article by A Midwestern Doctor.
To prove the validity of spike exosome shedding of the mRNA nanoparticle gene therapy vaccines, supportive evidence for the following three mechanistic conditions is required along with clinical evidence of the development of typical vaccine adverse effects arising in those exposed to the vaccinated.
Condition #1: The produced spike protein would need to distribute widely in the body in order to allow excretion via the breath, urine, sweat, breast milk, feces etc.
Condition #2: The spike protein would need to establish sufficient concentration in body fluids or exhaled breath.
*Some question whether the concentration of spike protein then excreted could ever be sufficient enough to make someone develop adverse symptoms, especially if the vaccinee is not themselves symptomatic. Based on the countless and highly detailed descriptions of shedding events we have compiled here, it is clear that only a minority of the population is “environmentally sensitive” enough to experience adverse effects from exposure to the vaccinated and thus the concentration of exhaled exosomes is likely only sufficient enough to make a small subset of exposed people symptomatic.
Condition #3: LNPs and/or spike protein-containing exosomes must be able to enter the body of an exposed person either through inhaled breath, skin, or eyes. If pregnant, LNP/exosomes would need to have the ability to cross the placenta. For breastfeeding women, LNP’s, free spike protein or mRNA would need to be found in breast milk and evidence of intact absorption of exosomes be demonstrated in babies.
Clinical Evidence: If scientific support for conditions 1, 2, 3 are present, then evidence is needed to show that typical vaccine adverse event symptoms develop in unvaccinated people (or even previously vaccinated) people after close exposure to a vaccinated person.
Shedding Condition #1: The produced spike protein would need to distribute widely in the body in order to allow excretion via the lungs, urine, sweat, breast milk, feces, etc.
Evidence:
1) Synthetic LNPs containing vaccine mRNA are distributed widely in the body as per this recently leaked EMA letter.
2) A Japanese document obtained by FOIA reported on the lipid nanoparticle biodistribution data for Pfizer’s vaccines and found the LNPs distribute to every organ in the body.
3) Australia’s Therapeutics Goods Administrations (TGA) evaluation report on Pfizer’s nonclinical biodistribution study also revealed that the lipid nanoparticles travel to the liver, spleen, brain, eyes, bone marrow, adrenal glands, ovaries, and testes.
Shedding Condition #2: The spike protein would need to be present in exosomes in sufficient quantities in body fluids or exhaled breath. For pregnant women, spike protein would need to be found in breast milk.
Evidence:
The spike protein has a high (heparin dependent) affinity for binding to the surface of exosomes and numerous studies find that significant amounts of spike protein containing exosomes (which circulate in the bloodstream) increase rapidly after vaccination (and then decline). Other papers from 2013, 2020 and 2021 show that significant amounts of RNA containing exosomes can be found in breath.
Another study found vaccine mRNA persists in the bloodstream for at least two weeks after injection. The authors state that it likely retains its ability to induce S-protein expression in susceptible cells and tissues. Note this is much longer than was claimed by the manufacturers on the basis of brief studies in rats.
Numerous studies have found that vaccination with mRNA and translation of the mRNA induces the production of exosomes carrying the spike protein and circulating in the blood for a diverse range of durations (more than a week, up to 15 days up to 4 months, and up to 187 days [the study ended so the maximal duration has not yet been established]). After COVID infection, one study found spike protein-containing exosomes persist for up to one year later.
Long COVID and Long Vax syndrome patients (as well as more severe acute COVID patients) reveal the presence of spike protein-studded exosomes (see this paper and this paper). Additionally, they also showed exosomes from COVID patients are highly inflammatory (and potentially clot forming) and are taken up by lung cells.
Evidence for the biologic activity of spike protein-coated exosomes can be found in this study, which found that after COVID infection, spike protein-coated exosomes trigger an immune response in lung cells exposed to the exosomes.
A table from this paper on spikeopathy summarizes some of the studies showing persistence of spike protein and other vaccine components as below:

Clinical and pathologic evidence are available as well: a case report of an autopsy done in a man who died of multifocal necrotizing encephalitis three weeks after the vaccine found vaccine spike in numerous organs (heart, brain, muscles, germinal centers etc.). Further, they emphasized the finding of high concentrations in the walls of capillaries.
Finally, a team led by the esteemed senior German pathologist, Arne Burkhart, stained autopsy specimens for the presence of spike protein. He presented their findings in multiple invited lectures and reported that out of the first 50 autopsies performed at the request of families who suspected their loved one’s death was due to the vaccine, in 80% of cases spike-induced organ damage was determined to be the proximate cause of death.
A more recently published autopsy review reported 28 cases of vaccine-induced myocarditis and in cases where staining for spike protein was performed, spike was detected in the foci of inflammation in the heart and brain.
Shedding Condition #3: Spike protein containing exosomes must be able to enter the body through inhaled breath, or eyes. If pregnant, exosomes would need to have the ability to cross the placenta. For breastfeeding women, spike protein or mRNA would need to be found in breast milk and be able to be absorbed via the baby’s GI tract.
This review of nanoparticles (states that they can enter the body through inhalation, ingestion, skin uptake, injection, or implantation.
In support of the above, therapeutic nanoparticles have been successfully administered: transcutaneously (here, here, here). transdermally, transfollicularly, intranasally, via inhalation and then excreted via urine, feces, saliva, breast milk, breath, and sweat. An important point to note is that there is although LNP’s can be absorbed via the skin, there is insufficient evidence to support transcuateous absorption of exosomes.
