

Can Scientific Misconduct Be Criminally Prosecuted?
MP Andrew Bridgen is convening a group of experts to present evidence of criminal corruption during Covid to the Royal Police. I want a seat at that table. Oxford's trial authors should be nervous.

In my last post, I exposed the glaring amount of evidence of extensive scientific misconduct by Oxford’s PRINCIPLE trial investigators in the ivermectin arm of their trial. Problem: outside the followers of me and those of my network on Substack and Twitter (and the FLCCC), the wider public would never be aware of the level of fraud they committed.
That just changed when an Op-Ed written by me and Paul Marik was published in RealClearPolitics last Friday. We provided a more concise litany of the fraudulent tactics deployed by Oxford. I will tell you we were a bit shocked that it got accepted, and even more so from the editor’s response: “Excellent piece.” Check it out:

Score another one for the FLCCC as it appears the public was quite interested in this topic because our Op-Ed was still leading the list of Op-Eds 4 days later:

Then, over the weekend, I came across the below article about a recent statement made by my friend and colleague, MP Andrew Bridgen, in the British Parliament:

Besides addressing his (appropriately as you will learn below) sensationalist statement, they also wrote:
“Bridgen has contacted the Commissioner of the Metropolitan Police, Mark Rowley, to organize a three hour meeting where experts and whistleblowers will lay out the evidence to prove criminal activity by the most senior members of government and civil service in the UK.”
Now, although I boasted above that I wanted “a seat at that table” because I (and others) have compiled a mountain of evidence of research fraud in the largest trials of ivermectin (see our posts on Bill Gates/Sam Bankman Fried’s TOGETHER trial, Fauci’s NIH ACTIV-6 trial, and Oxford’s PRINCIPLE trial etc).
However, I don’t think it would make a difference because unfortunately… research misconduct is not a crime (with rare exceptions). For instance, this article below from 2017 reported that between 1979 and 2015 only 39 scientists from 7 countries have been subjected to criminal sanctions for research fraud.
So, what is research misconduct? The most accepted definitions are taken from Danish law:
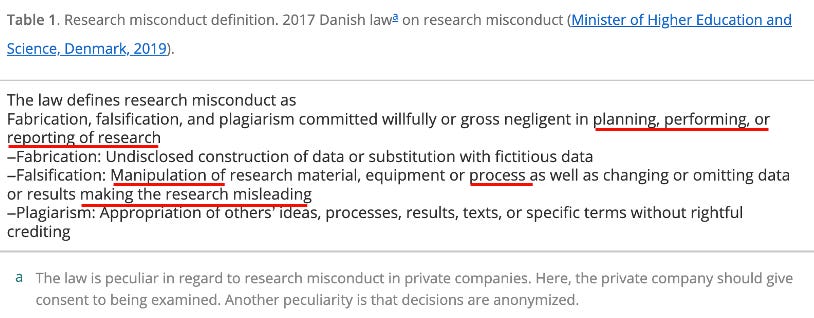
**I maintain that Oxford’s PRINCIPLE trial investigators committed all of the underlined actions above
Other classifications have also been proposed, I like this author’s in particular because he grades them in terms of severity, i.e. “Class 1 - Betrayal of the Truth:”

In the article above they discuss the fact that there have been repeated calls for such behaviors to be criminalized. They point out that although a number of countries have criminalized doping in sport but… none have criminalized cheating in science. Crazy right?
Yet, there is extensive published literature over the past 25 years that debates whether research fraud should be a crime, with many papers in favor:
But as of today, again, it is not a crime. One paper (by a federal prosecutor from Maryland (i.e. NIH territory) stated that “..the criminal prosecution of scientific research fraud is rare, if not wholly unprecedented.” Although the papers above go into somewhat erudite moral and legal arguments/theory, they also highlight the concerns and difficulty with drawing the line where scientific misconduct is criminal or not, plus they worry about both whistleblower protections as well as protections for the accused.
I am unmoved by the debate. For the past 4 years of Covid, I have, on a nearly daily basis, called out corrupt, non-scientific policies along with the immense amount of research fraud involving ivermectin. It is my opinion that the repeated scientific misconduct in the largest ivermectin trials that I described in my book, The War on Ivermectin, led to millions of deaths around the world.
