

Hospitalized COVID-19 Patients are Systematically Dying from Under-Treatment with Corticosteroids - PART I
US hospitals and their doctors almost never deviate far from the standard, anemic NIH recommended dose of 6mg of dexamethasone daily. Numerous studies support far higher doses far earlier in disease.


As a now renowned (infamous?) U.S pulmonary & critical care specialist with numerous co-authored publications and extensive experience treating COVID-19 in all it’s phases, almost every day of this pandemic, and sometimes multiple times a day, I am contacted by someone in my ever-widening circle of friends, family, or colleagues asking me to help a loved one who is deteriorating from COVID in the hospital. The case is invariably one of an often older (but not always) patient mired on a hospital ward or in an ICU, whose illness has progressed to the point where they require near maximal or maximal oxygen/ventilator settings and the patients and family members begin to question whether “enough is being done” or “is there more the doctors should be doing?” So they reach out.. desperate for help.
The therapeutic regimen that their loved one is on is nearly identical in almost all cases, especially on the hospital wards where a generally anemic dose of a corticosteroid called dexamethasone (standard of care worldwide for COVID patients in the pulmonary phase of disease), along with remdesivir (“run death is near” as some nurses have called this drug), and occasionally a medicine ending in “ib or ab” (classes of expensive medicines that block a specific inflammatory mediator called a cytokine, such as tocilizumab, sarilumab, or baricitinib) and some form or dose of a blood thinner. If lucky, some may get high-risk, costly interventions such as Vitamin D or zinc or melatonin (sarcasm noted yes?), and patients are generally on or have completed some almost certainly unnecessary antibacterial agent “just to be sure.”
In later posts I might explore some of the above raised issues more deeply, like the corrupt dangers and inefficacy of remdesivir, the costly and needless “ibs and abs”, antibiotic over-use etc. but today, I want to focus on the singular and most important treatment deficit (too low a dose of corticosteroid), which, if systematically corrected, likely presents the greatest opportunity to improve the survival chances of COVID-19 patients after entering the hospital by keeping them out of ICU’s and off ventilators (and reducing the accumulating PTSD I acquire from these daily calls for help). Please note that in almost every single instance that I am asked to help, I can offer zero help because less than 1% of physicians either feel they need outside help or desire to have a clinical discussion with a supposed “expert” (the near majority of docs are convinced they know COVID as much or more than anyone else).
So, I thought it might be interesting to run through the “history” of my own and the Front-Line COVID-19 Critical Care Alliance’s (FLCCC for short) long-standing knowledge of the need for higher dose corticosteroids in COVID-19.
Let’s start at the beginning when COVID-19 began to roll across the world. Every doctor caring for a COVID-19 patient was looking for guidance on how to treat the disease. The below table summarizes the inital guidance they recieved on the use of corticosteroids, coming from the worlds major national and international health care societies:
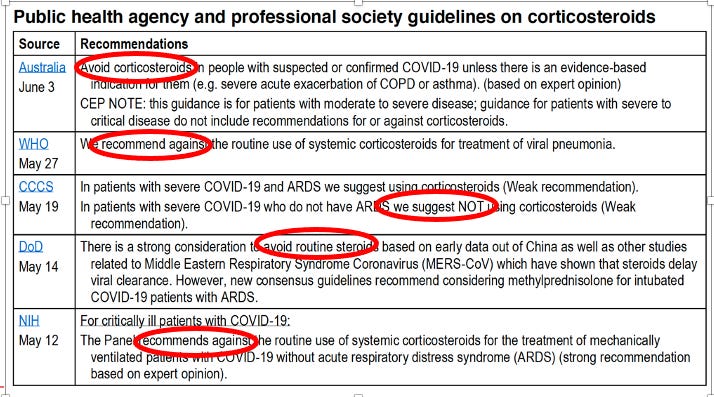
And so was born the FLCCC’s first mission: advocating for effective treatment of COVID-19 by trying to get the world to understand that it was a “corticosteroid responsive disease.” Off we go:
April 2020 – Dr. Umberto Meduri, one of the founding members of the FLCCC, co-authored a paper with a group of international critical care experts which argued against the global prohibition against corticosteroids in severe COVID-19 acute respiratory distress syndrome (ARDS), based on a robust analysis of studies conducted during prior coronavirus and influenza pandemics (SARS, MERS, H1N1) as well as his deep, lifetime career experience studying the role of corticosteroids in severe lung injuries and critical illness. All the leading health agencies above were echoing a misinterpretation of the observational data from those pandemics in that although those earlier studies found that patients who received corticosteroids died more frequently than those who did not, it was also true that the patients that were more severely ill and more likely to die…were given steroids! Meduri’s group argued that the largest and most carefully done analyses of SARS and H1N1 studies (by carefully controlling for dose, timing, severity of illness, age, and comorbidities found that treatment with corticosteroid therapy in viral induced ARDS.. led to a massive 50% reduction in mortality. Despite the fact that the Society of Critical Care Medicine blasted this paper to many thousands of their members.. the paper and its conclusions was ignored by every society and health care agency across the world (with the exception of the FLCCC :)).
