

Debate: Was Covid-19 A Pandemic Caused By A Novel Pathogen Or Was It Created Solely By Harmful Policies and Fear Propaganda?
In a What's App group chat, a number of data experts and scientists have been debating this question with front-line clinicians. Here I compile the debate arguments.

In the spirit and intent of fostering respectful scientific debate, a group of colleagues has asked some of us front-line clinicians to reply to a post written by Martin Neil, Jonathan Engler, and Jessica Hockett titled “'Spikeopathy' does not explain the 'novel' symptoms associated with COVID-19.”
Obviously, if you are interested in following the debate, the points raised and the points countered, it is mandatory you read the post above before proceeding with the below.
If you didn’t or don’t want to read it, I will instead summarize their main argument and findings. In no particular order, besides the post above, in the What’s App exchanges, these points were made by various members who have taken the position that “no novel pathogen existed.”
NICK HUDSON:
To summarize:
1. In Covid itself, there was no medical emergency of any sort.
2. Policy measures created a medical and social emergency of many dimensions—a mass casualty event at its most acute around the declaration of the (fake) pandemic.
3. The vaccines created a medical emergency of uncertain quantum and duration.
4. The drive towards digital IDs and CBDCs constitutes a political emergency.
5. Sustenance of the viral bio-weapon myth, inter alia, provides cover and justification for 4.
6. A not inconsiderable number of high-ranking policymakers were sighted on all of the above from the start, knowing that there was no material risk in Covid and considerable risk in the vaccines.
MIKE YEADON:
(in a reply to my descriptions of the clinical syndrome):
I’m sure you’re describing what you saw, but there’s a problem.
The epidemiological evidence doesn’t square with there being a highly transmissible & above average mortality.
Perhaps you dispute what Denis Rancourt & colleagues have published?
There was no hint of increased illness or death (as measured by all cause mortality) in USA (state big state) until after WHO called a pandemic.
(It is on this basis that I’ve been saying there’s been no pandemic).
How could this be if there was a highly contagious & above average lethality pathogen?
Separately, I’ve looked & looked and I’m unable to find in the literature good evidence of contagion in influenza like illnesses broadly. Patients with acute respiratory illnesses that are classified as Influenza-like illnesses (ILI) were unable to cause healthy people brought into contact with them to acquire symptoms of ILI. There were several experiments attempted & they were unsuccessful.
Do you know of literature that demonstrates symptomatic contagion of diseases of this kind?
The PCR-based diagnostic tests are not meaningful. How did you differentially diagnose “covid19” from other ILIs?
SEAN FLANAGAN:
As per my previous above👆, to me as the non-medic, non-scientist, ordinary Joe here, my net net short summary take away from our debate, discussion and various discussion on and our Twitter Spaces:
all the data in 2019, Diamond Princess 🛳️ Jan 2020, and 2020 BEFORE Lockdowns & NPIs in March, and ACM numbers and no Excess Deaths, points to No ‘Pandemic’ (of Oct 2019 & prior WHO definition?) and ‘Cases’ declining in March 2020 before Lockdown & NPIs.
The 2020 ACM and Excess Deaths data and numbers pre mid Dec 2020 commencement of mRNA injection roll out, point to No ‘Pandemic’
“There was something (or somethings) different in circulation which we had not seen before, but was totally manageable if treated properly” - words/quote to this effect on one of our Spaces by @Lynn Fynn and some Frontline Drs have said they saw some different ‘stuff’ earlier in 2019.
As previously mentioned here above 👆 and on our Twitter Space, various Frontline Drs around the world (including those here) were going about their normal business of “Treat What You See” with existing medications and therapeutics and sharing information, and IF the WHO, Gvt’s, Public Health, MSM, Big Tech et al had NEVER mentioned or declared ‘Pandemic’ or any of the data and fear porn They instigated….. then the whole world would have just carried on as normal and Frontline Drs globally would have swapped notes as to what was working (like our side did) and just carried on going about their day to day “Treat What You See”, and, with no interference and left alone to do what they do, aside from a bad and ‘strange’ or ‘different’ flu season, all would have been fine. This points to no ‘Pandemic’.
Prof John Ioannidis IFR%s are consistent with the above.