When your actions directly lead to the deaths of others, knowingly or unknowingly, there are a range of criminal charges that could be brought, from negligent homicide to murder. MP Bridgen is absolutely right in going to the police. Again, although I personally do not think there is a debate as to whether the researchers directly responsible for those frauds should be criminally prosecuted, the line on exactly who should be prosecuted may be difficult to draw (in terms of who knew what and when and/or how much authority or involvement in the planning and execution that they had). I would start at the top and work my way down.
Now, if not blowing the whistle to fraud was a crime, I could see many researchers going to jail, but apparently the legal view is that unless an offense directly results in serious injury or death, the act of not reporting it is not a crime. The “directly led to” is the difficult part to prove (or not).
So how is scientific misconduct dealt with currently? It is largely handled at the university or research institution level or at the journals. People have been fired, careers have been ended, papers have been retracted, reputations of institutions have been tarnished but… no-one goes to jail. No wonder we have seen so much brazen fraud throughout Covid. The perpetrators do not have to fear prison.
Interlude: my friend and partner in the FLCCC, Professor Paul Marik, was once accused (by a jealous, competitive, well-known fellow expert in critical care medicine) of research misconduct for… get this… “self-plagiarism.” At the time, Paul did not even know what that was so he had to study the topic. With his newfound expertise, he wrote one of my all-time favorite papers of his called “Self-plagiarism: the perspective of a convicted plagiarist.” It is a hoot to read.

Now, if scientific misconduct was illegal and you could be convicted of it, the list of “crimes” perpetrated by scientists and institutions in Covid is vast. In no particular order, as I am not attempting to be comprehensive (instead I will ask my readers to suggest more examples in the comments and I will compile later), here is just a sampling of my initial stream of thoughts:
Pfizer trial research fraud (burying adverse events, dropping subjects from treatment groups for invented reasons in the interests of making the jabs look good, plus everything in whistleblower Brook Jackson’s lawsuit etc)
All of the pharma-conflicted trials with pre-determined results for early treatments like ivermectin and HCQ and ciclesonide etc. This Substack as well as those of Alexandros Marinos and Phil Harper contain a mountain of evidence of indefensible misconduct.
Public health officials lying, dismissing, distorting and refusing to release comparisons of the true hospitalization and death rates between the vaxxed and unvaxxed in order to prop up the jab campaign. As vaccine safety researcher Ed Dowd says, “you can’t hide the bodies,” and I believe there are many health ministry leaders and their underlings across the world who know this data and hide this data. They know “where the bodies are” and are universally keeping quiet about it. The New Zealand whistleblower case got a lot of attention, but I am telling you, there are many more than just him who have this knowledge. He was the only one courageous enough to make it public.
All the high impact medical journal editorial staffs rejecting and retracting wickedly positive trials of IVM and HCQ as well as negative vaccine studies
Dr. Andrew Hill’s admitting he allowed “his sponsors” to alter the content and write-up of his strikingly positive meta-analysis of ivermectin in early 2021.
Dr. Andrew Hill’s later independant publishing of a profoundly positive meta-analysis on IVM showing massive impacts on mortality with ivermectin and then self-retracting it, only to re-publish it as a negative trial? Although one of the most craven and damaging acts in history, he might be able to whip up enough arguments for his statistical chicanery to create plausible deniability, so likely no jail. I would love to be an expert witness in that trial though.
Whistleblowers have posted videos talking about numerous manufacturing safeguards and policies being ignored at Pfizer vaccine plants with safety reports being buried or workers influenced to not report. However, to hold someone criminally liable for homicide you would have to tie those violations to specific “hot lots” where huge spikes in deaths occurred. Problem: the vaccines have not caused a single death in the US according to the CDC. So there goes that one.
Fauci’s deliberate refusal to fund research into low-cost, safe, repurposed generics during the first 5 rounds and over two years of the NIH Covid trials (ACTIV program), instead throwing millions at studying only patented, high priced, Big Pharma products. Good luck prosecuting Fauci.
