

The Global Disinformation Campaign Against Ivermectin, "The Fix" - Chapter 2
How Dr. Andrew Hill was the world's lead researcher of repurposed drugs in COVID, turning his team's attention to a sole focus on ivermectin in November of 2020, right when I posted my review paper.

My Global Disinformation Campaign Series:
Part I - Introduction to the Disinformation Playbook
Part II - Exposing the Corrupt Disinformation Campaign on Ivermectin
Part II - Ivermectin - An Attack by New York State’s Attorney General
Part III - Ivermectin - Lawyers Helping Doctors be Doctors
Part IV - Ivermectin - Saturday Night Fight At The Pharmacy
Part IV - Ivermectin - JAMA’s “Diversion”
Part VII - Op-Ed on Fluvoxamine
Part VIII - Op-Ed on Remdesivir
Part IX - Ivermectin - “The Fix of Andrew Hill” -
Part X - “The Fix of Andrew Hill”
Picking up from Part IX where I deeply digressed into highlighting the principles of “evidence based medicine” that are infuriatingly and corruptly ignored by academia as they are manipulated into holding fast the belief that the only vehicle to discern scientific truth in clinical medicine is the often flawed, severely limited and easily corruptible prospective, multi-center, randomized, double-blind, placebo controlled trial. Let’s get back to the story here and revisit my first conversation with Dr. Andrew Hill, where we shared our “origin stories” in regards to ivermectin in COVID.
My “origin story” with ivermectin was pretty straightforward and predictable as I had learned about ivermectin’s efficacy from Professor Paul Marik (he has been ahead of me in COVID and medicine in almost all topics, always and forever.. with the rare COVID exceptions of my early insight into the data supporting aerosol transmission, my identification of organizing pneumonia as the primary condition underlying the pulmonary phase of COVID, and my detecting the massively fraudulent vaccine safety and efficacy data before him (hey Paul, I gotta keep a little “street cred” here).
But in every other realm, he has ALWAYS been ahead of me, the FLCCC, and the entire specialty of critical care as he is the most highly published practicing critical care specialist in the history of our field.
Paul did so many cool things in his and our approach to “figuring out COVID.” Even before he invited us to form the FLCCC, right around when COVID hit U.S shores, he was posting on his Medical School website (yes, the one affiliated with the Sentara Health system that just ended his career), common sense prevention and treatment protocols with over the counter vitamins, supplements and therapeutic compounds with demonstrated anti-viral and/or immunomodulatory properties to help people develop optimal immune system strength to be able to survive the disease. And from the first days of forming the FLCCC, Paul created a table of potential therapies that we followed all of the observational and randomized trials data on, the most recent version of which is below.