Is this a fair and accurate short summary that we can all sign ✍️ up to….?
This more recent one by NICK HUDSON lends supporting data for their hypothesis that propaganda and harmful policies was the cause of the pandemic:
“Read this whole thread. The perpetrators knew exactly what they were doing. Don’t miss the section on how autonomic responses can create flu-like symptoms.”
Nick is referring to this Twitter thread by Champagne Joshi , i.e. @JoshWalkos
A 2006 DHS document about the possibility of a “Mass Psychogenic Illness” they define as: “A phenomenon in which social trauma or anxiety combines with a suspicious event to produce psychosomatic symptoms, such as nausea, difficulty breathing, and paralysis. If many individuals come to believe that the psychosomatic outbreak is connected to the cause of the trauma or anxiety, these symptoms can spread rapidly throughout a population.” Particular focus is given to a CBR Event (chemical, biological, radiological). “particularly those involving chemical, biological, or radiological (CBR) weapons. The number of those suffering psychogenic illness could far exceed the number of actual casualties in a CBR event.” Some implications stated in the document: “The observed symptoms of many mass psychogenic illness events are similar to several non-specific symptoms of possible chemical and biological weapons—including chemical agents, inhalational anthrax, and avian influenza.” “Recent cases of mass psychogenic illness display a transferal of the symptoms onto contemporary anxieties.”

Next, they submitted this 9 minute lecture by Prof. Denis Rancourt who states the following conclusions based on his extensive analysis of “all cause mortality.”
there was a peak of deaths early on in certain hot spots that was directly due to how people were treated in hospitals and care homes
There was no pandemic, instead there was intense propaganda
There was no particularly virulent pathogen
There was nothing that was spreading that was causing death, “mortality didn’t cross borders, there were areas without any increase in all cause mortality right next to “hot spots” where there was.
In more than half the countries studied, there was no increase in ACM until the vaccines were rolled out
Nick Hudson and Mike Yeadon agree with the above and they ask:
Let anyone who takes a different view please either:
1. Refute Rancourt’s basic analytical methods, findings and conclusions or
2. Offer an interpretation of events that squares the circle of a pandemic of a contagious & somewhat lethal pathogen, notwithstanding Rancourt’s findings.
FRONT LINE CLINICIAN “REBUTTAL”
I will state at the outset that I/we will be unable to fully “square the circle” in providing an explanation for all the anomolous events and data described.
However, as a clinician, the only point I wish to and believe I am able to counter is the assertion that “there was no novel pathogen.”
We maintain that there was a novel pathogen which caused a novel syndrome and that it was initially particularly deadly in many areas (Lombardy, NYC, Seattle, Detroit, New Orleans and others), and not just to the old, at least in my clinical experience.
However, what I cannot explain is why certain hot spots became medical disaster zones while other areas or countries, apparently not far away geographically did not exhibit such manifestations. I believe this latter question comes after we decide whether there was a novel pathogen. Then we can try to answer why this novel pathogen affected certain areas and places disproportionately.
One aspect of the “no new pathogen” camp’s argument is based on the existence of antibodies to SarsCoV2 found in numerous places in 2018 and 2019 before the Wuhan outbreak. Thus they conclude that the disease had been around, but the catastrophic impacts only occurred after the WHO declaration, media fear mongering and the illogical and harmful lockdown and mask and social distancing policies.
We counter with the fact that whatever was causing antibodies to be made in certain places in 2018 or 2019 did not have the pathogenicity of the “new variant” which seemingly escaped or was leaked out of Wuhan. I have one data point which might support the “emergence of a new deadly strain” of SARS-CoV2 from Wuhan:
In this WSJ article from August 2020, they describe a CDC “early warning system” for pandemics which was based on “listening” for key words across the global internet. In the article, they describe a post which was flagged by the CDC early warning system from a Wuhan Health Ministry website on Dec. 31, 2019 which had this recommendation: “Avoid closed public places and crowded places with poor air circulation.”