Again, if I spent more time, the list of criminal misconduct would fill many many pages. However, I do think there has been one trial where the actions taken do reach the level of a provable capital criminal offense. The evidence is all available right now. Today.
*If you value the time and effort I put into researching and writing my posts, support in the form of paid subscriptions would be appreciated (know that I never put any posts behind paywalls).
The scientific crime I mention above involves the hydroxychloroquine (HCQ) trials in the UK and at the WHO which directly led to the deaths of research subjects. I (and others) believe the investigators committed homicide. Although I haven’t asked Andrew Bridgen exactly what evidence he is bringing to the police, I submit that the HCQ scandal should be in there. RFK Jr. does a devastating exposure of this crime in his book, “The Real Anthony Fauci”:
Dr. Fauci, Bill Gates, and the WHO financed a cadre of research mercenaries to concoct a series of nearly 20 studies all employing fraudulent protocols deliberately designed to discredit hydroxychloroquine as unsafe. Instead of using the standard treatment dose of 400mg a day, the 17 WHO studies administered a borderline lethal daily dose starting with 2,400mg on day one and using 800mg a day thereafter in a cynical, sinister and literally homicidal crusade against hydroxychloroquine.
A team of BMGF operatives played a key role in devising and pushing through the exceptionally high dosing. They made sure that UK government RECOVERY trials on 1,000 elderly patients in over a dozen British, Welsh, Irish, and Scottish hospitals, and the UN SOLIDARITY study of 3,500 patients in 400 hospitals in 35 countries as well as additional sites in 13 countries (the REMAP-COVID) trial all use those unprecedented and dangerous doses. This was a brassy enterprise to prove chloroquine dangerous and sure enough it proved that elderly patients can die from deadly overdoses. The purpose seemed very clearly to poison the patients and blame the deaths on hydroxychloroquine says Dr. Merrill Nass, a physician, medical historian and biowarfare expert. In each of these two trials solidarity and recovery the hydroxychloroquine arm predictably had 10 to 20% more deaths than the control arm the control arm being those patients lucky enough to receive standard supportive care.
RFK Jr. then goes into who funded the RECOVERY trial (this is likely why MP Bridgen is talking to the police): the funders were the UK government, Wellcome Trust (also in the UK), and the Bill and Melinda Gates Foundation (BMGF).
He deliberately discusses the role of Bill Gates in this crime:
Gate’s fingerprints are all over this sanguinary project. Despite suspiciously missing pages, the published minutes of WHO’s part-secret March and April meetings show these medical alchemists establishing the lethal dosing of chloroquine for WHO’s SOLIDARITY clinical trial. Only four participants attended the second WHO meeting to determine the dose of hydroxychloroquine for the solidarity trial. One was Scott Miller the BMGF Senior Program Officer. The report admits that the SOLIDARITY trial used the highest dose of any recent trial. BMG’s unique dosing model for the studies deliberately overestimated the amount of HCQ necessary to achieve adequate lung tissue concentrations. The WHO report confesses “that this model is however not validated.”
Gate’s deadly deception allowed the FDA to wrongly declare that HCQ would be ineffective at safe levels. The minutes of that March 13 2020 meeting suggest that BMGF knew the proper drug dosing and the need for early administration. Yet their same researchers then participated in deliberately providing a potentially lethal dose, failing to dose by weight, missing the early window during which treatment was noted to be effective and giving the drug to subjects who were already critically ill with comorbidities that made it more likely they would not tolerate the high dose. The SOLIDARITY trial design also departed from standard protocols by collecting no safety data (Ed: What?), only whether the patient died or how many days they were hospitalized. Researchers collected no information on inhospitable complications. This strategy shielded the WHO from gathering information that could pin adverse reactions on the dose.
A masterful and deeper dive into the clear (to me) criminal, homicidal intent of the RECOVERY investigators to use a toxic dose of HCQ was written by polymath Phil Harper here. It provides even more detailed evidence of the investigator’s foreknowledge that the doses would be toxic. One of the most damning excerpts is below (there are more):
There’s also the UK database on toxic substances. Look at hydroxychloroquine and you’ll get a clear answer, “Adults who have ingested 10 mg/kg or more chloroquine base as a single dose should be referred for medical assessment“.