Thus, the inhalation route presents the highest risk of absorbing shed gene therapy-based vaccine products. The findings in this paper from 2005 states that:
“When inhaled, specific sizes of nanoparticles (LNP’s/exosomes) are efficiently deposited by diffusional mechanisms in all regions of the respiratory tract. The small size facilitates uptake into cells and transcytose across epithelial and endothelial cells into the blood and lymph circulation to reach potentially sensitive target sites such as bone marrow, lymph nodes, spleen, and heart.”
This randomized, double-blind controlled trial in The Lancet found that in humans, liposomal DNA gene therapy-loaded nanoparticles administered locally by nebulization transfected airway cells. This was validated by the fact that cystic fibrosis patients treated in this manner experienced a stabilization of lung function, while the placebo group experienced a decline.
Clinical trials for influenza prevention have shown the efficacy and safety of inhaled mRNA LNP vaccines. This study reported three clinical trials that used aerosol as the route of administration. In 2022, this study showed that exosomes were effective via nebulization therapy in COVID-19 patients.
An inhaled vaccine was made from lung-derived exosomes coated with spike proteins (they were lung-derived so the lung cells would be more likely to absorb them). These spike protein exosomes both generated an immune response and were absorbed into the body. Once absorbed, those exosomes then traveled to other tissues and organs in the body that are known to be affected by shedding (note this comports with the clinical reports we’ve received and the patients we’ve evaluated and treated).
Lastly, a 2023 peer-reviewed study found that unvaccinated individuals who were around COVID-19 vaccinated individuals developed an immune response to the spike protein.
PUBLISHED EVIDENCE SUPPORTING SHEDDING PHENOMENA
Here we document typical COVID mRNA vaccine adverse event symptoms in unvaccinated people after exposure to COVID mRNA vaccinated people.
Evidence For Shedding Via Breast Milk
This study found that the vaccine mRNA was found in the milk of 1/10 women studied (4/40) in the first week after vaccination with mRNA vaccine (either after dose 1 or dose 2). Amounts can reach 2 ng/mL of milk.
This study in the Lancet reported on the breast milk of 11 women who were vaccinated with mRNA within six months of delivery. They found trace amounts of mRNA in 7 samples from 5 different participants at various times up to 48 hours post vaccination. The vaccine mRNA appeared in higher concentrations in the extracellular vesicles (i.e. exosomes/nanoparticles) than in whole milk. Their conclusion:
“Our findings demonstrate that the COVID-19 vaccine mRNA is not confined to the injection site but spreads systemically and is packaged into breast milk extracellular vesicles.”
Another study found PEG (a component of the mRNA vaccine) as well as COVID vaccine mRNA in breast milk. The authors write “Of note, PEGylated proteins concentration is higher in mRNA-1273 compared to BNT-162b2 which also stand in line with mRNA concentration in each vaccine (ready for administration vaccines were used).” So, a dose-response relationship was found which is particularly damning — the more you give, the more you find in breast milk).
So, we know mRNA can be transmitted (shed) to breastfed babies in breast milk. We initially dismissed the importance of this finding by reasoning that the stomach acid of the baby would destroy the mRNA and render it inert. But then we found these papers (here, here, and here), which stated:
“It has been known for some years that mRNA encapsulated in extracellular vesicles is protected from gastric juices and can transfect intestinal cells. A recent review by Melnik and Schmitz confirms that milk EVs survive the extreme conditions of the gastrointestinal tract, are internalized by endocytosis, are bioavailable, reach the bloodstream, and penetrate peripheral tissue cells. Beyond integration into the genome, other concerns should arise such as provoking an “immunogenic” reaction to mRNA.”
Clinical evidence suggesting that the mRNA and/or spike in breast milk can survive in the stomach and cause illness in the baby lies in the below list from an eight-page confidential document of reports made to Pfizer by lactating women who were vaccinated. Pfizer was aware of and tracking adverse events in babies “exposed” to the mother’s vaccination via breast milk.
Pfizer observed what was graded as non-severe adverse events (AEs) in a shocking 20% of the 215 lactating women reporting “exposure” to the vaccine.
The report also documents 10 serious AEs, including facial paralysis (not listed under “serious” interestingly), lymphadenopathy (swelling of lymph nodes that could be associated with cancer), and blurred vision. Note these are all side effects of the vaccines reported by adults. Among infants, reports included skin exfoliation, rashes, swollen skin, and unspecified sickness. That is a very high percentage of serious AEs in babies for any therapy.
Again from the article by investigative reporter Sonia Elijah, she reports on data obtained from a Freedom of Information Act request for the EU’s Periodic Safety Update Report #3 (PSUR #3), covering the 6-month period of 19 December 2021 through to 18 June 2022, which recently became available on the Austrian Politics and Science blog, tkp. She discovered that Pfizer documented numerous cases of strokes, convulsions, and respiratory failure among nursing babies.
It is important to note that upon further review of PSUR #1, something extremely disturbing surfaced – adverse events were reported for breast-fed babies indirectly exposed to the Pfizer-BioNTech mRNA shot by their vaccinated mothers. The screenshot below is taken from page 165 of PSUR #1.
The fact that two cases from the post-marketing (PM) data involved babies who were indirectly exposed to the Pfizer-BioNTech mRNA vaccine (BNT162b2) via the trans-mammary route (through the breast milk) and consequently suffered a stroke (central nervous system haemorrhages and cerebrovascular accidents) is shocking.
Then, on page 149 (screenshot below), three more cases of babies suffering from neurological adverse events, for example, convulsions, from being indirectly exposed to the vaccine via their vaccinated mothers’ breast milk, were recorded.

From the analysis of booster doses (> 2 dose primary series), a staggering 455 cases were recorded during the 6-month reporting interval (1 from the clinical trial data and 454 recorded from the post-marketing data) and involved babies whose cases “were excluded due to indirect exposure (transplacental/transmammary) to BNT162b2.”
