


New Study Provides Legal Support For The Vaccine Injured
Corporate lawyers beware: "Post Covid Vaccination Syndrome" is now a "real disease." A new Yale study will hopefully help me and my patients' lawyers win them compensation in disability hearings.


A study from Yale was published this week that describes the clinical and immunologic profiles of those that suffer from chronic post covid vaccination syndrome (PVS), a disease that, before this paper, did not exist despite the fact I have specialized in diagnosing and treating it for over three years.
I cannot overstate how important the new Yale study is to the legal and medical plight of these patients. Actually, scratch that, I can overstate it because, let’s be clear, the study is on a pre-print server and until it gets fully peer-reviewed and published in a reputable journal, opposing lawyers will still be able to gaslight both me and my patients in the courtroom (I say this because an earlier version of the study is still on a pre-print server 18 months later).
The disability hearings I have participated in so far have been traumatic for my PVS patients (and me). Opposing lawyers repeatedly deny the association of their illness with the vaccine by aggressively attributing it to other causes, most often Covid itself.
Know that, just as I have devoted massive amounts of pro-bono efforts to defend persecuted doctors, I have also done the same with my PVS patients who are trying to get disability and/or workers compensation. Support in the form of paid subscriptions is immensely helpful in continuing this kind of work so please subscribe if you can:
Fro instance, recall my recent post where I described “losing it” on the stand when the opposing lawyer went so far as to accuse me of tailoring my testimony for a medically destroyed pro-bono PVS patient of mine… so that she would then have the funds to pay for my care. If it wasn’t on Zoom, I probably would have made the nightly news for leaping out of the witness box and punching him right in the #$%@ face (obviously I would not do that but it was cathartic to write).
However, and at the risk of sounding egotistical, the Yale study actually does little to further my clinical (not immunologic) knowledge of their illness because as my readers know, three years ago I opened a specialty clinic with my partner Scott Marsland where we have focused on studying and treating what has turned into the most complex and idiosyncratic disease I have ever encountered. Welcome to the new specialty of “Bioweapon Medicine.”
I wrote a series of posts 18 months ago which described PVS nearly identically to that of this Yale paper:



However, I do think the paper is historic in that this absurd, idiotic ruse of “system” doctors diagnosing (er, I mean dismissing) all of my patients with the more politically acceptable diagnosis of “Long Covid Syndrome” (LCS) will hopefully come to an end.
From the introduction to the paper:
Ya don’t say? Here we are, four years after the mRNA rollout, and finally there is a paper which introduces the concept that the Covid vaccines can cause a devastating chronic illness like Covid can.
Maybe, just maybe, the “gas lighting” by “system” doctors will subside (if they read such papers). For any who have read the earlier posts above, you may recall that 70% of my practice suffer from PVS while only 30% have LCS. What is the difference you ask? Easy:
PVS begins in direct temporal relationship to receiving a Covid vaccine
LCS begins in direct temporal relationship to having fallen ill with Covid
Although yes, in a minority it can be difficult to differentiate the exact trigger, and yes, others are “hybrids” in that both triggers likely contributed, in the vast majority it is child’s play to arrive at correctly identifying the cause of the syndrome.
For instance, if the patient starts trembling with vertigo and chest pain within minutes from receiving the shot, which then progresses over days into the fuller syndrome of fatigue, post-exertional malaise, and brain fog, it ain’t “Long Covid.”
From the Yale study:
“A large fraction of individuals reported the onset of symptoms to be as early as within one day of COVID19 vaccination.”
Are there any other differences between the two? Actually, there are, although they are few and largely inconsequential such that my therapeutic approaches are nearly identical. In my three years of caring for these patients, I have found that:
On average, PVS patients are far sicker (higher rates of complete disability and neuropathies) than LCS patients (with some notable exceptions)
LCS patients without treatment are more likely to enjoy slow improvements over time than PVS patients. This is not to say that PVS patients are refractory to the therapy of “a tincture of time” but rather the effects are much less.
LCS patients can have post-covid pulmonary disease (i.e. residual active organizing pneumonia or fibrosis) in a minority
PVS patients can have spike antibody levels “through the roof” (i.e. >25,000) while LCS patients almost never crest 4,500.
My observations above are further supported in the Yale paper:
“The molecular mechanisms of PVS remain largely unknown. However, there is considerable overlap in self-reported symptoms between long COVID and PVS, as well as shared exposure to SARS-CoV-2 spike (S) protein in the context of inflammatory responses during infection or vaccination.
This overlap is not hard to understand as we have long maintained that LCS and PVS are “spike protein induced diseases” (the name I gave to our FLCCC conference on the topic two and a half years ago):