Know that to me, this is the first evidence that a pathogen was circulating in Wuhan with novel characteristics, i.e. the ability to transmit through the air. That is the only reason why a health ministry website would tell the public suddenly that they “should avoid closed public places and crowded places with poor air circulation.” I maintain that the Chinese knew immediately this thing was airborne. The article then goes on to casually state that the website post was taken down within hours. But it spooked the CDC. And it spooks me to learn of it. I believe this was the first warning that something big and bad had just been leaked or escaped and spelled trouble due to its high transmission properties. That is why they said to avoid poorly ventilated places. Know this was months before the WHO declared a pandemic.
And that by the time the WHO declared a pandemic and then ACM started to rise should be understood as that - a real pandemic of a newly highly transmissible respiratory pathogen had erupted. And thus, the ACM increases were not secondary to WHO declaration of the Pandemic, fear mongering, and lockdowns, but instead reflected the reality that a rapidly spreading viral illness syndrome was affecting a lot of people. Yes, the timing of the rise in ACM started only after the WHO pandemic declaration which is troubling to contemplate. However, as little as I want to give the WHO credit for any decision they have made, the declaration appeared to be supported by the clinical reality on the ground - lots of people getting sick with a minority getting really sick (a minority of a suddenly very large number of infected people such that this “minority” overwhelmed numerous urban areas in terms of hospital capacity). I know this did not happen everywhere, I personally do not have the knowledge or expertise to explain the transmission patterns globally, but my best guess is something nefarious contributed to the anomolous spread, something as preposterous as deliberate widespread release in certain targeted cities and areas.
Anyway, beyond the evidence above that a novel pathogen with significant airborne transmissibility likely emerged from Wuhan in December 2020, is the fact that Fauci et al immediately embarked on a massive cover-up of their bioweapons research being implicated (if not obvious, “gain of function” research is bioweapons research). Why did they go to such lengths to cover up the origin of a pathogen “that didn’t exist?”
OK, back to the “novel pathogen” argument. I will relate some of the key points that I believe the non-clinicians overlook and why I maintain this was a novel and severe disease:
Outside of a biopsy of tissue or culture of a pathogen, there is no uniquely diagnostic criteria for any disease, certainly no single radiographic finding, symptom, or lab abnormality. All such findings are always, by definition, non-specific as they can be found in a number of diseases (the organs of the human body have a narrow range of symptoms they can express when sick, thus many different illnesses share symptoms and lab abnormalities. Learning how to discern among overlapping symptoms, findings, and blood tests and radiographic abnormalities is literally the core skill of a medical doctor and why training is so long and why we need to see so many thousands of patients in order to acquire sufficient diagnostic capability). If you doctor long enough, you find that discerning amongst diseases is not as difficult as when you start out.
Further, what must be recognized is that Covid-19 is not just a few viral symptoms, but rather presents as a “syndrome” with a wide but predictable constellation of findings, and although a number of the abnormalities are non-specific, when they present in clusters or simultaneously, then you can differentiate Covid as a unique and/or novel syndrome by comparing to how pre-existing infectious or viral disease syndromes present.
Also know that in medicine, since it is rare for any single test, symptom, of physical exam finding to be diagnostic of a single disease, what physicians do as a core skill is to amass all the presenting data including “history of present illness” (triggers, timeline, context, contributing factors, medical history, travel), physical exam findings, lab and radiographic abnormalities etc) and then generate a “differential diagnosis,” ranking the likelihood that the patients presentation is one disease or another, something like, “these findings strongly support Covid-19 given bilateral ground glass opacities on CT, typical viral symptoms, illness beginning after a holiday party where a number of others also subsequently fell ill, the elevations in D-dimer, CRP, ESR, low lymphocytes, significant hypoxia without an accompanying increased work of breathing, and abrupt improvement in oxygenation after administration of ivermectin.” For example. Further, I would also then write “bacterial pneumonia is less favored given bilateral findings vs. unilateral, lack of consolidation on CT, dry cough unproductive of phlegm, lack of elevated neutrophil count, lack of pleurisy, obvious contagiousness as per history etc). Know that in the above examples, I chose a relatively “clean” set of findings which allows one to rule in or rule out a diagnosis. Certainly there were times where the totality of findings may be less discriminating as to cause, but in general, hospital phase Covid presented very similarly.