The document also reports four cases (babies) suffering from respiratory adverse events of special interest (AESI), which were “determined to be non-contributory and were not included in the discussion since these cases involved exposures to the vaccine during the mother’s pregnancy or through breastfeeding.”
The above are clear admissions that babies can be “indirectly exposed,” i.e., evidence that shedding between mother and baby occurs.
Given the gravity of this important safety signal affecting nursing babies, to brush over the fact that these infants’ adverse event cases were non-contributory because they were indirectly exposed to the vaccine via breast milk is unconscionable.
More evidence: A study published a year ago in JAMA revealed that 3.5% of women reported a decrease in breast milk supply and 1.2% reported “issues with their breastmilk-fed infant after vaccination.” Here is one vivid VAERS entry, which could represent spike or the LNP in breast milk:

Elijah did a more recent investigative report on Pfizer’s Pregnancy and Lactation Review which had just been released in April per court order by the FDA, two years after it was signed off. She again found reports of similar damning adverse events, such as spontaneous abortions and preterm delivery of fetuses after exposure to the vaccine trans-placentally or trans-mammary (through the breast milk) after their mothers were vaccinated. Adverse events such as facial paralysis and lymphadenopathy were also reported in infants, indirectly exposed through the breast milk of their vaccinated mothers.
Evidence For Shedding Transplacentally
Animal studies clearly indicate that nanoparticles can transit through ordinary placental transcellular transport. From this paper: “nanoparticles can readily pass through the placental barrier” and, more disturbingly, “that NPs less than 240 nm have transplacental activity in an ex vivo human placental perfusion model.” It is worth noting that the LNPs in the COVID mRNA vaccines range from 100-400nm in size.
Further, in one mouse study, they developed a PEG-ylated LNP similar to the COVID mRNA vaccines that could get to the uterus as a therapeutic delivery mechanism. Apparently, they succeeded given the study’s conclusion: “These LNPs may provide a platform for in utero mRNA delivery for protein replacement and gene editing.”
Further, there is an alarming amount of data showing adverse effects of the COVID mRNA vaccines to fetuses in pregnancy. Let’s start with another document obtained by FOIA from Pfizer and the FDA:
Pfizer received 458 reports of mothers “exposed” to the vaccine while pregnant. In 248 (54%) reports, an adverse event was reported. 53 of the 248 adverse events involved spontaneous abortion.
One team of researchers performed a survey study of the impacts of vaccination on menstruation and were quickly deluged with 140,000 reports. Published in Science, they found that 42% of women reported menstrual abnormalities related to the vaccine.
As stated above, Sonia Elijah reported on findings from a FOIA-obtained Periodic Safety Update Report #3 (PSUR #3) in the EU, which recently became available on an Austrian blog. Here is an excerpt:
There were 697 pregnancy cumulative cases reported, with 597 mother cases and 100 baby/fetal cases. 20% reported adverse events as follows:
● Spontaneous abortions (46)
● Pre-eclampsia (7)
● Cephalo-pelvic disproportion (6)
● Abortion missed, fetal death, postpartum hemorrhage, premature separation of placenta (4 each)
● Abortion threatened, ectopic pregnancy, gestational hypertension, premature delivery, premature labor (3 each)
● Abortion incomplete, hyperemesis gravidarum, maternal exposure via partner during pregnancy, miscarriage of partner, uterine disorder (2 each)
From the list above, it’s noteworthy to point out that “maternal exposure via partner during pregnancy” and “miscarriage of partner” refers to cases of women being indirectly exposed to BNT162b2 by their vaccinated partners. This importantly relates to vaccine shedding, which we know from their clinical trial protocol that Pfizer was aware could happen.
Beyond the European data, Thorp et al., recently published a study of the VAERS database using a CDC established method for detecting vaccine danger signals called “the proportional reporting ratio” (PRR). The PRR is calculated by comparing AE report rates to the rates reported by flu vaccine recipients. The CDC states that a PRR of two or greater is a safety signal “that requires further study.”
The two figures below show the PRRs for 11 menstrual and pregnancy related outcomes. The first on the left calculates it by number of doses given and the second to the right by number of persons vaccinated. The magnitude of the PRRs is unprecedented. Depending on comparator method, having “abnormal menses” ranges from an RR of 298 to 4927 (i.e., well over the threshold of 2). With miscarriages, the PRR ranges from 15-57.
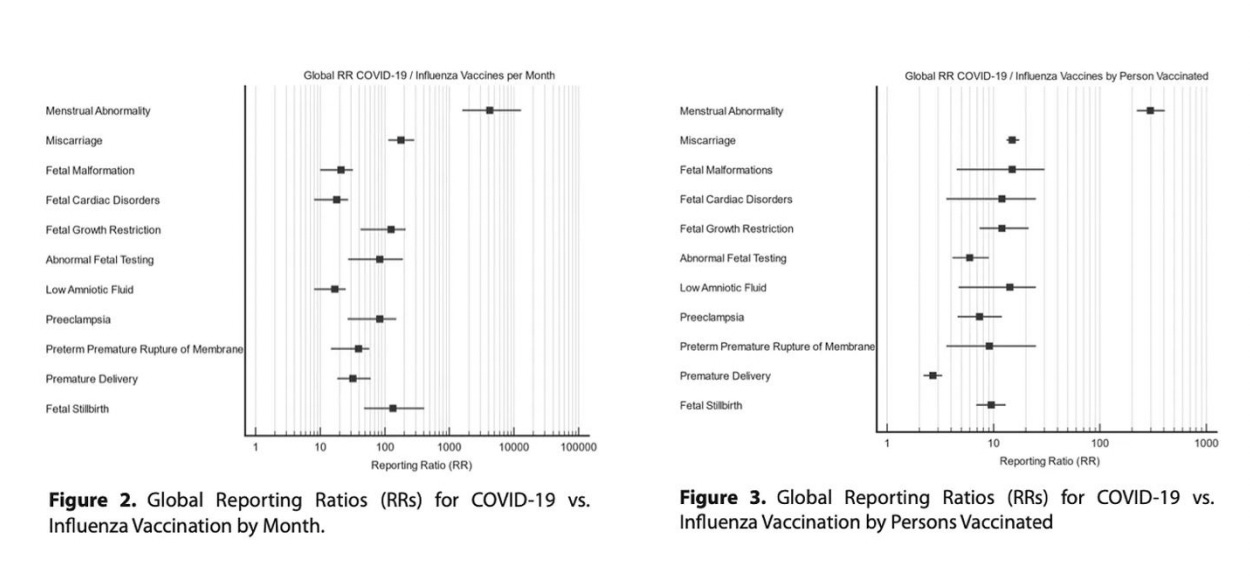
Note the conclusion by this team of authors: “These results necessitate a worldwide moratorium on the use of COVID-19 vaccines in pregnancy.”