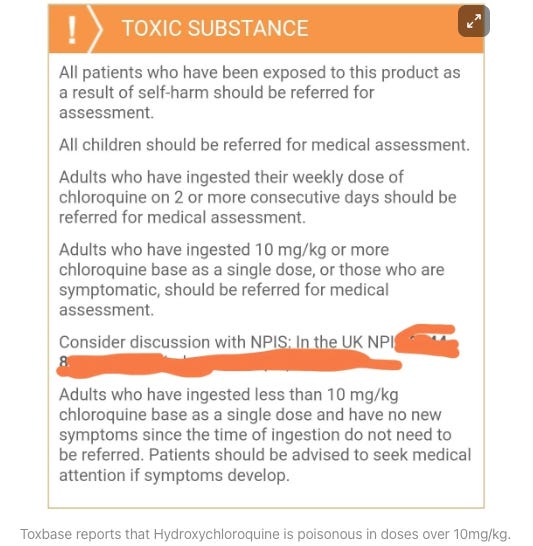
The initial dose that patient’s received on the RECOVERY trial was 620mg, which means that anyone weighing 62kg or less received a toxic dose from the first four tablets on Landray and Horby’s dosing schedule. As you can see from Figure 4 above, even though those doses were split into two 12-hour intervals, those patients received 620mg every single day for 10 days. The average weight for a woman in the UK is 70kg, which means that it’s very likely there were women in the study who weighed 62kg, and therefore, according to very clear information on toxbase, those patients recieved toxic doses.
Again borrowing from Phil Harper whose article largely relied on the excellent work of Xavier Azalbert of France Soir:
Noticing the dose seemed very large, we’re lucky to have the work of Xavier Azalbert of France Soir, upon which this article is based. His publication had the chance to interview Professor Martin Landray on June 5 at 8:00 p.m. Suspecting a problem, Azalbert asked Professor Landray about it directly, and Landray’s answer creates more questions than it answers.
France Soir: Could you specify the dosage of HCQ that you gave to the patients?Martin Landray: It is 2400mg* in the first 24 hours and 800mg* from day 2 to day 10. It is a treatment for 10 days in total. These are high enough doses to ensure that the level of HCQ in the blood is high enough to have a chance of killing the virus
France Soir: How did you decide on the HCQ dosage?
Martin Landray: The doses were chosen based on pharmacokinetic modeling and these are in line with dosages used for other diseases such as amoebic dysentery .
France Soir: Is there a maximum dosage for hydroxychloroquine in the UK?
Martin Landray: I have to check, but it's much bigger than 2400mg, I think it's six or ten times more. For Covid, there is no recommended dose because it is a new disease
Audio from the exchange extracted from the interview Landray did with France Soir. It’s available at this link.
Wow. Just wow. This guy is literally making up explanations and telling lies. Phil then looked into the “dysentery” excuse:
This is an incredible exchange. It suggests something very strange was going on with the dosing on the hydroxychloroquine trial. He’s arguing the dose is based on the treatment for amoebic dysentery, even though his own protocol says the dose is based on the treatment of acute malaria. To make matters stranger, amoebic dysentery isn’t usually treated with hydroxychloroquine, a drug called Metronidazole is used. That’s according to the UK’s NICE guidelines.
Probably a good time to note that, contrary to HCQ, ivermectin has a stunning range of safety around dosing - one study of healthy volunteers took ten times the standard dose and did fine, plus another study used 5-6 times the normal dose for 5 days and found no issues. That is why, in all the ivermectin trials, they all tried as best they could to underdose. The most absurd example was Bill Gates and Sam Bankman Fried’s TOGETHER trial where they literally started the trial studying a single dose. Yup, one day of treatment. They apparently realized this absurdity would never fly so they then changed it to 3 days. Still under dosing but whatever. Also a good time to mention this trial won the award for best clinical trial of the year:
Although the crimes above (intentional poisoning) are enough to send someone to jail, there was also violations of the Nuremberg code:
They also did not retain any consent forms from the elderly patients they were overdosing, and even allowed patients to sign consent forms in retrospect. The researchers evince their guilty knowledge by concealing the research records of the doses they used in solidarity when they filed their trial reports. They also omitted dosing numbers from the report at WHO’s meeting to determine the dose and omitted details of dosing from the WHO SOLIDARITY trial registration.