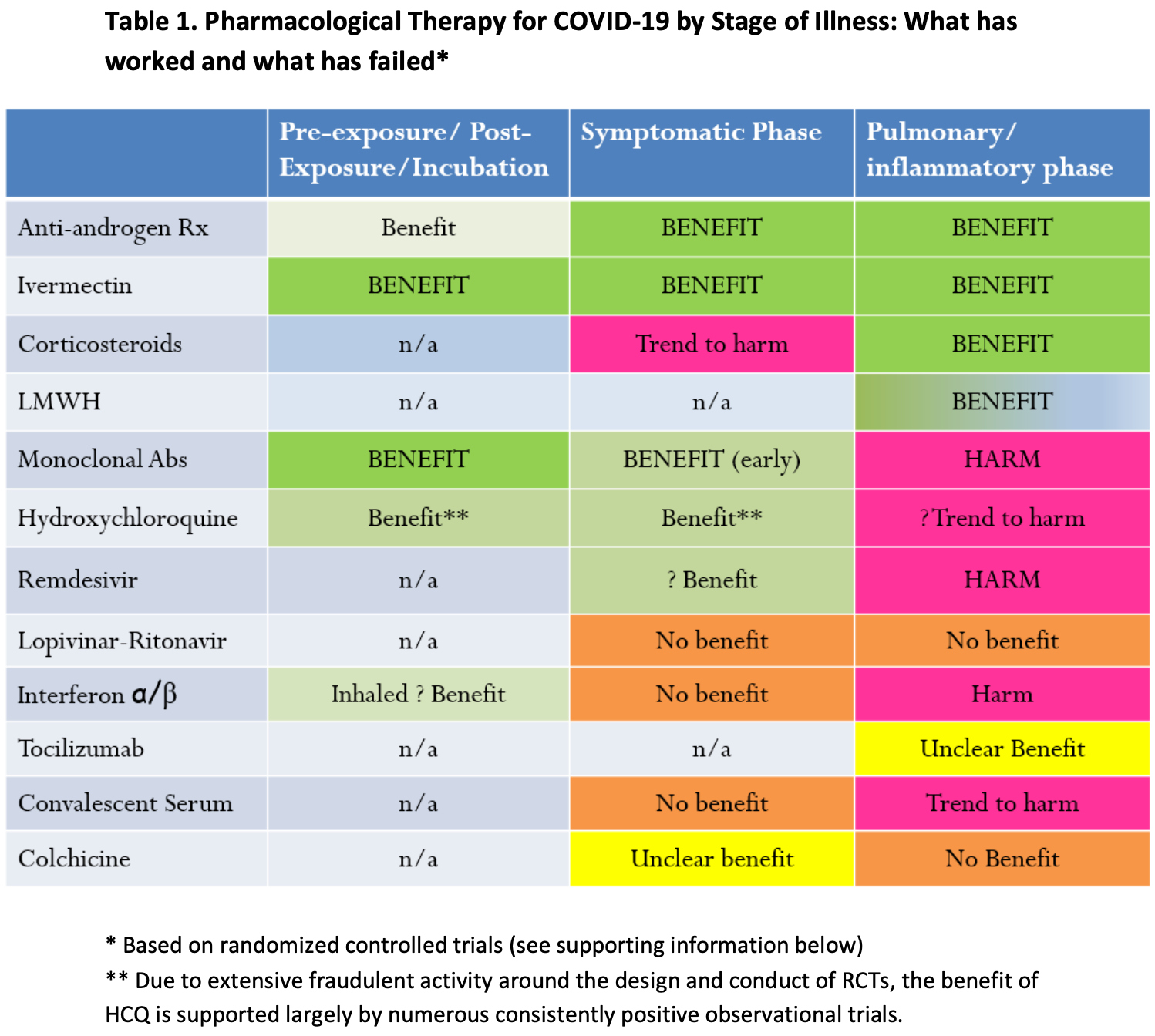
From April of 2020, after the Monash University study by Leon Caly and Kylie Wagstaff showed near complete eradication of SARS-CoV2 from a cell culture after being exposed to ivermectin, Paul had initially put ivermectin in the table with a “question mark” next to it, as we were waiting for clinical trials to emerge. And emerge they did, right around September and October of 2020 at around the same time that the first “big RCT’s” of therapies like anti-coagulants, tocilizumab, hydroxychloroquine, convalescent plasma and others were being reported (almost all were negative with the exception of anti-coagulation).
After Paul saw “a strong efficacy signal” from the first handful of clinical trial reports with large magnitude impacts on survival or hospitalization, he put together a lecture and posted it on his youtube on October 24th, 2020 (still there somehow) where he concluded it would save the world and end the pandemic. Intrigued, I immediately dove in right behind and started to read, read, read. And write write write. What I quickly discovered was exhilarating, things like ten years of in-vitro studies of ivermectin in a dozen RNA virus models where it stopped replication (Zika, Dengue, West Nile, HIV, influenza and others), in-vivo (animal) studies where ivermectin led to increased survival and decreased organ damage, large case series from a number of countries with incredible outcomes like the one by Jose Morgenstern et al in the Dominican Republic where they treated over 3300 consecutive emergency room patients.. and recorded only 16 hospitalizations and 2 deaths. Not to mention the insane safety profile of ivermectin, almost unparalleled in our armamentarium of medicines. I started to feel like it’s Nobel-Prize winning impacts on world health related to eradicating endemic and disfiguring parasitic diseases might even be surpassed by it’s newly discovered properties as one of the world’s broadest anti-viral medicines. No wonder the Nobel Prize winning discoverer of ivermectin, Professor Satoshi Omura, calls it “the wonder drug”).
Then I started finding RCT’s and OCT’s, all with positive benefits, not always statistically significant, but large enough amongst small trials where they were beyond convincing, especially when you combined them into a meta-analysis. And then I found Juan Chamie and David Scheim’s landmark paper on a pre-print server which analyzed the epidemiology of covid cases and deaths in areas of Peru that had done massive distribution campaigns of ivermectin. Chamie’s paper literally transformed me and instantly became a large part of my draft manuscript.