In light of the evidence supporting the science behind the mechanisms of shedding, along with the published data supporting the occurrence of shedding between mother and fetus or mother and breast-fed baby, it is clear that shedding of the COVID mRNA nanoparticle gene therapy vaccines is real and can negatively impact fetuses and breast-fed babies of vaccinated mothers.
Evidence For Person-to-Person Shedding
Although the evidence for shedding via either breast milk or the trans-placentally is both considerable and compelling, we are aware of only one peer-reviewed, published study. A 2023 peer-reviewed study found that unvaccinated individuals who were around COVID-19 vaccinated individuals developed an immune response to the spike protein, which the authors hypothesized (we believe wrongly) was due to antibodies being directly transferred through the breath. This in turn demonstrates that something is indeed being transferred from the vaccinated to the unvaccinated (e.g., the spike protein).
In addition to the above, we have been recently informed of a soon-to-be published study nearing the end of the peer review process that found a high percentage of menstrual irregularities developing in unvaccinated women after exposure to the vaccinated.
In order to obtain more clinical evidence, we (and others (e.g., My Cycle Story) made a public call for reports of shedding phenomena. We have currently compiled over 800 reports submitted by people who have found themselves or their spouses to be sensitive to shedding. Although many may dismiss these as “anecdotal” data, we disagree with this assessment based on the following observations:
The descriptions submitted were repeatable and predictable;
The descriptions appeared evenly split between people who reported a cluster of symptoms vs. a single symptom;
Many submissions were by people who only realized they were being affected by shedding once they saw that what they had experienced matched what many others reported. This suggests they did not have a preconceived notion that caused them to hypnotize themselves into believing they were being harmed by shedding;
The descriptions were consistent with the reports compiled by the MyCycleStory survey of 6049 individuals.
In the context of the last four years of immense scientific censorship being practiced by medical journals in an attempt to support the mRNA vaccine campaign, we must note that this is one of the most taboo scientific topics to explore. We do not know if the above referenced study will ultimately be accepted for publication, and thus feel it has become necessary to bypass the peer-review scientific apparatus, which is what we have attempted to do here.
However, while the data we present below looks alarming, we emphasize that it is still fairly rare to encounter individuals being severely affected by shedding. We believe that the over 1000 reports were drawn from a population of approximately 500,000 to one million people who heard our public call for submissions of shedding events and were willing to submit a testimony. One of the reasons shedding events are far less common than mRNA vaccine injuries is that they predominantly affect only the most environmentally or physiologically sensitive members of the population.
SUMMARY OBSERVATIONS OF OVER 1000 CLINICAL REPORTS OF SHEDDING
The below summary of observations of the vaccine shedding phenomena were taken from the public call-out for clinical case reports in this comprehensive post by A Midwestern Doctor.
General Patterns Reported
Two forms of shedding were reported: primary (where someone gets ill from being around a vaccinated person (e.g. vaccinated parents making their unvaccinated children ill) and secondary where someone gets ill from being around a person who was recently around vaccinated people, (e.g., children shedding and affecting parents after coming back home from school). Primary shedding is much more common, but secondary is reported particularly by sensitive patients. Note the primary and secondary shedding phenomenon was clearly addressed in Pfizer’s trial protocol mentioned earlier.
Sensitivity to shedding varies immensely and generally only affects environmentally or physiologically sensitive people. We believe the majority of people who are being affected by shedding are either already aware or will be upon completing this review. We want to emphasize this point so that the rest of the population does not generate newfound fear of being “at risk” from shedders.
Patients develop similar symptoms after a shedding exposure, particularly after a “strong” shedding exposure and the symptoms resemble what is seen in other spike protein-induced syndromes (e.g., long COVID/long Vax).
Many patients will have repeated shedding symptoms emerge after the same exposure (e.g., always feeling ill when a vaccinated husband returns from a long trip away, when going to church each week, when singing with their choir, or when taking a crowded route to work).
In cases where the patient strongly suspects the source of shedding (e.g., the spouse) and they have agreed to testing, high spike protein antibody levels are found.
Eliminating the shedder from the patient’s life or treating the asymptomatic shedder with a vaccine injury protocol has reduced or even eliminated the effects of shedding.
The symptoms often respond to the same treatments used for treating spike-induced syndrome (e.g., ivermectin, which binds the spike protein and/or nattokinase which breaks it down).
Susceptibility to Shedding
In general, there seem to be three categories of people who are susceptible to shedding, however some patients can belong to more than one category.
1) Sensitive patients [e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11].