Similarly, as stated in the Yale paper:
“Given the striking similarities between long COVID and PVS symptoms, there has been speculation regarding the potential causal role of the persistent presence of spike protein driving the chronic symptoms”
We are now getting closer to proving that the spike protein is a “pathogen” - defined as any organism or agent that can produce disease in a host. I wish the entire field of pathology will eventually come to know this simple fact (recall that pathologists are expert at identifying pathogens.. except nearly the entire worlds pathologists are still unaware of this fact as I detailed in one of my most popular posts ever):

The most important point I want to make about LCS and PVS is that they are NOT new diseases! An identical syndrome has been associated with numerous other infections (and vaccinations), such as Epstein-Barr virus, Lyme disease, mycoplasma, influenza, Giardia etc.
PVS and LCS are identical to a disease called “myalgic encephalitis/chronic fatigue syndrome (ME/CFS). For the purists, yes, I know that ME and CFS have different historical origins and emphasize different aspects of the disease, but they ultimately refer to the same underlying condition which is characterized by profound fatigue, cognitive dysfunction, and worsening of symptoms after exertion.
From the earlier version of the Yale study:
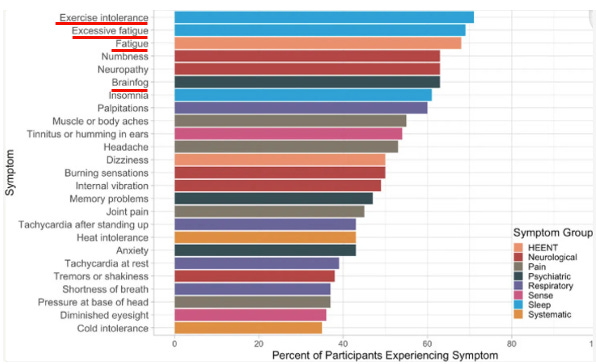
However, as you can see above, those three symptoms are just the “tip of the iceberg” in this disease. The chart above illustrates that powerfully: 13 different symptoms are reported over 50% of the time.
As per my previous post on the symptom burden of PVS patients, after the “Big Three” above, the next most common are:
Sensory neuropathies (burning, tingling, pins and needles, numbness, pain, electric shock like feelings)
Dysautonomia (POTS, i.e. high resting heart rates, spikes in heart rate on position change or minimal exertion, labile blood pressures, temperature dysregulation - feeling hot or cold or sweating, then GI issues like abnormal stomach emptying and peristalsis).
“Cranial” issues ( vertigo, tinnitus, dizziness, headaches, visual disturbances)
Atypical Motor neuropathies (fasciculations, weakness, ALS like syndromes, tremors, shaking, convulsions, ballismus, flaccidity, and dystonic reactions).
Others (arthritis, skin diseases, cancers, heart attacks, strokes, blood clots, autoimmune diseases, myalgias, etc
Editor note: This study was done by a group of immunologists and primarily focused on the numerous immunologic profiles and abnormalities they found in PVS patients. I am ignoring these for now, but will include a brief summary in the post-script.
Know that the Mayo Clinic was quick to recognize the rising epidemic of ME/CFS in Covid when they decided to publish this position paper below in November of 2021, warning of a rising epidemic of ME/CFS due to SARS-CoV2 (but not the vaccine)::