The strongest point that I can make is that, even if not ALL features below were present in the hospitalized patient, generally most of them were present, and I had never seen a syndrome with such reproducibility of this constellation of symptoms and findings, thus leading to what I felt was a high specificity of diagnosis. Making a diagnosis of Covid in the hospitalized patient was not difficult. In an outpatient whereby all you have is generally mild clinical symptoms to differentiate patients by, I completely agree that in many cases Covid would be hard to confidently differentiate from other respiratory viruses. But as the illness progressed and became severe, it had a unique set of findings on presentation and a unique trajectory once in hospital. Also know that Paul Marik was reprimanded for saving a mans life because he treated the man with a large combination of therapies which made up our COVId MATH+ protocol. Why was he “reprimanded?”. Because the man had had numerous negative tests for Covid, but Paul treated him for Covid based on his “clinical” diagnosis of the syndrome which was pretty classic. Nothing else fit better than the diagnosis of COVId, despite the negative PCR test. So Paul treated him and he survived but this did not stop his actions from appearing as a complaint in his personnel file.
Again, the “specificity” was a cluster of findings, not any individual one! When 8 out of the ten findings are present, you have a diagnosis. When 6 out of the 10, you still have a confident diagnosis. And then, just to add to the complexity, there are also, like with any disease we study and treat, “atypical” presentations, like my oldest and best friend who simply got nauseous, started projectile vomiting, went to hospital and was eventually diagnosed with adult onset multi-system inflammatory syndrome related to Covid (note he was Covid positive on admission). But know that he never had a preceding upper respiratory symptom however all the other findings were consistent with the new rarer syndrome of MISC-A.. So, atypical presentation, but his eventual A-MISC syndrome has criteria for diagnosis and he met all of them. I have also seen, on few occasions, other presentations that were atypical, i.e. more GI predominant than respiratory but the response to treatment was the same.
The unique “collection” of findings in the initial hospital presentation were as follows:
A viral phase preceding the pulmonary phase, the latter of which befell a minority of those with the initial viral syndrome, and typically becoming severe enough to need hospital for hypoxia/shortness of breath approximately 7-10 days after first symptoms. The reproducible timing of the “pulmonary phase” as I call it, was novel. We published a paper describing the timeline and characteristics of the phases in late December 2020 here.
Often presenting with “happy hypoxia” which is a clinical (i.e. observational) diagnosis not a defined mathematical one. In my career diagnosing and treating causes of acute respiratory failure/hypoxia, most patients with severe hypoxia evidence visibly obvious increased work of breathing with use of respiratory muscles, upright posture in bed, “tracheal tugging”, diaphoresis, abdominal respirations, confusion etc. An elevated respiratory rate is not what I use to define or differentiate happy hypoxia. In Covid, I kept seeing patients with moderate to severe hypoxia but without all the signs above of an elevated work of breathing. I saw so many patients whose oxygen levels and work of breathing were so obviously discordant and to me as a respiratory failure expert, I found this novel. And not only to me - early on, a number of us clinicians had debates among us as to why this was happening and it was my recall that I had only seen that kind of presentation in patients with the disease called “organizing pneumonia” or OP. Know that OP is not an infectious condition, although it can be caused or associated with infections, but its most common causes are either idiopathic or drug-induced.
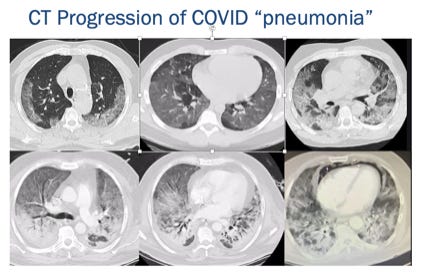
There was a pervasive “bilateral organizing pneumonia” on CT scan (OP is an uncommon finding in general and “organizing” patterns are quite differentiating amongst diseases, especially if you solely compare films on presentation to hospital, not later on the wards or ICU’s as disease progress or secondary complications develop. I compare apples with apples ( films on presentation) and not apples with oranges (film on presentation vs. film after ventilation).