I was shaking as I uploaded that manuscript to a pre-print server as I literally thought the paper would alert the world to the solution to the pandemic (yeah right).
“Andy’s” origin story of how he started to focus his research on ivermectin in COVID was that he had been hired in June 2020 by UNITAID, an international health care organization funded largely by BMGF and several other countries (BMGF is also the 2nd largest funder of the WHO). UNITAID was collaborating on the ACT Accelerator program with the WHO (with this program being completely run and staffed by BMGF), and Andy was in charge of the team looking only at repurposed drugs which, at the time, I thought was phenomenal (it was what I shouted about in my Senate testimony, i.e. that our governmental health agencies were not initiating a coordinated effort to identify effective already available drugs to “repurpose” them to fight COVID, and here he was the head of the team doing just that!)
Given this background, I asked him, “How and when did you come to choose to study ivermectin?” His answer, even then, was a little suspicious, “well, we had been researching numerous medicines since June 2020 like favipiravir, hydroxychloroquine (I forget the others).. and none of them showed efficacy” (yeah right). He then said, “I was told by a Professor at my university to look into ivermectin in early November” (my review paper was uploaded on a pre-print server on November 13th). Hmm. Do you think Big Pharma scientists were monitoring pre-print servers for emerging evidence on repurposed medicines?
What you have to do here is remember the Professor. The at that point unnamed Professor’s identity will be revealed much later in this story, as he was, in my mind, the “point man” who conducted this Disinformation play distorting and suppressing the evidence of efficacy of ivermectin, however this was at the global level because it was this Professor (Andrew Owen) who was also in charge of compiling the evidence on ivermectin to the WHO, whose guidance was the most important in the world, influencing nearly every country on Earth. He thus was a key contributor to one of history’s most fraudulent documents which was the WHO’s “Updated Guideline on Ivermectin” which was published on March 31, 2021, right in the beginning of India’s Delta wave. That document and the people behind it, in particular the Professor, have contributed to millions of deaths since. If you think I am worried about being sued for defamation, I am not. For them to do so would allow a whole lot of discovery as well as the interrogation of many who were witness to or complicit in the production of that Guideline.
My manuscript was literally called, “Review of the Emerging Evidence of Ivermectin in COVID-19.” Now knowing what the investigative journalist Phil Harper has since uncovered, Andy’s initially innocuous comment that “A professor told me to look it” gives me the chills now. Let me say at the outset here that I don’t think Andy knew who and what he was working for at the time. He was just a pawn then.
We then started talking about our impressions of the accumulating clinical trials and his words were very similar to Paul Marik’s impression, something along the lines of, “this is the first time I am seeing such consistent and reproducible benefits from so many different centers and countries around the world.”
I then began to tell him about the patients I had treated like my very first patient experience of a 50-ish woman, a CEO of a health care employment agency, who called me to tell me that she had been ill for two weeks with COVID, spiking fevers every night, viciously fatigued yet with a resting heart rate in bed of 120 beats per minute. She had found mention of my review paper and had printed it out and brought it into her pulmonologist’s office to ask him whether he would prescribe it for her based on the conclusion of our review. He agreed, prescribed her ivermectin, and she described to me what happened after her first dose; “it was a Sunday evening at about 5 p.m, I took the ivermectin, and within about an hour, I felt flushed, warm, and somewhat sweaty. The symptoms passed within an hour and I was able to go to sleep, easier than I had in a while. I woke up the next morning, no fever and a heart rate of 80. I felt great.”
This was the first patient I personally knew of that was treated with ivermectin for COVID, and then by the time I first talked to Andy, I had treated over a dozen with consistent reports of some diminution or lessening of at least one important symptom within 12 hours of the first dose, things like fevers resolving, energy levels increasing, chest tightness lessening. All the patients were as equally surprised and pleased as I was. It was exhilarating to see in clinical practice what all the evidence had shown it would do (on this thought, I still have not come across any ivermectin naysayer/denier/attacker who can also claim they have treated even a single patient with ivermectin).