AMD wrote a much longer article about this archetype, but briefly, these patients tend to be:
● Highly sensitive to toxins in their environment (hence leading to them frequently being injured by pharmaceutical products);
● Very empathetic and perceptive of subtle qualities others do not notice;
● Have an ectomorph or Sattvic constitution;
● Frequently have ligamentous laxity (e.g., Ehlers-Danlos has been correlated with being predisposed to HPV vaccine injuries and many are now reporting EDS predisposes one to a COVID vaccine injury);
● Frequently have chronic illnesses such as mast cell degranulation disorder, multiple chemical sensitivities, EMF sensitivities, Lyme disease, mold toxicity and fibromyalgia;
● Were more likely to avoid the COVID vaccine (due to their previous bad experiences with pharmaceuticals) or more likely to be chronically debilitated by the COVID vaccine (or a COVID-19 infection);
● Tragically, we’ve also seen many people develop these sensitivities after a COVID-19 vaccine injury, and a few people have shared that spike shedding caused them to develop environmental sensitivities (e.g., this reader lost the ability to eat meat unless they addressed their shedding — something we had previously only seen after tick borne diseases).
2) Patients who have been sensitized to the spike protein due to a previous vaccine injury or having long COVID. These patients in turn frequently find their symptoms worsen when they are around individuals who were vaccinated and many have reported that their sensitivity to shedding increases with time.
3) People who cannot effectively produce antibodies to the spike protein. In a study of vaccinated patients who developed myocarditis, those affected were found to be unable to develop a neutralizing antibody for the spike protein leading to a large amount of free spike protein circulating in their blood (thus these patients become symptomatic after being exposed to a much lower concentration of the spike protein).
Characteristics of Shedders
The most common observation with shedders is that they are dramatically more likely to shed soon after vaccination (depending on who you ask, this window ranges from three days to four weeks). However, the more sensitive patients find they are affected by a shedder indefinitely and strongly disagree with a 2-4 week cutoff.
We believe this essentially matches what has been found in numerous studies — i.e., that following vaccination, spike protein production in the blood spikes and then declines but never reaches zero and appears to continue for months afterwards (presently we don’t know how long the effect lasts as it simply hasn’t been monitored long enough although we are now becoming aware of a few cases where testing showed it continued for over two years).
Additionally, quite a few people have noticed that shedding events (in the same location) are the most frequent and severe immediately following a new booster rollout, after which they gradually diminish until the next booster campaign.
It has also been observed that young and healthy people tend to shed more frequently (presumably since their body has a greater capacity to manufacture the spike), children shed the most, and the elderly shed the least frequently. Additionally, quite a few people have observed that shedding greatly varies by the individual (e.g., “I react to specific people I see at church”).
Repeatedly boosting appears to worsen shedding for two reasons:
1) It causes patients to resume having high spike protein levels in their body as typically after vaccination or boosting, there is a spike and then decline of spike protein, which persists at a low level for months (again, no study has yet assessed if it lasts for years).
2) Successive boosting appears to increase the degree of shedding which occurs when compared to the previous injections the patient experienced.
Timing of Exposure
There seem to be three common timelines of exposures:
1) Immediate — Patients often notice this, and either feel as though some type of poison had been immediately injected into them, or that there is an oppressive presence in the area they are entering that makes them feel unwell.
2) 6 to 24 hour delay — This seems to be the most common variant. In certain cases, patients have reported this occurring like clockwork (e.g., every Monday they get ill after they had gone to church on Sunday).
3) Longer term delay — This is often seen in the patients who have the most severe complications from vaccine shedding.
In each of these cases, patients will typically recover after a few days, but there were also many patients who reported a permanent (partial or debilitating) illness after the shedding exposure.
Symptoms of Exposure
Many of the symptoms of shedding appear to match what is seen in both long COVID and Long Vax, again suggesting this is a spike protein mediated disease (especially since the effects of a shedding exposure are often reduced once a spike protein treatment like ivermectin and, to a lesser extent, nattokinase are started for a patient). However, while the symptoms overlap, some are more common after vaccination while a few are more common after a shedding exposure.
All of this we believe is a testament to the fact that the effects of the mRNA gene therapies are not all predictable or consistent and it was hence extremely premature to administer these highly variable injections to the general population.
Routes of Exposure
Based on our review of the over 1000 clinical reports submitted, we believe that the most common route of shedding exposure is by exhaled spike protein containing exosomes as no other route makes sense without closer exposure. However, other routes of shedding were described such as through:
Platonic hugging [e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26].
Sexual intercourse [e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30]
Skin-to-skin contact (this was less common).
Most Common Symptoms
Menstrual Abnormalities
By far the most commonly reported symptoms are gynecologic in nature. Of these, menstrual abnormalities are by far the most common (something also seen with the vaccine), and we have lost count of how many people have shared a story of a short- or long-term menstrual abnormality that occurred immediately after what they, in hindsight, realized was a textbook shedding exposure. Since this is so frequently reported, we will not link to each example of it (as you will immediately find many once you read the comments in AMD’s and Dr. Kory’s articles).
A few women have reported measured hormonal levels changing after shedding exposures [e.g., 1, 2, 3]. The best case report we know of comes from this reader, who regularly measured her hormones and repeatedly found her estrogen spiked after a shedding exposure.
Conversely, another (50-year-old) woman (who is also a physician) shared that after her shedding exposure, her estrogen and progesterone dropped to 0 (while some testosterone remained).
In some cases, highly unusual menstrual abnormalities occur (e.g., profuse bleeding which sometimes is voluminous enough to create severe anemia, or massive clots they’ve never seen before being passed). Many post-menopausal women have reported that shedding caused them to either bleed or develop severe menstrual cramps [e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20]. Conversely, a few cases of women becoming menopausal due to shedding were reported [e.g., 1, 2].