To give you an example of what really happens in Covid disease, look at this progression – note the presenting and two subsequent films are classic “OP” but then, over time, you can see consolidations, nodules, traction bronchiectasis, fibrosis, and DAD/ARDS. But the presenting film in the top left was classic and reproducible:

Patients often presenting with high ferritin levels indicating severe activation of macrophages (also uncommon, but can be seen with other viruses, however, the consistency of this elevation was unique).
Patients often presented with high D-dimers, CRP, ESR (markers of inflammation and clotting). Again, these are all non-specific findings, but when appearing together, over and over, helped define this novel “syndrome”
Often presenting with high LDH and quite low lymphocytes ( this latter finding was relatively unique and highly reproducibly found in the first wave).
In the first wave especially, lots of hypo- and hyper- natremia in the ICU which perplexed the nephrologists I worked with.
Often presented with complete anosmia or ageusia (loss of smell and taste) which would then persist for weeks to months beyond the illness (this latter “persistence” I had never heard of before, typically anosmia and ageusia are transient while ill with a virus and then they return once recovered). I was in an Uber yesterday with a driver who told me he hasn’t been able to smell in 3 years since he had “Covid.”
Often rapid progression to fibrosis on CT scans - this was novel to me, I had never seen such rapidly fibrosing lung findings on CT scans in ICU patients (again, not unique as there is a rare, rapidly fibrosing lung disease called AIP (acute interstitial pneumonia) but it is very rare and does not present in the context of the syndrome above.
High rates of ME/CFS (myalgic encephalitis/chronic fatigue syndrome a.k.a Long Covid) compared to what has been described with other viruses as per this Mayo Clinic paper. Long Vax is actually more common than Long Covid and those patients are on average, sicker than Long Covid patients. Both diseases share the spike protein as the common pathogen, further supporting spikeopathy as “a thing.” Further, aside from the novelty of spike protein disease is the unfathomable complexity, this 40 page, 250 reference paper starts to scratch the surface of the innumerable now well described unique pathophysiologic mechanisms triggered by the spike protein. Spikeopathy is literally in the title of the paper.
High transmissibility with clear evidence of aerosol spread - I have never seen a disease which spread so rapidly and widely, with numerous super-spreader events, well described in the media and the CDC. Know that none of the other common respiratory viruses we see (flu, RSV, rhino, regular corona) transmit by aerosols to a significant extent (all are thought to be capable in certain discrete circumstances, but this thing was “suddenly” and pervasively airborne). I wrote on Op-Ed on aerosol spread in April 2020, first accepted by NY Times in May, then dropped, then published in USA today in July of 2020 which detailed numerous instances supporting the reality of aerosol spread. The contagiousness within families and after group events despite social distancing and masks were consistent and reproducible (even my own household saw such spreads, multiple times). The best explanation for the mis-understanding and under-emphasizing of the reality of predominance of aerosol spread can be found in the Chapter “Belief #1” in the book by Clare Craig called “Expired.”
An unusually high number of pneumothoraces and pneumomediastinum on presentation to hospital (holes in lung developed, causing air to leak out either around the lung (pneumothorax) or in the center of the chest (pneumomediastinum). Outside of someone with a chronic lung disease this is extremely rare to occur spontaneously in patients with a pre-morbid healthy lungs. When it occurs spontaneously, it typically only occurs in thin, tall young men and women and occurs idiopathically - but we were seeing a lot of them - again, very rare for a viral infection to produce a pneumothorax in native, healthy lung. However, although I saw this numerous times, it was still relatively rare amongst the total population of patients, but was far more frequent than in any other acute illness i have encountered.
Lots of deep venous thromboses and pulmonary emboli on admission or soon after admission, i.e very high rates of macro and micro clotting (microclotting, like turbo cancer are new medical terms by the way, only introduced since Covid (reversing the micro-clotting/aggregation of red blood cells is one way in which ivermectin works and has been associated with rapid improvements in oxygenation, two novel insights since Covid). Also, I have never had a case of a 29 y.o healthy male who died in the Emergency room from overwhelming right heart failure from a massive PE about 5 days into his symptoms. Nasty nasty nasty. Nor have I seen dialysis circuits where you could see the clots in the tubing as a regular occurrence (saw this in the 2nd Covid patient I encountered). Nor had I heard of such reproducible difficulty with drawing bloods or blood then clotting in the collection tubes. Again, I wrote a paper about the incidence of hypercoagulability with near zero fibrinolysis in ICU patients and I started writing that after my 4th patient. Again, this pattern can sometimes be seen in other critical illness, but it was so reproducible/identical between patients (in the first wave).
