

A Contrarian Opinion Regarding The Massive Increase In The Use of Sedatives And Opiates In UK Nursing Homes In Early 2020
Some Covid experts think that over-use of sedatives and opiates caused the increased deaths in early Covid. They even go as far as suggesting euthanasia was committed. I strongly disagree.

I am not disturbed by the data or reports of massive increases in the use of sedatives and opiates in the UK and elsewhere in early 2020. I believe people are interpreting these data malevolently, which is uncalled for and frankly, in my opinion, this shows an astounding amount of ignorance as to how those medicines are used in real life situations.
Before we get to the issue of increased use of these agents in the UK “care homes” (i.e not ICU), I think it is instructive to review what I observed in regards to their use in New York ICU’s in the Spring of 2020.
When I left the University of Wisconsin (which, like many places, was not terribly overwhelmed with Covid in Spring 2020), I did so on what I called a “humanitarian leave.” I took a leave of absence of my leadership position at UW to take over my old ICU at Beth Israel Medical Center in lower Manhattan (as a New Yorker I couldn’t stand not being on the “front lines” of my hometown during their massive “surge”). I arrived to find my old colleagues over-worked and exhausted. The hospital was running six full ICU's (there were three just prior to the surge) with four or five of them full of Covid patients on ventilators.
Now is probably a good time to address the “controversial” issue of whether hospitals were really “overwhelmed” in Spring 2020 or whether it was all just media “fear porn.” In talking to so many people throughout the pandemic, it is my belief that Covid surges were extremely variable - many places experienced only a slight uptick in admissions and ICU needs, others had empty hospitals due to people’s fear of going to the hospital or because they stayed severely locked down etc. But in New York City it was literally like a wartime catastrophe in the ICU’s. Perhaps you had to see it to believe it. But, I will agree with the naysayers that the media never showed videos and pictures of quiet ER’s and ICU’s to balance out the “chaos” the media was constantly blaring from hard-hit areas like Seattle, NYC, Detroit and New Orleans (and other densely populated urban areas). “If it bleeds it leads” but for sure it wasn’t “bleeding” everywhere. But In NYC it was hemorrhaging. Another data point that people don’t realize when they look at admission and hospital capacity data is that almost all hospitals shut down “elective surgeries” for weeks to months which are the bread and butter of a hospital’s bottom line. Thus a huge cohort of patients no longer were in the hospital because it was filled with Covid patients. So even if it “looked” like a hospital was not at capacity, this overlooks the fact that the patient population in the hospital was suddenly inverted with a massive increase in the need for ICU beds, ventilators and ICU experts. That is why I went to New York.
The patients I took over the care of when I arrived, were, as you know, not being effectively treated (because nothing was “proven” to work yet at that time, so everyone was afraid to try therapies, ugh). Further, I saw something I had never seen before outside of an ICU at Beth Israel- a separate, “regular” hospital ward full of patients on heated high-flow nasal cannulas and/or non-invasive ventilators, two devices which were, prior to Covid, almost never used outside of ICU’s for prolonged periods. The degree of respiratory distress I saw in patients outside of an ICU was unprecedented. (Remember this sentence when we get to the care home discussion).
Many of those patients were on those devices for days, on the precipice of end-stage respiratory failure. I called that floor the “Wild West.” Every shift, emergency calls to my ICU team would go out from that floor because one or more patients needed emergent intubation so they could be placed on a ventilator. Then we had to find them (or rapidly “create”) an open ICU bed to transfer them there.
In the ICU I took over, many were in late phase disease, in a condition called Acute Respiratory Distress Syndrome (ARDS) and their lung mechanics on the ventilator were severely disturbed with many in a state of what we pulmonologists call “patient-ventilator asynchrony.” Plus they had severe encephalopathy and delirium. In order to sedate them so we could synchronize them with the ventilator (i.e help them to not “fight” the ventilator, this required, for whatever physiologic reason in that first Wuhan variant, much higher doses of sedatives than what we typically used in vented patients). Unprecedented doses in fact.
I can recall one patient who needed three different high dose sedative infusions to keep them comfortable and their lungs safe/protected (and to keep them unconscious because they were also on a paralytic agent - you never want a patient conscious who is being paralyzed as it would be as distressing an acute condition as you can imagine). I had never seen a patient who required such levels of sedation to achieve this state.