Decidual Cast Shedding
In early 2021, a large Facebook group was formed where they discussed menstrual abnormalities created by the vaccine and from shedding exposures. A large number of people within that group reported experiencing a decidual cast shedding (the entire lining of the uterus coming off as one piece), and since that time AMD met one woman in real life this happened to as well as two other cases here and here. For context, this is a very rare condition (e.g., one paper that looked into this found prior to the vaccines fewer than 40 cases of it had been reported in medical journals across the world — making the condition rare enough that it is impossible to estimate how frequent it is). Further, in a survey that 6049 (vaccinated and unvaccinated) women responded to, 292 (4.83% of respondents) reported a decidual cast shedding event, of whom 277 had never been vaccinated (and of those 277, most reported having been around vaccinated individuals).
Most tragically, several cases of sudden termination of pregnancy were reported where a shedding exposure appeared to end a pregnancy [e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9,
Presently we are unsure if women in general are more sensitive to shedding than men, or if menstruation specifically (which only applies to women) is more sensitive to shedding than anything else, and if the other systems (e.g., the heart) are harmed at an equal rate for both genders.
Note: in men, the closest equivalent to menstrual issues is “groin pain” which while repeatedly reported, did not occur anywhere near as frequently as menstrual issues in women.
Outside of menstrual abnormalities, the most commonly reported symptoms are as follows:
- Headaches*, which are often described as migraines* [e.g., 1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53, 54, 55, 56, 57, 58].
- Tinnitus [e.g., 1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27], which along with nosebleeds appears to be the most noticeable symptoms of shedding.
- Nosebleeds [e.g., 1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24]. These are often profuse, frequent throughout the day and immediately follow exposure to a vaccinated individual.
- Painless and inexplicable bruising* [1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20] is also commonly observed after a shedding exposure, although two distinctly different types are observed. Sometimes many tiny bruises spontaneously emerge, which is often indicative of an immune process destroying the platelets (e.g., see this readers account), but more frequently large painless bruises are observed. Additionally, one reader reported that her limbs, abdomen and veins will turn consistently turn blue (which we associate with blood stasis) 4-6 hours after working with triple vaccinated patients.
- Dizziness* is also frequently reported [e.g., 1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27], and in many cases occurs immediately after physical intimacy with a vaccinated partner.
- Brain Fog/Malaise: mental cloudiness and a general feeling of being unwell (e.g., how one feels before a flu) was also reported. This can include feeling as though a fog has come over them, fatigue, difficulty concentrating, joint pain or quickly coming down with symptoms similar to those experienced when the individual had COVID.
In the same way that the COVID vaccines caused immune suppression and reactivated latent infections such as Lyme or EBV, lighter versions of latent reactivations have also been seen after shedding events (e.g., this is a compelling case history of it happening with herpes). Additionally, this immune suppression may also explain why individuals develop COVID or a COVID-like illness after being exposed to a shedding event. Note: a few readers reported shedding appearing to reactivate Lyme [e.g., 1, 2] and EBV [e.g., 1, 2, 3, 4], although some of these cases may instead have been a reactivation of the CDR.
By far, the most common reactivation associated with the COVID vaccines is shingles, and likewise, the most commonly reported reactivation after a shedding exposure is shingles [1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17]. Note: in some of these cases the link between shedding to shingles is very clear, while in others it is less so. Additionally, we believe some of these cases may be a result of immune suppressed vaccinated individuals directly spreading the shingles virus rather than “shedding” activating a latent shingles infection.
Skin rashes* [e.g., 1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30] are also something we repeatedly saw in the vaccinated (e.g., at dermatology clinics — where sadly the dermatologists insisted again and again they could not be linked to the vaccine). Most frequently these resemble hives, although a few people also reported psoriasis [e.g., 1, 2, 3], shingles-like rashes and areas that felt like a rash but were not visible [e.g., 1, 2]. Here are two examples of the rashes [1,2]:
Note: there are

a lot of nuances to correctly diagnosing skin conditions (especially if you cannot look at them directly), which is why I am hesitant to be more specific.
Less Frequent Symptoms
Some of the less frequent symptoms repeatedly reported include:
Atrial Fibrillation
[e.g., 1, 2, 3, 4, 5]. Many have also reported heart palpitations or PVCs [e.g., 1, 2, 3, 4. 5, 6, 7, 8, 9], which often indicates undiagnosed atrial fibrillation.
Muscle Pain [e.g., [1, 2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15]. This seemed to be a mix of the typical aches felt at the onset of flu like symptoms, severe or chronic cramps and tightening or pain in areas (e.g., the calves) where muscle pain was frequently reported after mRNA vaccination (e.g., this was one of the most common side effects reported by Pfizer in their original clinical trial). One reader shedding report particularly stood out for suggesting that a pathologic process was occurring within the muscle. Numerous readers also reported experiencing other types of musculoskeletal pain after shedding.
Peripheral Neuropathy [e.g., 1, 2, 3, 4, 5, 6].
Insomnia [e.g., 1, 2, 3, 4, 5, 6].
Hair loss [e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9, 10].
Swollen lymph nodes [e.g., 1, 2, 3, 4, 5]. In many cases, individuals reported this swelling immediately after a shedding exposure.
Severe abdominal pain [e.g., 1, 2, 3]. It suggests the possibility the partner is experiencing something similar to mesenteric ischemia as a result of the microclotting in the bowels or an allergic reaction to the shedding agent (e.g., semen).
Sinus pressure or copious nasal discharge [1, 2, 3, 4. 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21].