The next research crime RFK Jr. describes against hydroxychloroquine (i.e. homicide/murder of patients) comes from Brazil and is even more chilling, if that is possible:
Another group of researchers using overdose concentrations of chloroquine published their studies on a preprint in mid-April 2020 and then was quickly brought to print in the preeminent journal JAMA in this murder for hire scheme. Brazilian researchers used a dose of 1,200 mg a day for up to 10 days. According to a 2020 review of chloroquine and hydroxychloroquine it says as little as 2 to 3 grams of chloroquine may be fatal in adult patients though the most commonly reported lethal dose in adults is three to four grams. Predictably so many subjects died in the Brazilian high dose study 39% (16 of 41 of the subjects who took this dose) that the researchers had to halt the study. The subject’s mean age was only 55. Their medical records revealed EKG changes characteristic of CQ toxicity the WHO and UK trial coordinators must have known this information but they made no effort to stop their own overdose trials in order to lower the doses.
If you missed it above, please note that the paper was quickly published… in JAMA.
Lastly, RFK Jr. describes the public actions and statements made against HCQ by Fauci and Gates. These will not help them in front of a jury:
All through 2020 Bill Gates and Fauci lashed out against hydroxychloroquine every chance they got. During the early stages of the pandemic in March, Bill Gates penned an op-ed in the Washington Post and besides calling for a complete lockdown in every state along with accelerated testing and vaccine development, Gates warned that “leaders can help by not stoking rumors or panic buying. Long before the drug hydroxychloroquine was approved as emergency treatment people started hoarding it making it hard for lupus patients who needed to survive.
This was a lie - The national strategic stockpile had 63 million doses in it. I am sure Gates knew that, but am absolutely positive Fauci did.
Also about Gates and HCQ:
In July, Gates endorsed censorship of hydroxychloroquine recommendations after a video touting its efficacy against coronavirus accumulated tens of millions of views. Gates called the video “outrageous” and praised Facebook and YouTube for hastily removing it.
Anyway, the business model of Big Pharma using their money to influence researchers and journals to conduct and publish trials with predetermined conclusions would and could end if these actions were made crimes (or just significantly decrease).
It would go a long way in cleaning up science. I bet RFK Jr would support such legislation, and I know this because he once said in an interview with Dr. Drew, “On day one of my Presidency I am going to call all of the heads of the medical journals and threaten them with a RICO lawsuit if they don’t stop lying to the people.”
I believe RICO laws are appropriate given that Pharma and its journals have demonstrated a pattern of behaviors identical to a criminal enterprise near fully in control of modern biomedical science. The criminality of the pharmaceutical industry is best documented in the followins two books, the first by a former Pfizer executive, “The Whistleblower: Confession of a Healthcare Hitman” and the second is Dr. Peter Gotzsche’s “Deadly Medicines and Organized Crime: How Big Pharma Has Corrupted Healthcare.”
Similarly, I titled Chapter 25 of my book “The Editorial Mafia.” In that chapter I detailed numerous rejection letters to investigators with positive ivermectin studies and documented numerous retractions of papers by researchers which found ivermectin to be effective.