We weren't trying to “kill” them using such doses, we were trying to save them. In my opinion, the massive doses of sedatives required during that time simply resulted from the widespread insufficient or non-treatment of the underlying lung disease with corticosteroids and anti-coagulants (foreshadowing - it was not from a deficiency of antibiotics).
In the below charts showing the overlapping of the excess death spikes with spikes of sedative use in the UK care homes is, to me, completely unsurprising. The main question to answer is, was it the chicken or the egg? I am making the argument that it was the increased rates of respiratory distress from Covid that led to a need for increased use of medicines to keep patients comfortable. Many/most seem to be arguing that increased use of these medicines caused all the deaths. I find this notion absolutely preposterous and trust you will too by the end of this post (if we ever get there).
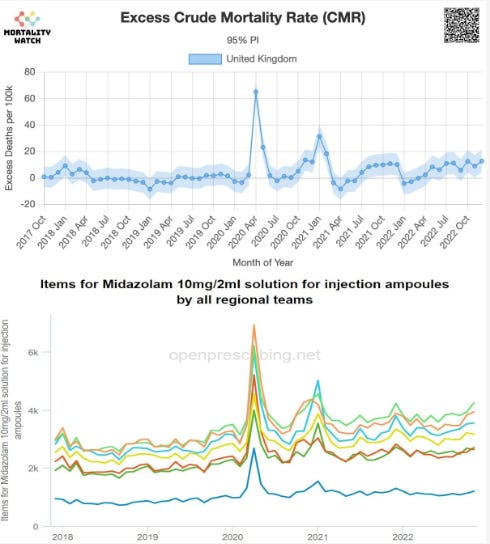
Now, although I realize that the above charts reflect care home use only, just stick with me for a bit.
In the ICU, patients with end-stage Covid ARDS on ventilators were wickedly difficult to sedate. When patients are deeply sedated, the ventilator does the work of breathing for them. So you can’t “kill” (ugh) someone on a ventilator with sedatives because the ventilator always has a back-up rate, so even if their breathing is completely suppressed, which, in those patients, we often had to do with paralyzing agent infusions but they do not die. In fact, they become much more synchronized with the ventilator and thus more comfortable and less distressed. The “synchrony” that results between the patient and ventilator helps avoid a condition called “Ventilator Induced Lung Injury.”
Life support devices like ventilators, acute dialysis, and ECMO (heart-lung support machine) are “double-edged swords” in that, yes, those interventions can and do save lives by affording patients time for their failing organs to recover. Many patients in such states will respond to treatment and their organs recover in time. But sometimes those devices simply serve to prolong dying. Thus my use of the term “double edged sword.”
Overall, depending on the ICU, despite use of these tools, an average of about 10%-20% of ICU patients will die. People die. It’s life. The machines do not make us immortal. These machines cannot “save” everyone. In those that continue to deteriorate or enter multi-organ failure, the patient becomes “irrecoverable” and enters into what I call the “actively dying” phase. Prolong the actively dying phase with life support machines means you are actually prolonging suffering. This happened a lot and was one of the reasons why I myself had a career-long “love-hate” relationship with ICU work.
Further, in patients at the end-of-life who are being removed from a ventilator to allow them to die more peacefully, it is absolutely required to sometimes use high doses of opiates and sedatives so that they experience no significant respiratory distress. Opiates are particularly well-suited for such situations since one effect of opiates is that they blunt or relieve the feeling of “dyspnea.” The definition of dyspnea is a “sensation of difficulty breathing.” In patients dying of respiratory failure, it is perfectly appropriate to use such medicines when removing them from the ventilator so they can pass comfortably without experiencing severe dyspnea, a procedure called “terminal weaning.”
My experience in the ICU I was running in Spring 2020 was that many patients were dying from irrecoverable lung injury (they hadn’t been treated!) such that they had to be terminally weaned which required even more sedation. This is actually something that I would even call “best practice.” But medicine is complex and some patients, even in advanced Covid, could stay in an advanced state of respiratory failure for prolonged periods without further deteriorating and they instead benefited from a tracheostomy (a stable and more permanent airway) with prolonged weaning at a ventilator facility. So, I am not saying that every patient on a ventilator died, but a very high proportion did while others required prolonged weaning over weeks to months in ventilator facilities.