May 2020 - I left the University of Wisconsin to help my former hospital in New York City - Mount Sinai Beth Israel. They were inundated with severe hospital cases and all my former colleagues and trainees were exhausted. Upon resuming the care of my old ICU, I became quickly intrigued by how all these COVID patients were presenting early on with “happy hypoxia” - a description meant to convey the combination of low oxygen levels with a lack of breathlessness or discomfort. I had definitely seen patients present in similar fashions but they were rare in my mind.. I couldn’t put my finger on the connection until one night, I was obsessing about this familiarity as I was trying to fall asleep, when it suddenly hit me that these patients reminded me of patients with a rare-ish disease called “organizing pneumonia (OP).” The name is actually a confusing one becuase OP is not an infectious illness but instead a reaction to a lung injury, typically from an unknown source or most commonly a drug reaction. In some cases, it can be “associated with” or “caused by” a viral infection but it is not a true infection itself.. in that, the treatment is as follows: 1) remove offending agent/drug and/or 2)treat with... corticosteroids (and use high, “pulse doses” in fulminant cases). These patients were notoriously in need of oxygen, often for prolonged periods, and often in high fractions despite being fully conversant and not in overt respiratory distress while resting in their hospital beds. “Happy Hypoxia” solved! SARS-CoV2 was causing an “organizing pneumonia”.. in almost everybody?
So, in order to validate my hypothesis, first thing the next morning, I called my friend and close colleague Dr. Jeff Kanne at the University of Wisconsin, one of the worlds premier chest radiologists and someone whose intelligence and skill in the field is nearly unparalleled. As soon as he answered the phone I said, “Jeff, what would you say if I told you that I think that all of these Covid patients are suffering from organizing pneumonia?” His answer? “Of course it is, we wrote this up in March in the journal Radiology after an expert panel that I chaired had completed our review of all the CT scans from Wuhan.” (turns out they literally had written in their expert report “the most common reported CT findings in COVID-19 patients are typical of an organizing pneumonia pattern of lung injury.” I then started yelling “no clinicians read radiology journals! We need to publish this in a clinical medical journal! Like NOW!”. We quickly agreed to write it up together. I went home after my ICU shift and started working furiously on it. The paper accumulated the radiographic, pathologic, and clinical evidence to try to prove that the pulmonary phase of COVID-19 was an organizing pneumonia and that the first line therapy for this condition was.. corticosteroids. As brilliant as this hypothesis was (forgive me for I am biased) it took me 4 months and 6 journal submissions with 2 peer reviews until it was finally published in a prominent journal. The highlight of that journey was the rejection letter I received after a rigorous peer review in the American journal Chest, when the peer reviewer who voted for rejection wrote, “in order for this paper to be published, a randomized controlled trial of corticosteroids would need to be performed.” Yup.
Come on back for Part 2 (am almost done) where I finish detailing the journey to anemic doses of corticosteroids becoming the standard of care worldwide for COVID-19 (including the first time I lost my temper during U.S Senate testimony (starts at 48:30).
P.S. I hope you enjoyed my first substack. If you did, please subscribe, and please note that founding member subscribers will get invitations to a private zoom discussion/Q&A every month :).
Excellent first sub stack Dr Kory! And thank you for moving over here as well, I constantly worry that one day the Twitter Gods will poof you as they did with Dr. Malone.
Dr. Kory, thanks for all you and your alliance have done. You all have saved countless lives. Keep fighting censorship and spread the truth!