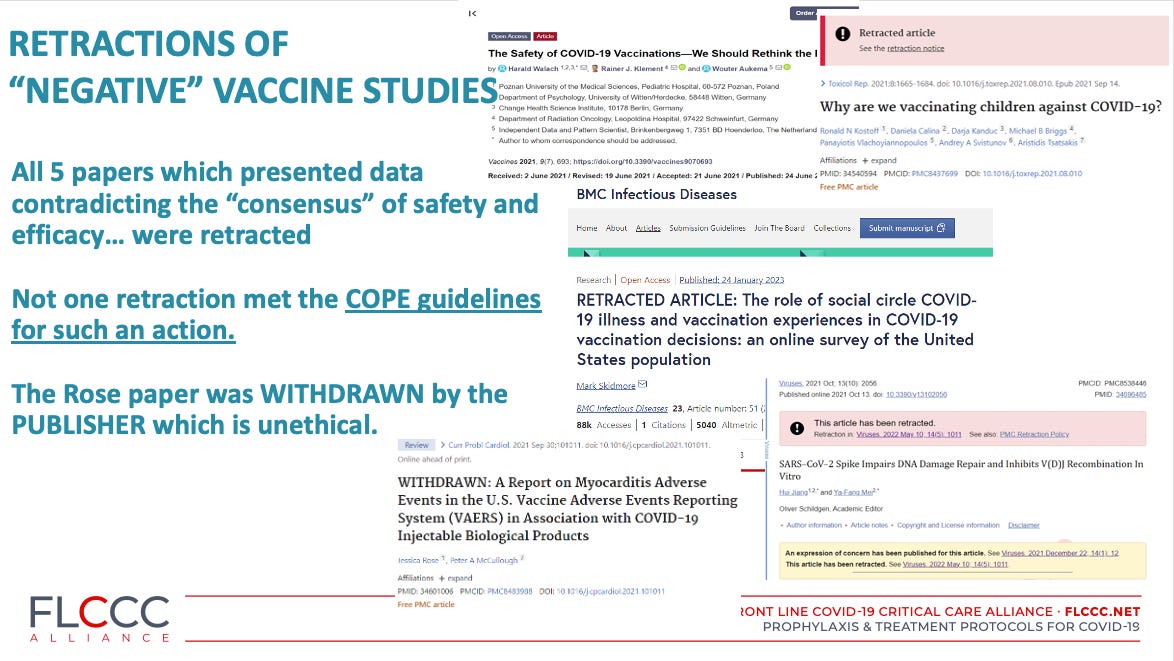
I think the Editorial Mafia’s censoring crimes around the vaccines exceed those of ivermectin. It became nearly impossible to publish any negative or concerning data around the vaccines in any top or close to the top tier journal in the world (outside case reports of adverse reactions - those, at last count were nearing 4,000 which is an absolutely unprecedented number for any medical intervention.
However, the wider reviews and analyses finding immense harm that somehow managed to get through to publication were then quickly retracted. The below retracted analyses reporting the devastating impacts of the Covid vaccines stand out (the below slide was from my testimony in the Brazilian Senate a couple of weeks ago against their universal child > 6months vaccine mandate (insane):
Most disturbing is how many Covid papers were retracted without evidence or rationale supporting a retraction:
I wonder if you can prove criminality for these “censoring” behaviors. Would be hard to prove a rejection by an editor is criminal, but maybe the baseless retractions? Discovery would be interesting - finding out who is making the calls or writing the emails to the journal editors demanding the retraction could get real interesting.