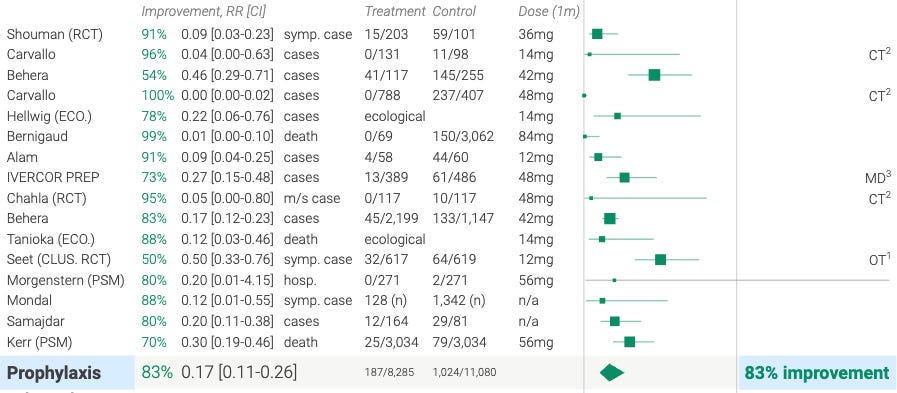
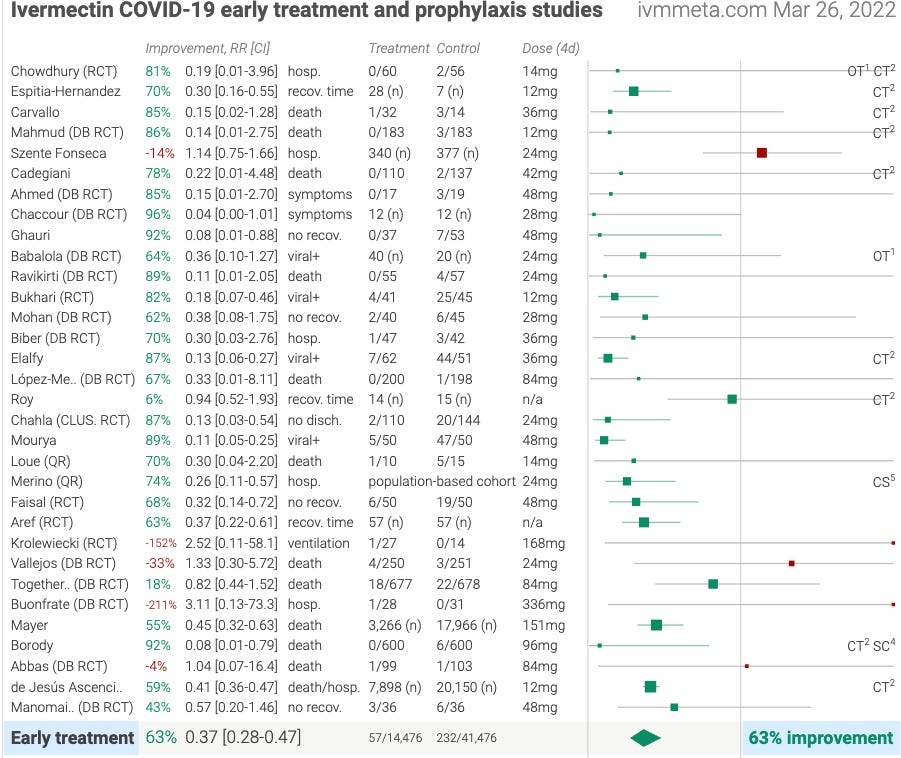
The testimonials of these patients are vast (and the first dozen or so I have put into a moving compilation here). RCT’s be damned. The patients knew what helped them and the data shows what saved them given it sits atop one of the most profound evidence bases of efficacy among almost any medicine in history in any disease model. You just do not see Forest plots like this.. ever, especially the prevention trials which are just so over-the-top astoundingly positive.
PREVENTION TRIALS
EARLY TREATMENT TRIALS
One reason why you don’t see plots with this many positive trials is that once “proven” to work after profound results from large trials or a meta-analysis of a collection of smaller trials, ethically you could no longer give a placebo because “Institutional Review Boards” (committees established in every research institution across the world to oversee the ethics of research studies) would NEVER allow them. That is, if we were in a normal world. Which we are not. To wit, the NIH continues to conduct a placebo controlled trial, using artificially short durations of ivermectin, smaller doses than the FLCCC uses, with delayed initiation of treatment etc. Absurd. And so fully indicates the regulatory capture of our agencies. It ain’t subtle folks.