However, once the decision has been made with the family that life support and critical care should be discontinued due to a collaborative assessment that such interventions were “prolonging suffering,” rather than providing a reasonable “opportunity for recovery”, terminal weaning is completely ethical. Our core responsibility as a physician is to relieve suffering of our patients and not to prolong their suffering and dying. The latter is what happens when life support interventions are used in inappropriate situations.
In my entire career, I was almost always physically present in the patients room during “terminal weans” to support not only the family but also the nurses in giving enough sedation (some young nurses were sometimes too timid with dosing and the patients would experience distress). Again, the goal was to allow the patient to pass comfortably without respiratory distress. This is NOT euthanasia, this is humane care of a patient at the end of their life who is suffering terminal breathlessness. We are not “killing” them, we are simply stopping a medical intervention that is failing at its purpose and doing it in as humane and comforting way possible. Everyone has the right to refuse medical care (or did before the vaccine mania, ugh) and the families were asking us to stop life support. Removing someone from life support in this way is a core skill of a palliative medicine specialist (and palliation is a core skill of an intensivist).
Okay, I am going on a tangent here, but know that NYC is a place with one of the most diverse populations in terms of cultural, ethnic, and religious backgrounds. Many different ethnicities in New York had either personal, cultural or religious beliefs which left them either unable to discontinue life support in their loved one, or their religion supposedly forbade it (I say supposedly because no religion has a precept regarding the absolute need for always providing life support in all situations, but many adherents of certain religions interpret their religious precepts in such a way).
Often, despite the extensive amounts of time I spent with families in what we called “end-of-life” discussions, the family decision maker would disagree with or simply not accept my assessment and recommendations. They would instead insist that we keep “trying.” So, in many dying patients, they would remain on life-support for days to weeks in a state of single or multi-organ failure with their heart still beating as a result of the devices. That is, until, despite all the organ support, the heart would finally somehow stop on its own. To make matters worse, in such situations, due to New York State (and many other states) laws, we were forced to do CPR unless the family agreed that it was not indicated. CPR, so you know, is indicated for acute, reversible causes of cardiac arrest and was never intended to be used in... dead people or people who are dying after weeks of what is essentially CPR (life support).. But we often were legally forced to do CPR in dead people despite our professional opinion that is was clearly not indicated. The issue of CPR laws is an ugly one to me but let’s not go there right now.
It would take an entire separate post to explore the obvious “grey areas” I am not addressing, like.. “how do you know they are irrecoverable?” Have you ever made a “mistake” in your assessment of their prognosis? The answer is that I can recall one or two cases where my assessments were proved somewhat incorrect. Why do I say somewhat? Because, in those cases, although the patients ended up recovering function to a degree that was unexpected, they still remained gravely and chronically ill. If you want to argue that had I kept all the dying patients alive for longer, I may have seen more recoveries, that is certainly a possibility and is one I struggled with emotionally throughout my career.
However, as a NY ICU doctor, I gained extensive experience providing life support to dying patients because families often insisted on it “to give them every possible chance” (I completely empathize with this sentiment). Thus, I was being forced to do exactly that due to the “families wishes.” My experience caring for hundreds and of patients in critical illness states that were beyond saving made me an expert at “pattern recognition” and thus I could get highly accurate at prognosticating. But to say we could claim 100% accuracy is delusional. However, based on these experiences, ICU physicians, especially if you practice in NYC, develop a keen sense of “futility” because, again, I provided way more futile care than I could emotionally handle at times. But keep in mind, if I had any “grey area” or uncertainty in a patient’s prognosis.. I either did not initiate an end-of-life discussion or I communicated that uncertainty to families. Period.
Weird fact: I will never forget a discussion I had with my early mentor Dr. Paul Mayo right before I left New York to start my new position at the University of Wisconsin. He told me that my life as an ICU doctor would be transformed in the Midwest because I would no longer be constantly forced by families to continue life support in the dying to the degree this occurred in New York.
He was 100% correct. I quickly discovered that end-of-life conversations were much “easier” in Wisconsin as I found that families more readily accepted my assessment that their loved one was dying. When I would explain to them the medical situation in great detail, they generally agreed and accepted my assessment and guidance. In New York, this occurred a minority of the time whereas in Wisconsin this described the majority of my end-of-life discussions.