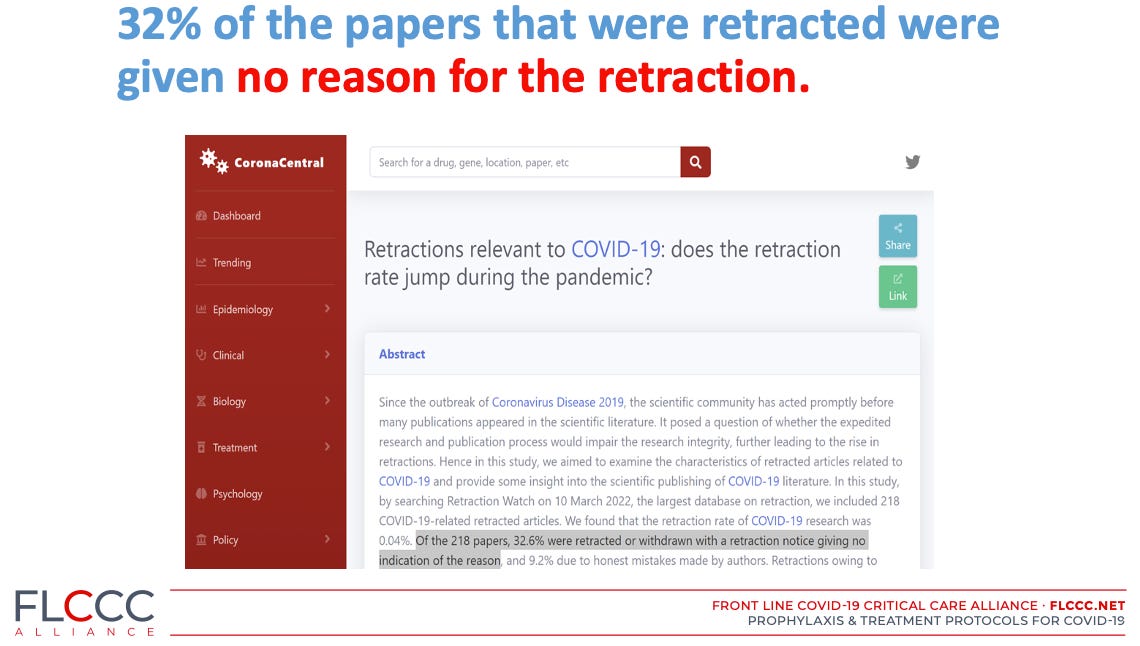
These retractions “without explanation” that occurred in Covid appear largely unprecedented in modern science. From the paper above:
According to retraction guidelines, notices of retraction should state who retracted the article and the reasons for retraction, and should be linked to the retracted articles wherever possible (4). However, our study demonstrated that nearly one-third of articles were retracted or withdrawn with retraction notices giving limited information or even without notice, and the full text was not available for over 40% of retractions.
The most devastating retraction of a vaccine review came only a few weeks ago (notice several of the authors are from my network of friends and colleagues):

It was a meticulous and comprehensive review of diverse sets and sources of vaccine related data as detailed in the abstract below. In the concluding sentence, they literally call for a global moratorium of these products. Uh-oh.
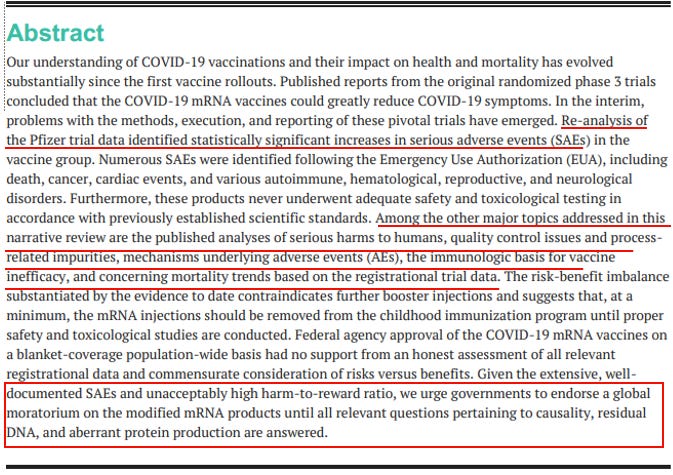
One of the authors was Steve Kirsch and his “expose” of how that retraction went down is both unsurprising and shocking. But the paper just had to go. How the hell it stayed published on-line for just over a month is the only thing surprising to me.
Anyway, to me, PRINCIPLE is the most indefensibly and brazenly fraudulent trial in all of Covid. There is just no way of defending the actions that led to the below design differences between the ivermectin trial and molnupiravir trial by the same Principal Investigator:

And that is why Paul and I wrote the Op-Ed. We are just sick to our stomach with the brazen fraud all around us in Covid science. The world needs to know what is really going on. And I applaud MP Bridgen’s efforts, I truly hope History will remember him. After Senator Ron Johnson, he more than any other politician in the world has tried to get the truth out about Covid.
I say it is time for the prosecutors, judges, and the prisons.
Our Op-Ed is below:
*If you value the time and effort I put into researching and writing my posts, support in the form of paid subscriptions would be appreciated (know that I never put any posts behind paywalls).