Penicillin use in bacterial infection would likely have produced a similar Forest Plot (unless not dosed correctly or treatment was delayed or stopped too early etc). Read the following from David Scheim of the Chamie et al paper which analyzed the incredible impacts of Peru’s IVM distribution campaigns, where he contrasts the evidence base supporting the adoption of penicillin with what is going on with ivermectin in a more modern environment where the pharmaceutical industry controls and manipulates media, the agencies and our subservient government officials who believe what they are told etc:
Public health policy decisions regarding two proven cures of the past century provide useful lessons for decision making about COVID-19 therapeutic options. In the early 1980s, an Australian physician, Barry Marshall, found that stomach ulcers were caused by a species of bacteria, H. pylori. He developed a treatment consisting of a few weeks’ course of two oral antibiotics and bismuth that permanently cured ulcers. In 1988, he conducted a randomized, controlled clinical trial that established the efficacy of this treatment and in 2005 received the Nobel Prize for medicine for this research. Dr. Thomas Borody, also of Australia, conducted another clinical trial demonstrating 96% efficacy of such a therapy in 1990. But patients and physicians were in the habit of taking and prescribing, respectively, two best-selling palliative medications for ulcers, and the cure for H. pylori did not become widely used in clinical treatment until the late 1990s. Of related interest, Dr. Borody has become an active investigator and proponent of IVM treatment of COVID-19 (note we both admire and interact with Tom Borody as he is the Australian version of Paul Marik in terms of recognizing IVM’s efficacy in COVID, except he both gained this knowledge and went public with it before the FLCCC did.. and predictably got roundly attacked and dismissed for this opinion). In contrast to the decade-long delay in the widespread clinical application of a proven cure for stomach ulcers was the rapid deployment of penicillin for bacterial infections, escalated by the urgent battlefield needs of World War II. The first successful treatment of a patient, a 90-year old women with a streptococcal infection, using penicillin was performed in March 1942. A case series of penicillin treatments of 15 patients through oral, IV or intramuscular administration and of 157 other patients with local application was published in March 1943. With a clear record of cures for most patients and no toxicity in these and subsequent case series, production of penicillin was rapidly escalated and treatments extended to more patients limited only by supply. By June 1944, enough penicillin had been produced to treat all wounded Allied soldiers in the D-Day invasion. At no time through 1944, however, had randomized clinical trials validating the efficacy of penicillin been conducted.
I believe that my early treatment experiences with ivermectin must have been similar to the medics in World War II when they first began treating wounded soldiers with penicillin. In my case, covid patient after covid patient kept contacting me and I was calling in prescriptions all over the country, sometimes for multiple family members, and they were getting better.. quickly (albeit on occasion responses were more slow, especially after Delta came around). I also began receiving emails from a growing collection of colleagues from around the world who had been using various combinations of early treatments (most with IVM or HCQ plus other medicines).
Many had seen similar responses with hydroxychloroquine since early-mid 2020 and were now seeing even more robust responses, especially in combination. Doctors like George Fareed and Bryan Tyson, the United States early treatment pioneers, report in their book that they have done “early treatment” in over 8000 consecutive patients with COVID in their urgent care centers and offices, yet observed only a dozen or so hospitalizations and just 2 deaths (none in those treated early).
Lets now go back to December 2020: within days of my Senate testimony “going viral,” I was contacted by the Chief of Staff (and former state Commissioner of Health) of a Congressman that sits on the House committee which oversees the funding of the health agencies. He told me that Paul and I absolutely must meet with the NIH to present our data.. and that he would make that happen.
A week later, I got an email from the Coordinator of the NIH COVID treatment guidelines panel, a panel, that along with FDA and their EUA’s, and due to the CARES act which paid massive 20% bonuses on each COVID hospital bill if they used these EUA approved medicines were effectively dictating the care of every US hospitalized patient. For a 20% bonus to your bill, not giving remdesivir… would hurt the hospital. Giving ivermectin instead of remdesivir would have a large impact on the hospitals reimbursement. I did not know that then, but I was already extremely angered because this blind following of agency recommendations violated the most important sentence in the guideline, at the end of the introduction; “Finally, it is important to stress that the rated treatment recommendations in these Guidelines should not be considered mandates. The choice of what to do or not to do for an individual patient is ultimately decided by the patient and their provider.” That sentence used to define my autonomy and my practice in myriad conditions and complexities of patients who often were actively dying in my care as an ICU specialist. I was tasked and trained to save them any which way I could and had great freedoms and support in doing so. That was one of the reasons why I loved ICU work, the adrenaline, and the challenge, having to figure out, and fast, why someone was dying (hence my expertise in critical care ultrasonography, one of the greatest diagnostic tools ever wielded by front-line clinicians, heck, I made more life saving diagnoses in my first year after adopting that tool than I had in my career). Looking back, another awesome thing about ICU medicine.. is you weren’t questioned or second guessed, as you were the most expert in the hospital at resuscitating (or “re-animating”) the dying (the French intensivists call themselves “re-animators”).