Why is that? To be honest, I don’t really know but my two theories are that, in the Midwest, people seemed to be much more deferential and respectful of my expertise and guidance as a physician whereas in New York, many patients families challenged me and seemingly discounted (disrespected?) my experience, knowledge, and expertise. It seemed like they “knew better” than me, which certainly may have been the case in certain situations, but most of the time it was not. Another reason is that they didn’t “trust me.” Who wouldn’t trust a doctor? (I know, I know, it is a terrible joke, so sorry).
So, end-of-life discussions in New York were challenging, leading to more situations than I can count where families accused me of wanting “to kill their grandmother” or “to save the hospital money” etc. Another theory explaining the cultural difference towards death between NY and Wisconsin is that Wisconsin is more rural and more people have experiences on farms and caring for animals. Thus, they are much more attuned and knowledgeable about the “cycle of life” and thus understand that all animals, no matter how we/they have lived, will come to the end eventually, and that at some point, “it’s time.” In New York, death was a four letter word and families often wanted to fight off death, no matter how futile the medical situation was (I can tell you stories my gosh). Now you know why I said I had a “love/hate” relationship with my specialty.
Now, lets get back to “terminal weans.” One of my mentors said to me early in my career that he felt that ICU’s were the “best place to die.” One of the reasons why I came to completely agree with him is that I have had friends with parents with terminal illnesses on home hospice, with sublingual morphine and sedatives in the fridge, and even an emergency hospice nurse on site to administer the medicines during their final minutes/hours.. yet the descriptions of those deaths were quite distressing and traumatic to the family (and the patient). That is why, although we think we want to die at home peacefully, home deaths are not always so “peaceful” depending on what the patient is dying from - respiratory failure is not a pleasant way to die at home. Thus, ICU’s can, for some, be the best place to die in that we have so many resources and meds and IV’s etc. It can be accomplished in a highly organized, controlled, and even peaceful fashion whereby the patients (and the family) experience no such distress or trauma.
Now, lets get to the issue of what was happening in the UK care homes. One Substack author interpreted the problem as follows:
It seems that starting in April 2020, 10,000s of elderly were designated as “at the end of life” and euthanized with an opioid (Morphine) and benzodiazepine (Midazolam) combination.
The evidence of United Kingdom’s “Midazolam murders” in Long Term Care homes is damning. Overall, it paints a very dark picture: in the UK, it appears the elderly in Long Term Care homes were euthanized by the 10,000s in order to drive up the COVID-19 death toll in 2020.
We need whistleblowers to tell us.
Notice the interpretation that “murder” and “euthanasia” must have been committed to explain this. This is their reasoning: since lots of sedatives were used and lots of deaths were recorded this meant that health care providers must have been murdering or euthanizing people.
Whoa.
How about this reasoning instead: People in care homes/nursing homes often have what are called “advance directives” which stipulate that they do not want to be intubated and placed on a ventilator to die a slow death in an ICU at the end of their life. They stipulate this because they understand that life support interventions are not only unable to return them to some previous state of health, but mostly because ICU care in frail, elderly patients with significant co-morbidities very rarely leads to even the possibility that they can be returned to even their present diminished health status. Thus, such patients often have orders stipulating things like “do not hospitalize,” “do not intubate,” (no vent), and “do not resuscitate” (no CPR). Their own (or their families) assessment is that they are at the end of their life and instead of seeking “extraordinary measures” which will not achieve what they desire, they instead elect to die peacefully.
So, I maintain that another explanation for the increased need for opiates and sedatives is that patients were falling ill with Covid, then entering the pulmonary phase, were not being treated with corticosteroids or anti-coagulation, and thus becoming increasingly breathless with falling oxygen levels. Focusing on symptom control in these patients by using medicines to blunt what is often severe dyspnea is entirely appropriate in such situations.
Now, lets review some definitions:
Murder - The killing of another person without justification or excuse, especially the crime of killing a person with malice aforethought or with recklessness manifesting extreme indifference to the value of human life.
Euthanasia, also called mercy killing, is the act or practice of painlessly putting to death persons suffering from painful and incurable disease or incapacitating physical disorder or allowing them to die by withholding treatment or withdrawing artificial life-support measures.