In terms of how deadly it was, this also gets complicated because the disease changed over the past few years, and despite the seemingly low Infection Fatality Rate, it is the opinion of my colleague A Midwestern Doctor that it is impossible to calculate the true IFR for influenza so a direct comparison between the two is not possible.
One other troublingly unique aspect was that in the first wave in NY, doctors and nurses were dying on the front lines. One of the first to die was an absolute giant of my specialty, he died in Seattle right after their first influx of patients. I have NEVER lost a colleague to the same disease we were treating.. ever. And I knew of at least 3 who died in the first wave of Covid. And that’s just me.
The trajectory of illness in the hospital and ICU, for me as an pulmonologist and ICU specialist was also novel in that patients with hypoxia and CT scan changes would require high fractions of oxygen initially, could breathe without distress, but then over days to a week, the lung changes would advance/worsen, distress would develop, non-invasive or invasive ventilation would then be required, and once on a vent, would require weeks before recovery or death (yes there was a minority who died fairly quickly). However, the “prolonged stability” of these patients was unique to me in that, in critical illness, once you have an advanced organ failure like heart or lung failure, the typical trajectory is patients “declare themselves” in the first 4 days of ICU, meaning they start to evince a slow or rapid deterioration or a slow or rapid improvement. But you see changes daily. However, in Covid patients, day after day very little would “budge”, either good or bad. Weird I tell you.
Again, the main thrust of my argument is that there was a constellation of symptoms and findings that presented in a novel and unique combination, it was not any one single finding that gave it its uniqueness, as there are very few “pathognomonic” findings in medicine, as in, very rare to have an abnormality that is present or specific to one disease, but this does not mean we cannot differentiate clinically amongst presenting illnesses.
That process is literally the core of what I do as a physician, I am first a “diagnostician” and true expertise in medicine is driven by very high level abilities to discern among patterns, i.e. pattern recognition, and the “pattern” of presentation of Covid was unique and easily discernable and distinct from other viral syndromes to a seasoned clinician. Yes, all ILI will have some combination of a cough, fever, head ache, sore throat, chest congestion etc… and yes, those alone are not easily differentiable, but when you bring in the timing of symptom development, context of symptom development (predictably timed after household or social exposure where others were or became ill), a combination of their initial radiographic abnormalities, lab abnormalities, initial dry lung (relatively rare in acute respiratory failure outside of asthma or COPD exacerbations), progression/trajectory of illness with progressive hypoxia and then progressing radiographically from just GGO’s to other more severe injury patterns like consolidations, response or lack of response to certain therapies, you become very familiar with what was a unique and novel syndrome.
Although I believe I addressed the main conclusions of Neil et al’s post reviewing the published literature on Covid-19, if it is helpful, and at the risk of sounding redundant, let me specifically address some of their main points in that article:
Radiologic findings cannot reliably differentiate between Covid-19, influenza like illnesses, and bacterial pneumonia.
My response: agree and disagree as above but this is NOT the only thing we used, although using radiography was super helpful in discriminating, and yes, I can say this despite the papers showing relatively equal incidences of various radiographic abnormalities overall - you are overlooking timing and stage of disease where radiography is a much better differentiator than those papers suggest).. Also, if you accept this statement on face value, it essentially would mean that radiography cannot be relied upon to differentiate among infectious illnesses. Ask any doctor and they will tell you that radiography is one of the best diagnostic tools (never perfect, but hugely impactful).
Symptoms, clinical observations (Happy Hypoxia), and laboratory findings cannot differentiate between the above illnesses either
I simply and respectfully disagree - experts have pattern recognition which easily allows for this, and pattern recognition might be better explained as “intuition”, it is almost an unconscious process when it occurs but I have been successfully relying on my pattern recognition skills to differentiate among causes of acute respiratory failure for 20 years.