I started witnessing doctors giving medicines at “this dose and this duration using only these drugs and patients were failing these bullshit protocols, as they were ignoring the responses and severity and stages of disease, all variables that would normally factor into any treatment decision. I saw docs stopping steroids because the arbitrary 10 day duration had been completed. Crazy town. Clown world. And that was 18 months ago. Many, but not all, of my colleagues practiced like this but I knew there was so much more we could do and try to turn them around, I knew the 6mg of dexamthasone was bullshit and they were dying but everyone kept following the stupid (and corrupt dose set by Oxford and propagated by the NIH - that will be another post later).
As if this insanity was not enough, suddenly hospitals started removing “controversial” medicines from their pharmacies and not filling them.. even in the dying. This blind obedience spread quickly and with little noticeable resistance in COVID, a disease I should emphasize.. which was novel. Never before in my career had I been told there was a medicine I could not use and in Paul Marik’s case of Sentara Health in Virginia (one of the more evil health systems in this regard), they removed 6 other critical medicines that we used in our FLCCC protocols, nearly all supported by combinations of RCT’s and OCT’s. Two of the more moving testimonies illustrating what it felt like as physician in such a society was the recent testimony by Paul Marik (a must watch) in Senator Johnson’s brilliant COVID: A Second Opinion panel hearing, recently and then the speech by Canadian physician Daniel Nagase during the “Remembering Nuremburg” demonstration (especially 9:00 and onwards).
It is chilling and sad and represents the plight of all the “real doctors” that valiantly tried to act out upon their insights, studied knowledge, clinical experience, clinical collaborations, knowledge of pathophysiology and pharmacologic mechanisms, and most importantly their humanity in employing risk/benefit assessments towards their deteriorating hospital patients. Everything a physician should be. I will say that many docs tried but were effectively blocked or threatened.. Those that fought back, lost jobs. Quickly.
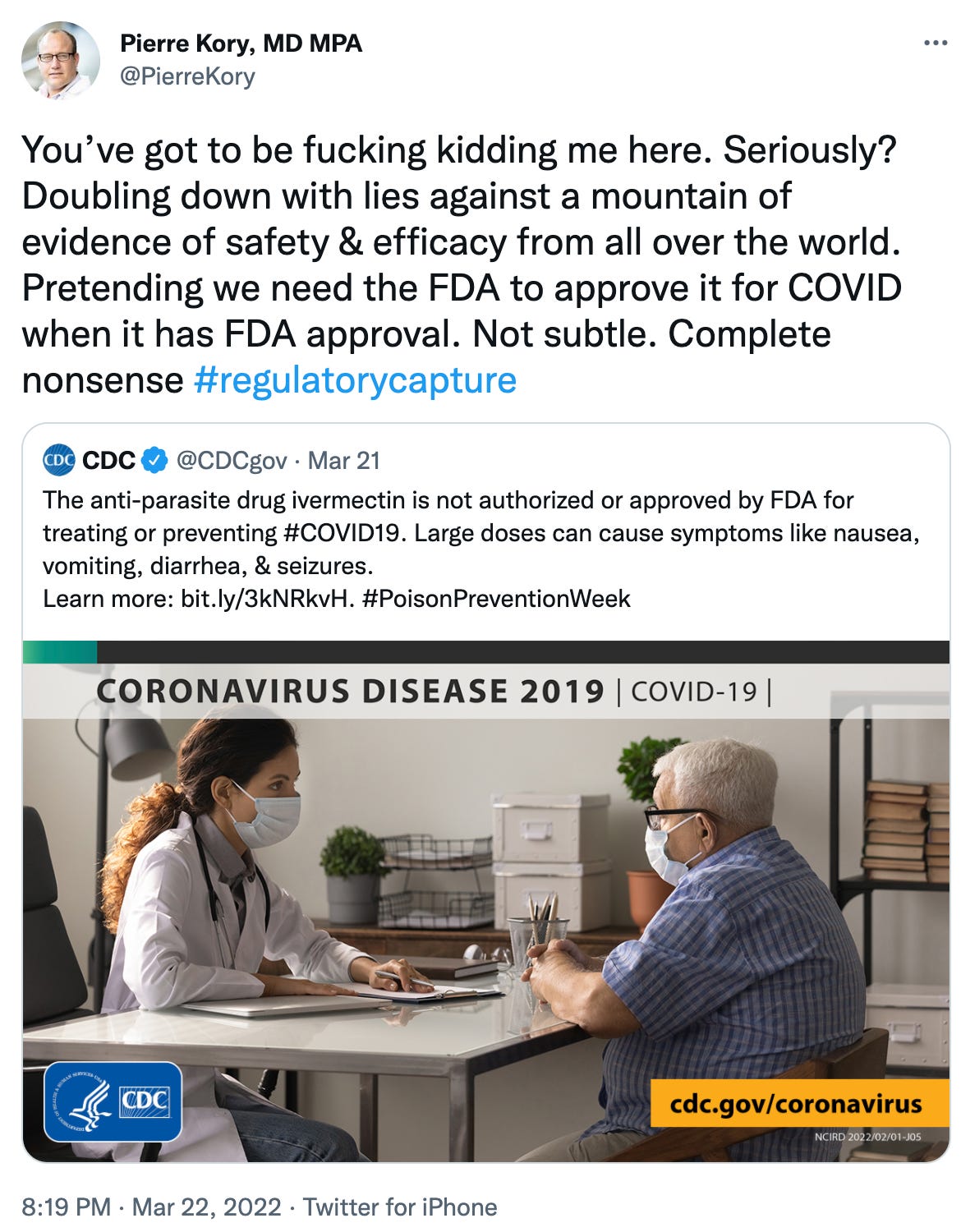
Wasn’t I supposed to be telling the story of Andrew Hill? Too many memories and emotions come flooding that I can’t stick to one topic it seems. I promise I will do better in Chapter 3 of “The Fix of Andy Hill,” coming soon. I am going to pick up where I invite Andy Hill to present his more expansive RCT data to the NIH guidelines committee with me and Paul. Little did I know that meeting was going to be my first battle between the FLCCC and “the agencies” in what is