Four Years Later – The Toughest COVID Pill to Swallow
By Pierre Kory & Paul Marik
March 14, 2024
Looking back over the past four years, the toughest Covid pill to swallow was watching our public health institutions abandon so much of what we knew about science and medical practice to manage the pandemic. Strategies and treatments that were proven to help people boost their immune response to viral infection and fight disease were ignored and attacked. Generic drug trials were designed to fail, and investigators reported positive results as negative findings instead. They did precisely the opposite for new antiviral drugs, using every available means to claim a benefit.
The results of multi-year studies published by Oxford University shows exactly how this worked. In March 2020, Oxford started conducting a series of Covid trials with repurposed generic drugs like ivermectin and expensive new antiviral drugs like molnupiravir. For molnupiravir, for example, investigators managed to register and randomize 25,000 patients a median of two days after symptoms—a herculean effort for any clinical trial. But for ivermectin, investigators included participants up to 14 days after onset of symptoms, when the disease would have reached a more severe stage. You may recall during this time, people with Covid symptoms were recommended to stay home and isolate for two full weeks. No treatment stood a chance of making a difference after 14 days.
Efforts to tip the scales did not stop there. For the ivermectin trial, there were reported long delays between registration and enrollment, and the ability to pick-up medication from a pharmacy was stopped, forcing patients to endure notoriously slow delivery times. They also limited the days that the trial was open. These moves were clearly intended to decrease participants’ chances of receiving early treatment with ivermectin, and thus the chance it would be found effective.
Other damaging actions also raise concerns. The study authors took a full 14 months to complete the trial, far exceeding the other arms. Then they took another 600 days before publishing. To explain this delay, they claimed they needed a one year of follow-up of the patients, something not mentioned in the original study protocol. Keep in mind the backdrop of a global public health emergency that warranted $5 trillion dollars of federal government spending.
If ivermectin had been found effective, surely there was a moral and professional obligation to alert the world, as Oxford did in June 2020 upon completion of their trial on corticosteroids. At the time, the world was only three months removed from Covid’s arrival, and in desperate search of answers.
But researchers sat on the data, waiting until this month to make it available—a full 9 months after the concocted one-year delay. It first appeared not in a high impact medical journal, but in the little-known “Journal of Infection,” the seventh ranked journal of infectious diseases.
After their attempts to delay failed, they published the findings in a lower-impact outlet. The result was not the searing headlines from the New York Times (“Ivermectin Does Not Reduce Risk of Covid Hospitalization, Large Study Finds” blared the Gray Lady on March 30, 2022) but a far more muted rollout.
Even after stacking the deck, the data from the Oxford study showed ivermectin leads to faster recovery, reduced rates of hospitalization or death and reduction of long Covid symptoms. Now that the results are out, it’s clear that in addition to rigging the trials, the investigators also put a thumb on the scale in the presentation of results, minimizing ivermectin’s perceived benefit for patients and exaggerating molnupiravir. Unfortunately, it’s too little too late for millions of people. The “war on ivermectin” is over, as I argued in my book, and the truth tellers lost.
** the rest of the Op-Ed is here.
Pierre Kory, MD is President and Chief Medical Officer and Paul Marik, MD is Chief Scientific Officer at the FLCCC Alliance.
*If you value the time and effort I put into researching and writing my posts, support in the form of paid subscriptions would be appreciated (know that I never put any posts behind paywalls).
Knowingly designing treatment trials with potentially fatal doses of HCQ is the right place to start criminal investigations. Thank you Andrew Bridgen, and thank you for this clear and thorough explanation, Dr. Kory
Yes, intention is everything, the educated have the responsibility because we have command of the wisdom and knowledge. Therefore, we have the responsibility to wield it to protect and save others not infect and annihilate.
Those holding the wisdom and education to make proper informed decisions yet decide not to should they be criminally prosecuted with
((( extreme prejudice )))
We do not hesitate to persecute, prosecute, and execute for so much as a stick of bubble gum-
but for intentionally participating in the willful infliction of the illness injury and death of the general public which places there trust in us as doctors is not only unforgivable- it's diabolical!