A study of patients ill 6 months after mild or moderate acute COVID-19 found that about half met criteria for ME/CFS.14 One review suggested that the number of cases of ME/CFS could double as a result of the pandemic.6 Like ME/CFS patients, those with post-COVID conditions have recounted being dismissed by health care professionals.15
Know that, as they describe in that paper and I will expound upon personally, ME/CFS is devastating medically and legally because:
“System” doctors do not have the time, skill, or interest in treating such a complex, often refractory, and idiosyncratic disease
Besides “pacing of activity levels,” no single treatment works in everyone (not even close) and some fail to respond to even a dozen trials of therapies.
ME/CFS is a “clinical diagnosis" which means that the diagnosis is based upon the symptoms the patients report - there is no definitive diagnostic test; physical exam findings are often unrevealing. Blood work is either completely normal or non-specific. Imaging is almost always normal (MRI brain, CT’s ultrasounds, X-rays etc.)
ME/CFS is thus one of the worst diseases to present with in medicine because doctors literally decompensate intellectually and psychologically when all the testing is normal but the patient is reporting 7-15 often debilitating symptoms. This leads them to diagnose the patients with anxiety, depression, or the worst fate of them all - “functional neurologic disorder” (FND). Once that appears in your chart, you are cooked in terms of getting other clinicians to take you seriously or offer you treatments to mitigate your suffering.
The point of this post, is that because of the above, it is very very difficult to get disability. Neurological exams by disability physicians will often find normal strength, tone, gait, reflexes etc. Mental status exams - normal. Vital signs - normal. Echocardiograms and pulmonary function tests - normal. Clearly the patient can go to work, or at least sit at a desk for 8 hours no?
Answer - NO! And that is due to the most maddening and horrific symptom of them all which is “post-exertional malaise” or PEM. Meaning, when my ME/CFS patients try to exert themselves, even as little as going to the curb to get mail, or God forbid, emptying the dishwasher or running an errand, they are “destroyed” for hours to even days later. “Destroyed” meaning so fatigued that they cant get out of bed, or their other symptoms flare - headaches, dysautonomia, dizziness, neuropathies etc.
Prognosis of ME/CFS
I need to correct myself now because the real “worst thing” about the disease is its prognosis which is why the denials of disability for PVS patients is not only catastrophic, but also devastatingly cruel given the vast majority were coerced into getting the vaccine. As per the Mayo Clinic paper:
ME/CFS substantially impairs occupational, educational, social, and personal activities.
The degree of impairment can exceed that of rheumatoid arthritis, multiple sclerosis, depression, heart disease, cancer, and lung disease. There is a wide spectrum of severity ranging from mild to very severe:
Up to 75% are unable to work, and an estimated 25% are consistently housebound or bedbound. The level of severity can fluctuate, with 61% reporting being bedbound on their worst days.
A systematic review concluded that the chance of full recovery is only 5%.
One ME/CFS-focused clinical practice estimated that 50% of its patients were still ill after 2 decades whereas a second estimated 93% (oral communication, US ME/CFS Clinician Coalition, March 2019).
Temporary remission is reported, but relapses often occur. Patients most commonly report a fluctuating illness pattern in which symptoms wax and wane but are always present.
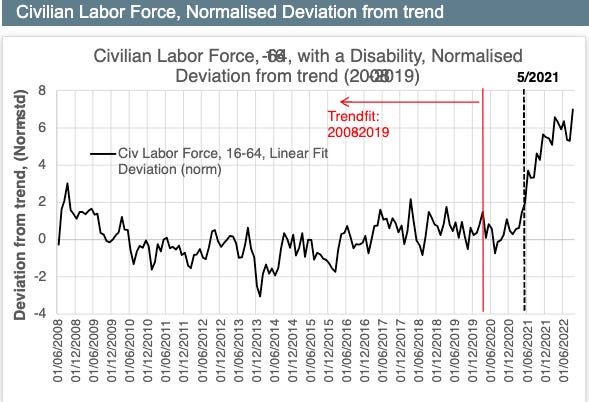
Now some might understand why “disability” claims are skyrocketing to historical record levels in the U.S in the wake of the mRNA campaign, a trend expertly captured by the work of Ed Dowd and his team (note the chart only goes up to 2022, it has gotten even worse since):
So, if ME/CFS is a devastating illness in “normal” times, what was it like for PVS patients in Covid? Beyond the fact my patients would all present with histories of either physicians “getting angry” when they would tell them the vaccine caused this, or they would be gaslighted by the physicians telling them, essentially, “it’s all in your head”, or they would say, “I don’t know what this is” and then order endless tests and/or referrals to get them out of their office. Referrals to physical therapy were particularly pointless and/or harmful.
Remember the “atypical motor neuropathies” that I listed above? Know these were some of the most devastating symptoms to witness (and treat) and which also unfortunately triggered the worst narrative of Covid which is that the vaccine injured were “faking it:”
The above was helped along by supposed Covid vaccine toxicity expert Alex Berenson, someone I cannot think about without developing near rage after he publicly lambasted one of my patients, Angelia Desselle, for “faking her symptoms.” His public dismissal of her helped fuel the above narratives as evidenced in this article in which the journalist writes:

“Late last month, a video resurfaced from 2021 of Angelia Desselle, a then 45-year-old woman from Louisiana attempting to walk while supposedly experiencing these symptoms, which she claims were developed after receiving a COVID-19 vaccine. This is just one example of many.
Since Desselle's video was reposted on Twitter, it's been viewed more than 72 million times, helping to reignite controversy over the safety of COVID vaccinations.”
Berenson went even further by even dismissing Long Covid as a real disease:
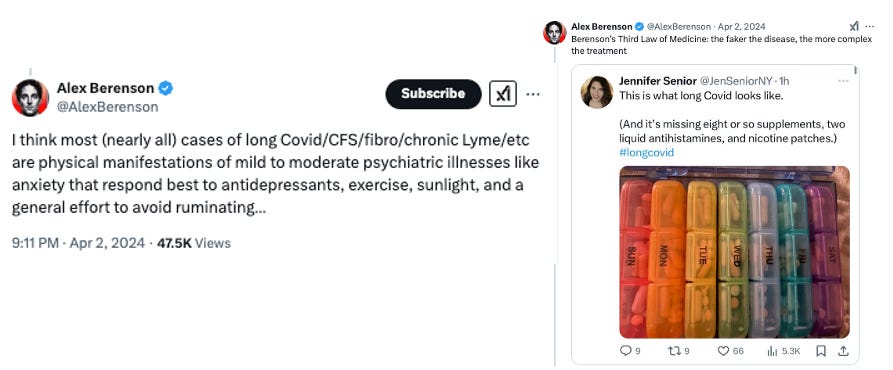
I wish “Doctor” Berenson could know what would happen when my ME/CFS patients attempt to exercise. For the sickest, it would lead to an almost complete medical collapse followed by hours to days of worsening symptoms. I won’t even bother to address his recommendation to try antidepressants.
From the Yale study:
In conclusion, people reporting PVS after covid-19 vaccination in this study are highly symptomatic, have poor health status, and have tried many treatment strategies without success. As PVS is associated with considerable suffering, there is an urgent need to understand its mechanism to provide prevention, diagnosis, and treatment strategies.
Conclusion
This study is the first to recognize and describe the disease that I have been treating for over three years, a disease which I had been calling “Long Vax syndrome” but which I will now call PVS.
Knowing that PVS exists is extremely important because, conveniently, no-one can be held liable for my patients having gotten ill from Covid (LCS) but they hopefully can be held liable for having mandated a toxic, illogical, barely tested, and poorly manufactured (understatement) “vaccine” which destroyed their health and livelihood.
Although I am not a lawyer, based on the suffering and disability I see on a daily basis, I would imagine a fair compensation for one of my disabled PVS patients would run into the millions of dollars (and still would not fully compensate some).
Unfortunately, to date, I have “won” a workers compensation case for only one patient. In a half dozen other disability cases, all were denied.
I truly hope this paper passes peer-review and publication so that it will support my expert testimonies in disability hearings as they are truly the only way for society to even come close to reversing the immense harms and suffering that the mRNA campaign inflicted on millions of people around the world.
If you appreciate the effort and time I spend researching and writing my post as well as defending doctors and patients, support in the form of paid subscriptions is greatly valued.
IMMUNOLOGIC FINDINGS
My colleague AMD did a more comprehensive review of the immunologic findings by the Yale group in their post yesterday so here I will present a concise summary of them:
The COVID vaccine spike protein can persist for years in the body.
In many cases, COVID spike protein persistence eventually stopped but symptoms continued
CD4 and CD8 cells had signs of being “exhausted,” i.e. partially losing ability to respond to infections due to a chronic over-activation of them (e.g., by persistent vaccine spike protein).
Viral re-activations were found, most notably with Epstein Barr virus, but also with herpes
Significant increases in IgM reactivities against 65 antigens, IgG 309 reactivity against 1 antigen and IgA reactivities against 39 antigens in PVS compared to controls after multiple testing corrections.
Among these antigens, two showed log₂fold change of greater than 2: anti-nucleosome IgM [which is strongly associated with lupus] and anti-AQP4 IgA [which is associated with a rare autoimmune disorder that attacks the central nervous system, particularly optic nerve and spinal cord].
Per AMD:
This study is extremely important as it provides objective proof the vaccine is indeed doing something harmful and abnormal, and that it is occurring long after vaccination. As such, when this topic is broached with a skeptical doctor (or academic) you can now say “did you know a multi-year Yale study recently discovered that the vaccine does chronically damage the immune system of certain recipients and cause a variety of persistent and debilitating symptoms?”
"Bioweapon Medicine," indeed. It was easy for me to reject the covid vaccine after spending three years being gaslit by the medical profession regarding my daughter's illness -- which turned out to be Lyme.
It's astonishing how many people still have no awareness of the well-funded research programs that have been ongoing since the 40s to weaponize everything that flies or crawls. I wonder how many of those programs will collapse now that this new administration is shining a light in so many dark corners. I pray they all do.
Continue the good fight, Dr. Kory. xox
Big Pharma has been sued many before for its very toxic products...and it uses the "Stall Technique" to keep on making massive amounts of money, while litigation keeps going on.. Many are now aware that all this focus now on bringing info to light about the CV-19 vax...does not get to the very CORE of the PROBLEM...The profound ignorance of those who call themselves doctors who would inject poisonous matter into the bloodstreams of other human beings...and declare it would provide IMMUNITY???? For 64 years, I have studied a subject called health and nutrition...it is shocking to me to think that educated doctors don't know how the body works! The right food produces energy and health. The wrong food. will produce illness.. Too simple! The AMA was taken over in 1910 by John D Rockefeller to promote his patented petroleum-based drugs...any other healing modality was eliminated. This is not just about the CV-19 health-destroying vax...it is about an INDUSTRY that has nothing to do with the subject of HEALTH. The entire INDUSTRY is of no value to mankind.