Vision/Eye Problems: [e.g., 1, 2, 3, 4, 5, 6, 7, 8, 9] such as microclots to the eyes. We saw more severe forms of this with the COVID vaccines (e.g., two retinal infarctions, which traditionally affect around 0.001% of people each year), while the less severe ones appear to be more common after shedding exposures.
Rarer Symptoms
In most cases, the severe vaccine side effects (e.g., a heart attack) are dramatically less likely to occur following a shedding exposure than following vaccination (which to some extent makes sense from a toxicity standpoint as they are receiving a much lower dose of the spike). Nonetheless, quite a few examples of severe effects were reported such as:
Stroke: multiple signs of a stroke* (e.g., drooping facial muscles and difficulty concentrating or driving).
Blood Clots: Severe blood clots* [e.g., 1, 2, 3, 4. 5, 6], some of which were life threatening and resembled those seen after the vaccine.
Severe heart injuries in children [e.g., 1, 2].
Polymyalgia Rheumatica [e.g., 1, 2]. Note: PMR is a debilitating autoimmune disease repeatedly seen after COVID vaccination.
Death: An individual with progressively worsening seizures (due to shedding) eventually experiencing a fatal seizure after a Thanksgiving dinner with vaccinated family members.
Cancers that appeared to be strongly linked to the vaccine shedding. Note: linking a cancer to shedding is almost impossible to prove, but this case provides the most compelling evidence (especially since the recipient received an unusually high shedding dose from her husband). Additionally, her rare cancer was identical to the aggressive one that a Moderna vaccine trial recipient developed (and Moderna never disclosed in their trial report despite the trial participant doing everything she could to get it recognized).
Sensory Neuropathy: a shaking, buzzing, or feeling as though fireworks were going off inside the body [e.g., 1, 2, 3].
Anxiety: One reader reported psychiatric complications from shedding (e.g., anxiety and more easily being stressed by situations.
CLINICAL GUIDANCE
First and foremost, we believe it is critical to not publicly espouse divisive ideas (e.g., “pure-bloods” vs. those who were vaccinated) that prevent the public from becoming united and impactful. The vaccines were marketed on the basis of division (e.g., by encouraging immense discrimination against the unvaccinated), and many unvaccinated individuals thus understandably hold a lot of resentment for how the vaccinated treated them. We do not want to perpetuate anything similar (e.g., discrimination in the other direction).
Likewise, we don’t want to create any more unnecessary fear — which is an inevitable consequence of opening up a conversation about shedding.
Nonetheless, while we do not believe you should be greatly concerned about shedding if it has not yet affected you, we do believe those being harmed by it need to be aware of it and should be treated with compassion and respect rather than being dismissed and ridiculed.
Protection Strategies
What can be done to mitigate the effects of shedding that cannot be avoided?
Many of the approaches for doing this should be evident at this point. For example, a key purpose of this document was to help people identify if they were at an increased risk for being harmed by shedding, and if so (which we do not believe applies to the majority of readers), to encourage them to avoid situations with a high degree of shedding.
In addition, we believe the following options have a lot of merit:
Take an effective proteolytic enzyme. Nattokinase along with Bromelain is the most popular option currently available (although some practitioners feel there are more potent and effective products on the market).
If it seems like you need it (e.g., you know you are sensitive to shedding), consider taking ivermectin to neutralize and bind the spike protein. Unfortunately, there are a cohort of spike protein injured patients who do not have a dramatic response to ivermectin, and likewise with shedding, some individuals who are exposed to shedding notice ivermectin is life-changing for them, while others aren’t sure if it helps.
Another commonly utilized spike protein binding agent is NAC (especially quantum NAC).
Some patients are now using a nicotine patch protocol (which we do not like as we’ve seen a number of patients that had bad reactions and nicotine is addictive but nonetheless it does help some patients).
Additionally quite a few people have benefitted from a zeta potential restoration protocol.
Others have had success with curcumin (unfortunately there is immense variability in the quality of curcumin supplements), Vitamin D, quercetin, and hydroxycholoroquine (while others have tried these approaches without success).
We don’t feel in most cases any of the above are actually needed, because typically “shedding sickness” seems to recover on its own once you are no longer around the shedder, although there have been a number of exceptions to this.
Sexual Partners
What do we currently know about shedding and sexual relationships?
Both the degree of shedding and the susceptibility to shedding vary greatly, so this will probably be the deciding factor if you want to pursue a relationship with a vaccinated individual (e.g., if you know you are fairly sensitive you have no choice, whereas if you are less sensitive you can first test if you react to the individual).
Since the unvaccinated dating pool is very small, this situation creates a significant dilemma for those entering the dating market. Presently our thoughts are as follows:
1) One benefit is that unvaccinated individuals are more likely to be in alignment with your worldview.
2) The website unjected.com is specifically designed for unvaccinated singles to meet each other. Although we think it’s a good idea in principle, it is too costly for many.
3) It is important to go slow with new partners, both so they can understand you are serious about the vaccine (so they won’t boost behind your back and hence expose you to a high vaccine dose) and so you can see how you react to them (e.g., can you tolerate having your mouth be close to theirs. It may be necessary to avoid direct contact with their semen.
4) It is highly likely as time goes forward, more and more people will lie and claim they were never vaccinated, so it will be important to be able to recognize if someone has a body you react to.
5) Many who can tell who is “shedding” have told me they’ve lost their attraction to potential vaccinated partners, so this all may also work itself out on its own.
Blood Supply
What do we currently know about shedding and blood transfusions from vaccinated individuals?
Another common concern we have repeatedly seen raised is if the blood supply is “safe,” and in turn more calls than I can count to create an unvaccinated blood bank for those who were not vaccinated.