Palliative care at the end-of-life: actions taken to provide comfort and support to patients who are facing the end of their life.
Let’s address murder first. I realize that the medical system has lost its way over almost all aspects of diagnosing, preventing, and treating Covid. The fraud and corruption by those in power who have used propaganda and censorship to manipulate doctor’s thoughts and actions does smack of depravity given the consequences that those actions caused. But to argue that, early in the pandemic, before the propaganda and censorship reached the heights they would eventually reach, suddenly health care providers in those homes just started to arbitrarily murder residents under their care is just not credible.
Now, what is the difference between administering medicines to euthanize someone versus administering medicines to make patients more comfortable, given that in both situations, you are using medicines which suppress the respiratory drive?
Answer: intent.
When you euthanize someone, the dosing and administration of the medicine is done with the sole purpose of ending their life. Quickly I assume (I don’t know, I have never euthanized someone).
When someone is suffering from terminal breathlessness (i.e they are approaching the end of their life) the primary intent of the medicine is to make them more comfortable, it is not to end their life. Their life is ending already, and you are trying to make that transition from life to death a more peaceful and less distressing one.
Where people get confused is that, in both cases, the opiate will suppress their breathing, so people think that, even in the latter case of providing comfort, that doctors are “hastening” death. Not true. The dose of the medicine used is titrated to the patients appearance, not their breathing or their pulse like in euthanasia. In comfort care, the doses are repeated or increased as needed until the patient is not gasping, rapidly breathing, or showing any other signs of distress like tightening of the facial muscles that suggest pain or discomfort. Typically, by the time your medicine doses achieve a state where the patient “looks comfortable”, the patient is unconscious, and yes, their respiratory rate has slowed. But they appear comfortable. Your therapeutic goal has been reached.
Question: do patients die faster in this situation? Answer: it depends. I will admit that yes, the time until the heart stops can be shorter in many cases, but again, that was NOT the intent, it is instead a secondary effect of the medicines, the primary effect was to relieve respiratory distress and make them more comfortable. Now, can it happen for instance that a nurse, after giving a few IV pushes of a medicine, does not achieve the state of comfort she is trying to, and then maybe gives a double dose as the patient is still struggling and she is trying to further relieve their continued distress. And lets say, for whatever reason, that that dose suddenly leads to a severe decrease in the patients respiratory rate, their oxygen drops, and then they die. This can happen, but it is NOT murder or euthanasia as that was NOT the intent. The nurse was trying to help someone get more comfortable at the end of their life! No nurse or doctor I have ever met (save a few serial killer documentaries I have seen), want to KNOWINGLY kill patients! Jesus man, come on!
Weird fact: I have seen a fair amount of cases where, after the morphine and sedatives are given and the patient appears more comfortable with breathing slowed… their oxygenation status actually improves.. and the dying process paradoxically lasts longer. Weird right? Why is that? Well, when patients are struggling with an increased work of breathing, this creates an oxygen demand. Once that demand is lessened from being made comfortable and their work of breathing lessens, the oxygen status improves. It takes longer for them to die, but they die comfortably. Similar with my nurse example above, you could accuse me of violating a core precept of a physician which is not to prolong dying unnecessarily. In this situation, in order to get the patient more comfortable, I used medicines which paradoxically prolonged the dying process. But they died comfortably, and the prolonged dying was a secondary effect, not a primary intent.
So, lets finish with the care home business. The other rationale for why people are suggesting murder or euthanasia was occurring is because apparently family members have reported that they “feel” that the medicines being used hastened their family members death. I am unsurprised that certain family members felt this way. Why? Because to explain all that I have explained above, is well beyond the capacity of providers in a crisis. Even in normal times, many physicians are poor communicators as they are overworked, poorly trained in communication, pressed for time, and thus often cannot explain the nuances of incredibly complex topics like care approaches at the end of life.
I promise you that if a doctor or nurse started giving doses of medications that were inappropriate or not indicated and patients started dying under their care as a result.. they would be immediately be reported by a colleague, lose their license, or even go to jail (maybe not too).. But, you cannot tell me that suddenly the whole staff of a care home collectively and simultaneously started euthanizing or murdering the residents. Not so fun fact: Although I dont know the reimbursement sources of care homes in the UK, if this happened in the U.S, all those workers would soon be out of a job. Why? An empty bed in a nursing/care home.. brings in no money. Last point - do you think providers at care homes have any experience or training in the care of the dying? They absolutely do.