Thus, there is no “proof” that a novel pathogen or syndrome existed, it was either flu, bacterial pneumonia, a toxic exposure, or widespread vaping illness
Following from the above, hundreds of thousands of doctors around the world were “fooled” into believing that this was a “new syndrome” while instead it represented illnesses long encountered throughout their collective careers, but it was the media, journals, and scare policies that made them view it as novel.
See reply to #2 above
But lets try to answer #3 above more specifically:
Why was it not the flu? Because, in my career, I have taken care of maybe 5 patients on a vent due to the flu and three of them (maybe 4?) were pregnant - over two decades and hundreds and hundreds of days running ICU’s. Flu rarely causes severe acute hypoxic respiratory failure in my experience, nor do we see hundreds of thousands of flu cases a year. With Covid, in NYC, it was difficult to run ICU’s because you would have 18-24 patients on your service all with nearly identical chest x-rays (OP initially, then progressed to consolidations and/or ARDS). I have never in my life had ICU’s full of patients with the same “disease.” This was novel.
Why was it not bacterial pneumonia? Well, from the features above, bacterial pneumonias are not associated with OP, are generally unilateral (the vast majority of Covid was bilateral), most often consolidative rather than with ground glass, accompanied by thick and/or colorful phlegm, can have pleurisy,, and when severe, typically causes severe sepsis/hypotension etc. Also, outside of TB, bacterial pneumonias do not exhibit human to human transmission so cannot explain all the transmission and dying unless someone was to argue that widespread immunosuppression developed making most of the population uniquely susceptible to bacterial pneumonia in their environment all of a sudden.
Note this was before the vaccines so I have no other possible cause of sudden immunosuppression amongst the population.. Again, bacterial pneumonias are random, relatively rare events in most people’s lives, and instead mostly tend to affect the elderly as they go into immunosenescence and/or develop swallowing difficulties.
In the young and healthy, they are very rare events. I had too many young and healthy (relatively) on vents suddenly - why/how would a bacterial pneumonia suddenly do this unless it was a new superbug which would have been quickly identified. True, people with viral illnesses can develop “secondary bacterial pneumonias” and certainly some/many Covid patients could have eventually developed a secondary bacterial pneumonia, but this is NOT what brought them to hospital in droves nor was the main cause of death. I, like Jackie, and most intensivists, would do a trial of antibiotics at the drop of a hat if there was a suggestion one was occurring (new phlegm, white count, new fever, worsening in oxygenation, new opacity on chest x-ray etc). However, despite doing this, it didn’t matter, the patients kept dying in the ICU. What I saw as the main cause of death was an initial viral induced “organizing” pneumonia (organizing patters are not associated with bacteria) which slowly led to complete lung destruction from a rapidly fibrosing process, ending up in what is called pathologically DAD (diffuse alveolar damage) and clinically is seen as ARDS (acute respiratory distress syndrome)..
Why was it not Vaping?
Vaping can be ruled out by history taking. The vast majority of patients were not vapers. Smokers and vapers make up less than 20% of the population. This syndrome spared no segment of the population and I am unaware of data showing a massive increase in the sales of vapes at that time.
Last rebuttal of a point Mike Yeadon made above:
YEADON: Separately, I’ve looked & looked and I’m unable to find in the literature good evidence of contagion in influenza like illnesses broadly. Patients with acute respiratory illnesses that are classified as Influenza-like illnesses (ILI) were unable to cause healthy people brought into contact with them to acquire symptoms of ILI. There were several experiments attempted & they were unsuccessful.
REBUTTAL: Beyond the above, I was also sent this post which compiled 67 studies where, under experimental conditions, various viral illnesses could not be transmitted to another person despite exposure to secretions, breath, live virus etc.
I have not done a literature search to find positive transmission studies, but in that list, I have to say that all of the polio studies (most were polio) should be thrown out because polio, in nearly all circumstances was not an infectious disease, the bulk of the evidence shows that it was caused by insecticide poisoning, with arsenic in the late 19th/early 20th century, and then later with DDT. However, a couple of influenza and measles studies failed which is interesting. Even more so the varicella, which I find odd, because in the little experiment that my mom did when I was sick with chicken pox as a child, she put me and my 2 brothers in the bath together, and they both got chickenpox immediately after. My mom didn’t publish that experiment though. Also, none of those viruses studied have been associated with significant aerosol transmission like Covid has. Covid is highly transmissable by aerosols. Seems contagious to me, unless some other theory of transmission or acquiring the illness can be posited. Perhaps they are all from aerosol poisonings by the sociopaths who run this world?