We think that as long as the health agencies refuse to acknowledge the dangers of the mRNA vaccines, this will never become a reality given how tightly regulated the blood supply is. The idea that you could create a separate blood bank that hospitals would then be willing to use is unlikely (e.g., consider how far New Zealand’s government went to prevent it from being done on a one-off basis).
Fortunately, we believe vaccinated blood injuries are quite rare (although they have occurred), to the point many of them may have been by chance and not related to the actual transfusion.
To be more specific, we know of three cases, (two here and here, and the third is a patient of Dr. Kory’s, whose history of illness clearly implicated a transfusion).
Further, when Steve Kirsch broached the transfusion subject to approximately 200,000 readers and received 568 comments, we did not find mention of a transfusion injury story.
However, more concerning is that one commenter on an article of Dr. Kory’s came from a hematologist who stated:
“I have seen some unusually severe reactions to RBC transfusions in the past couple years, including a couple that led to pressors/ventilator support. I have wondered if these patients received spike protein containing blood from jabbed donors.”
In line with the above is that in an article on reports from a nurse colleague of Dr. Kory’s, she stated that the hospital was struggling to get enough blood donations from the staff given they had seen so many vaccine injuries in their patients they allegedly felt their blood was tainted and hence weren’t comfortable giving it.
In this article, AMD explores more deeply the mechanisms in which vaccinated blood could potentially make someone acutely ill, however, based on the likely mechanisms, we feel that if people acutely react to a blood transfusion, it’s most likely due to them receiving a transfusion from someone who had recently been vaccinated. This can be prevented by telling people not to donate for a few weeks after vaccination — something the Red Cross already does for the J&J vaccine or if you do not know what COVID vaccine you received.
That all being said, while we do not believe you should be particularly concerned about the vaccinated blood supply, several approaches can be taken to protect yourself:
1) Hospitals will normally let you donate your own blood ahead of time, which can then be transfused into to you if it’s needed during an elective (non-emergency) surgery.
2) Certain drugs allow you to increase your red blood cell concentration. In turn, there is quite a bit of evidence that taking them prior to a surgery with a high amount of expected blood loss reduces the need for the patient to receive blood transfusions.
3) To some extent, blood loss can be compensated for by receiving saline (which dilutes your blood but preserves the total blood volume), followed by either iron infusions (typically done) or chlorophyl consumption (much less known about) to raise your hemoglobin count (e.g., see this trial).
4) The amount of blood loss that occurs during surgeries varies depending on the skill (and finesse) of a surgeon. Because of this, you can likely reduce your need for blood transfusions if you pick the right surgeon to work with.
5) Technologies exist to recycle blood that is lost during a surgery so it can be transfused back into the patient (e.g., the Cell Saver) and when studied, appear to work. Since your own blood is recycled this can bypass the need for a transfusion. In turn, certain surgical facilities offer this option to their patients.
6) Avoid transfusions as much as possible because other contaminants exist in the blood supply and there is quite a bit of data showing repeated transfusions can cause a variety of health issues.
Unfortunately, if you have an emergency situation (e.g., a severe accident) it is unlikely any of these will be viable to do. Fortunately, those situations are rare, and likewise, we believe vaccine injuries from blood transfusions are also very rare.
LEGAL CONSIDERATIONS
When you consider the liability from the vaccine injuries and deaths as well as the harm they have created to those who were unvaccinated, there is a massive degree of legal liability, something along the lines of a “too big to fail” situation. In such situations, governments almost always default to protecting the criminals (e.g., consider the trillions both Bush and Obama gave the banks) rather than punishing them to ensure this does not happen again.
Conversely, the one bright side we see to all of this is that shedding may open up a new avenue of legal attack for lawsuits since this is an unusual situation the blanket liability shield the vaccine manufacturers enjoy may not apply to. Additionally, if it can be proven that a significant number of people are sensitive to shedding, the American Disabilities Act (or OSHA’s requirement to create a safe work environment for workers) may require facilities to protect those sensitive to shedding (e.g., by instructing recently boosted individuals to avoid the facility — which will effectively remove any remaining willingness to take the boosters (which has already rapidly waned).
Know that a Miami school adopted a policy restricting the recently vaccinated from entering in July of 2021. Furthermore, David Gorski (whose blog strongly supports vaccine mandates) has understandably gotten quite upset that businesses might do the opposite and instead discriminate against the vaccinated. In turn, Gorski kindly created a compilation of many other businesses that followed in the Miami school’s footsteps and “banned” recently vaccinated individuals. This, in turn, indicates there is a precedent for private businesses protecting their employees and customers from shedding.
CONCLUSION
We hope you found this review helpful — it’s been a long journey to complete this (especially since it will need to be periodically updated as we receive more feedback). When reading it, we hope you were not overly disturbed by its contents and import. We are presently working with a lot of unknowns, so we have tried our best to provide the most critical information in the most responsible fashion possible.
ACKNOWLEDGEMENTS
This article was compiled with the help of the prolific research by my colleague who goes by the pseudonym A Midwestern Doctor.
P.S I just want to say thanks to all my subscribers, especially the paid ones! Your financial support is greatly appreciated as it allows me to devote what is often large amounts of the limited time that I have available to spend researching and writing my posts, so again, thanks. - Pierre
P.P.S - Proud to report that my book is gaining Best Seller status on Amazon in several countries and is climbing up the U.S Amazon rankings. *If any of you have read it, I would love if you could post an honest review!

I am so thankful to see such a detailed study on vaccine shedding.
I have reacted strongly to shedding; I break out with body wide sores every time I get exposed to a vaccinated or boosted person . The skin eruptions are getting worse with each exposure so I have to isolate to heal.
Most people do not seem to understand this phenomenon but I know it is real.
I am so thankful to know I am not alone in this battle.
This has been up for 5 days and there are only 6 likes. WTF? This is gold.