now an ongoing 15 month war with the latest salvo this little piece of idiocy below from the CDC last week (they couldn’t help going after ivermectin for #poisonprevention week). I include my retweet, using the not-so-rare but absolutely indicated f-bomb. I will say that all the comments from citizens were pretty much as damning (you guys should read them, some are hilarious).. which made me feel good to be among all of my countrymen and women who are awake. Check it out:
P.S. I just want to say how much I appreciate all the subscribers to my substack, and especially the paid ones! Your support is so greatly appreciated. Thanks my friends.
P.S.S See below for some events coming up.. plus a chance to “pre-order” my book!
March Against the Mandates.. in the heart of mandate madness (California). Please donate. Please Register. And most of all.. please SHOW UP
I am an invited speaker on the “Save A Generation Tour” in Florida at the end of April, joining many of the other renowned “Dissidents” (truth tellers). Tickets not on sale yet but waiting list is here

Hate to be hawking shit, but I am getting professional help (hah!) to write a book about what I have witnessed during COVID. Pre-order here for..


You had me on the edge of my seat with this chapter, Dr. Kory. And I see the book cover is following the same stark black-white-and-bold style of RFK Jr.‘s book, a clever approach that should prompt those readers to instantly gulp down yours, which belongs on the shelf beside it.
When you first started administering ivermectin, were you using it in combination with zinc, vitamin D, and/or other early treatment protocols, or just by itself?
On another note, I just published the culmination of two months’ work that has been described as “the best and most resource-full on the topic I’ve seen" by the cofounder of Real People’s Media, which documented the Canadian Freedom Convoy with a focus on the indigenous community:
“Profiles in Courage: The Canadian Truckers” (https://margaretannaalice.substack.com/p/profiles-in-courage-the-canadian)
I am trying to figure out how to share this article with the truckers, physician leadership, protesters, and everyone who participated in this historic demonstration of peaceful noncompliance. I know you were involved in many of the convoy events. Can you please help me get this message to the truckers so they know how much they are loved and appreciated, and most importantly, how vital their courageous actions were and remain?
Thank you, Dr. Kory, for being a truth and freedom warrior!
Dear Dr. Kory, I just want to say how much I like the way you write (and speak). Your 'dynamic expression', together with your expert knowledge, shows how deeply you care. Naturally I have pre-ordered your book. Many Thanks.