I apologize that I did not have the time to find published literature “proving” under experimental conditions the contagiousness of respiratory viruses. I have treated hundreds of Covid patients where, when taking a history, the vast majority can clearly pinpoint the place or event where they contracted their illness, typically along with several others, and often after finding out later that one of the guests or friends became ill after. I have seen and cared for countless family clusters and seen passage from husband to wife numerous times. I have more than a handful of simultaneous husband-wife hospital admissions (something which effectively rules out bacterial pneumonia as cause), and in a few cases, only one made it out. I have been observing non-stop contagiousness (i.e. a symptomatic Covid patient causing an asymptomatic person to then become ill with Covid). Reproducibly and predictably. I am unaware I need to find a published paper that “proves” the contagion. Further, if contagiousness of flu or ILI has not been shown to occur in published literature, then this might strengthen our argument actually - that this was a pathogen of novel transmissibility.
That’s all I got. I am not sure if I “squared the circle” in terms of making coherent sense of all the data and viewpoints and I think that is because there are still things we don’t know about how and why the virus spread the way it did and why it behaved so deadly in some spots at certain times and not others. One possible clue might be this paper finding that all? variants were created in a lab. Their concluding sentence: “The analysis showed that Omicron variants were formed by an entirely new mechanism that cannot be explained by previous biology, and knowing how the SARS-CoV-2 variants were formed prompts a reconsideration of the SARS-CoV-2 pandemic.”
*Writing this Substack is only one of my jobs, and I put a lot of work into it (at the cost of sleep and personal time). If you love this Substack and get value out of it please consider a paid subscription. Thanks, Pierre
P.P.S

Gather with like-minded people from across the world, learn from leading medical experts and health freedom advocates, meet healthcare professionals, and take charge of your health and well-being!
-Also proud to report that my book has gained Best Seller status on and off in several countries and is climbing up the U.S Amazon rankings, If any of you have bought and read the book, please leave a review on Amazon? Thanks! Link:

Thanks for this Dr Kory. I contracted the damn thing, as did many in this small rural community I live in, and while whatever-it-is may make little to no impression at population level, I believe it's too simplistic to simply write off the possibility of any pathological agent with novel characteristics whatsoever. The 'CoViD' stats are horribly confounded with fraudulent test results, but going purely on those with clinical signs and symptoms, there's enough evidence to state something out of the ordinary was circulating.
Personally, J J Couey's infectious clones hypothesis (ie. deliberate release(s) as opposed to a 'leak') strikes me as something with a lot to recommend it. It could account for the hotspots, as well as providing a possible route for integration of some novel (engineered?) characteristics within the quasi-species swarm that would appear to be implicated in normal seasonal respiratory virus morbidity. Hence many experienced nothing particularly serious, but also were able to note that something, even if indefinable, felt 'off' about it.
Great work. These are serious people making serious arguments. 1.There was a thing. 2. It was made in a lab and got out (no proof yet of intentionality). Fauci and crime brothers knew right away what it was. 3.It was serious but ultimately over-hyped and over-diagnosed. 4. Hospital protocols killed more people than the natural progression of the disease. A lot more. Boston, NY, NJ, and a few other places aggressively employed the protocols (maybe because they are surrounded by PHARMA companies and they are dominated by vindictive liberals). Iatrogenic non-care killed hundreds of thousands of patients in the US alone. 5. Every variant was man-made and individually released to sell vaccines. This leads us to the potential for intentional initial release. If they spread the variants they probably spread the initial bioweapon. Omicron was a vaccine to make the PHARMA product look efficacious. The PHARMA product failed hard and early. It was poison. The powers knew it failed in early 2021. They kept the charade going.<The objective of the international DOD/PREP response (and probably release) was to introduce MRNA technology as a panacea for the world.> Psychological motivations were pride, greed, power, control, and prestige. We dissidents stopped them.