Thus, I believe, on no granular direct evidence (find me a whistleblower that will change my mind), that they were doing the best they could, in a difficult situation of rapidly spreading Covid in those care homes, in frail, elderly patients that had advance directives that they were not to be hospitalized or ventilated, and, due to their age and frailty and the fact the first Wuhan variant was such a beast, were rapidly succumbing to various degrees of respiratory failure and the providers were trying to keep them comfortable in the only way they could which was to treat symptoms (no effective anti-viral or anti-inflammatory treatments were “approved” remember?).
Two more issues to address, this “vial” issue where the sedative vials only came in 5mg or 10 mg strengths or something. Who cares? Nurses and doctors know how to dilute any vial, yeesh. You draw up the vial into a syringe, then draw in saline to dilute, and you can carefully titrate to any dose you want. You are not “forced” to only give 10mg or whatever. Absurd.
The drop in antibiotic use. Yes, I am sure it is because they wanted all their residents to die of secondary bacterial pneumonia. Nonsense. It was a viral induced pneumonia, no antibacterials were indicated in the majority, and so many in care homes died from a viral pneumonia quickly, that I don’t find it that weird that total antibiotic use dropped. “Secondary bacterial pneumonia” certainly occurred, but it was relatively rare, even in the ICU! To suggest that everyone was dying of a secondary bacterial pneumonia (like in 1918 Spanish Flu where a bacterial pneumonia actually was the proximate cause of most deaths) is absurd. I would start antibiotics in the ICU any time I felt something “new” was going on, or they were getting “worse” and I couldn’t rule out a bacterial pneumonia, so I empirically treated them with antibiotics.. Didn’t matter.
Please everyone, stop interpreting these data as evidence of mass murder or mass euthanasia on the part of committed health care professionals trained in the care of the frail elderly, who were experiencing an unprecedented catastrophic situation in some places, particularly care homes. Although I have been exposed to increasing levels of depravity and absurdity in the actions of authorities in many fields and countries throughout the pandemic, the time period we are talking about is Spring 2020. Not everyone in Medicine had lost their minds… yet.
See Part 2 here for my hypothesis as to the more proximate root cause of all the deaths.
P.S I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amounts of time I spend researching and writing my posts, so again, thanks.
P.P.S. I opened a tele-health clinic with a specialized focus on the treatment of both Post-Vaccination injury and Long-Haul Covid syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.P.S. I am writing a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for:
Very disappointed in this post. "I promise you that if a doctor or nurse started giving doses of medications that were inappropriate or not indicated and patients started dying under their care as a result.. they would be immediately be reported by a colleague, lose their license, or even go to jail (maybe not too).. " Really? Are you kidding? Who wrote this? I personally know of a young family, father was hospitalized with covid in 2020, given remdesivir, ventilated, and lungs severely damaged. Doctors told the wife there was no hope, his lungs were beyond saving, that he was too weak even for a lung transplant. She fought them and many months later, he is now home breathing on his own. See the case in Vera Sherav's documentary of the girl with Down's Syndrome who was vented and doped up against her family's wishes and died. See the testimonies of many physicians and nurses who reported malpractice including starvation, lack of hydration, over sedation, inadequate monitoring, neglect, etc. ICU patients being managed by unlicensed medical students in NYC. Are you kidding? What are you talking about? You don't know what went on in the UK. And couldn't unprecedented high sedative doses also decrease and disturb all organ function, including the heart?
Thanks for this post, which gives wider context to the UK concerns. However it doesn’t address what I thought was the main concern (as reflected, eg, by John Campbell) that in the UK, the NICE guidelines issued at the time were disturbing, and appeared to be consistent with end of life practice rather than with therapeutics. The data on dosages may have been circumstantial but the directive (since withdrawn) was not. In addition, the very sudden (and short) and large mortality spikes observed were not consistent with any patterns of a spreading virus. While of course I respect your experience, and first hand accounts of NYC situation, your post doesn’t yet allay all the concerns I think.