

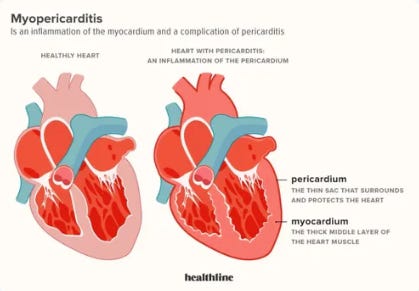
Medical Mystery: A Case Of Recurrent Myo-Pericarditis In A 20-Year-Old Unvaccinated University Athlete
Numerous "system" doctors have been unable to determine the cause of his illness. I thought it might be helpful to "crowd-source" for insights into why he is ill and keeps getting ill.

The New York Times Magazine has a long running column called “Diagnosis: Unsolved Cases” run by Dr. Lisa Sanders whereby she publishes cases of patients with varied and mystifying clusters of symptoms and then asks for readers to submit possible (or certain) diagnoses because the cases had so far “stumped” teams of expert clinicians and scientists. I saw a patient this week who met the same criteria and thought I would do the same (even though I have already arrived at what I believe is a highly confident diagnosis as to cause, I figured it would be worthwhile to ask a larger “brain trust” for their insights and differential diagnoses as to cause).
First, as an aside, some of my readers know that since well before before Covid-19, I have been a highly active Board member of the Neuroimmune Foundation, a non-profit dedicated to accelerating education and research into the diagnosis and treatment of “inflammatory brain disorders,” largely focused on the disease called “PANS” which stands for Pediatric Acute Neuropsychiatric Syndrome (a large part of PANS is caused by the “controversial” (ugh) disease called PANDAS (Pediatric Acute Neuropsychiatric Disorder Associated With Streptococcus). Founded and led by Anna Conkey (who has become one of my dearest and closest friends over the years), Neuroimmune has had major impacts into helping physicians diagnose and treat innumerable children for neuropsychiatric disorders which routinely “stump” clinicians.
I became active in that field after one of my daughters (later a 2nd daughter) fell catastrophically ill (months in an ICU) with what later was finally diagnosed as PANDAS. This only happened after 17 different encounters over months with clinicians and “experts” from major academic medical centers, emergency rooms, and psychiatric hospitals. The book “Brain on Fire: My Month of Madness” best details what we all went through. However, know that book was written by a woman with a different inflammatory brain disorder and our daughters were failed for far longer.
I am happy to say that the first daughter that fell ill fully recovered with intensive immunosuppressive and immunomodulatory therapies. When the other daughter fell ill (with literally identical symptoms), we knew what to do and fully recovered her in 6 months but she was also severely ill and incapacitated over that 6 month period.
The obstinance, arrogance, and ignorance of numerous clinicians who wrongly told me and my wife that our daughter had “anxiety” still deranges me to this day. Anxiety did not even come close to describe the symptom burden my daughter was suffering from (and we had to witness around the clock). No matter how much detail and information and insight into her illness we shared with them, the general diagnosis and response was always the same - refer to psychiatry.
At the risk of oversharing, I have PTSD from that period of my life (which overlapped with the onset of Covid) and both have impacted my health (which is getting better as some readers have commented on). Writing about that period of my life makes me uncomfortable but I think it is important to share so I am. To wit:

The picture on the right above does not even present me “at my worst” (that came later in the “depths” of my Covid journey) but it was in a white coat so I went with it. Also, I have no idea why the above is relevant to the main focus of this post except to show the stress that can happen to some people when the medical system “fails them.”
Anyway, I recall me and my wife reading the “Unsolved Cases” column years ago where Sanders presented a case of a young woman/teenager who had been deteriorating over years due to the fact that she would not and could not eat. The case was actually much more complex than just that symptom and my wife (an expert pulmonary and critical care physician and mother of two PANS children) recognized the patterns of symptoms and problems and wrote in with what proved to be the diagnosis - PANS (food restriction is a common symptom of PANS/PANDAS and helped lead to the diagnosis). Unfortunately, I could not easily find the case by searching as my memory of it is too vague.
Now, as many of my readers know, I am partners with Scott Marsland (his “Lightning Bug” Substack is amazing) in a tele-health practice called the Leading Edge Clinic which largely is specialized in the treatment of Long Vax/Long Covid (but not exclusively - we see all sorts of patients across all 50 states and even in other countries). I saw a patient this week who, similarly to my daughter, has “stumped” numerous clinicians from multiple academic centers. Here I present his case.
Another aside first: in all patients I see, I perform an extensive “history taking” whereby I collect all relevant information into what we physicians call the “history of present illness” (HPI). From Google:
The HPI is a chronological description of the development of the patient's present illness from the first sign and/or symptom or from the previous encounter to the present. The extent of history of present illness, review of systems, and past, family and/or social history that is obtained and documented is dependent upon clinical judgment and the nature of the presenting problem(s). The HPI is an integral piece of the puzzle that aids practitioners in understanding how the illness has developed over time, and piecing together and tracking the progression of these illnesses can help doctors and care providers formulate the best treatment plans based on the broader picture.
Note that the HPI is considered to be the most important diagnostic tool in all of medicine. It is considered to be the sole source of information required to arrive at a diagnosis in 80-90% of all patients presenting to physicians.
Now, on rare occasions, patients or their family members will submit a written “timeline” and/or extensively detailed history of their illness such that I do not have to personally gather extensive additional information. In the case below, the patients mother did so to such an expert extent that the amount of additional information I needed to obtain was minimal. I present her original history below, only slightly modified to add a few important pieces of information that I gathered during the initial consultation. I also changed personally identifying information and am posting this with the consent of both patient and mother. Here we go:
My son, Michael, has a diagnosis – recurrent myopericarditis - but the cause and continued symptoms are puzzling. Michael has not been Covid vaccinated.
Michael had Covid once at the very beginning of May 2021; it was VERY mild. Just over a month later in June, Michael spent a month away from home intensely training for rowing (in preparation to row at the collegiate level) and performed exceedingly well, better than he ever has. I only add this to show he clearly was NOT struggling from any lingering effects from just having had Covid (which he also confirmed). On 8/17/21, Michael woke up with chest pain, was hospitalized, and diagnosed with myopericarditis (confirmed by high troponin and cardiac MRI). He was prescribed colchicine and high-dose ibuprofen. For the next year, Michael continued to have chest pain that would get better and worse with no obvious pattern. In the summer of 2022, the chest pain seemed to get worse and stay worse, but troponin tests were coming back normal. Finally, the chest pain peaked in August 2022 when Michael woke up with numb arms, pain in his neck, and strong chest pain. This time the troponin was elevated, and he was again hospitalized with myopericarditis. The MRI showed more areas of inflammation than the first time, and Michael was placed on prednisone (for a year) in addition to the colchicine again. Although my son’s heart function, thankfully, still falls into the normal function percentage range, his heart has areas of scarring and a permanent wall-motion abnormality (likely caused by the scarring). And to this day, Michael still experiences daily chest pain, at certain times becoming quite elevated.
The cause of Michael’ acute episodes of myopericarditis is idiopathic; doctors just don’t know (Ed: definition of “idiopathic”: Of, relating to, or designating a disease having no known cause). Michael did not suffer any cold, sickness, or infection the weeks leading up to both episodes, nor was he sick at the time. Covid tests always came back negative, and my son did not receive any vaccines. Doctors ran every type of test imaginable (including a heart biopsy, which showed nothing), genetic testing, (Ed: extensive viral panels and serologies were also negative). I took my son for a second opinion to another local cardiologist here in Seattle and then another down at UCLA. I took him to the Mayo Clinic to see Dr. “Smith” who has been studying myocarditis for years and is known worldwide for his expertise. Michael is seen by a naturopath who has tested for many things. (Michael did test positive for aspergillus mold and had high antibodies to Epstein-Barre, but no one seems to think they are related to his myopericarditis. An appointment with an infectious disease doctor confirmed the same thing.) Michael has been seen by an allergist, just in case some allergen was causing an immune response leading to the myopericarditis episodes. Finally, Michael is followed regularly by a rheumatologist since his cardiologist believes the recurrent nature of the myopericarditis is indicative of immune dysregulation. My son has been on Anakinra/Kineret daily injections, but insurance finally approved Arcalyst/Rilonacept, so he is now on those weekly injections instead.
The two acute episodes of myopericarditis are very concerning for me, but I am also very worried about the chest pain that my son continues to have to this day, even almost 1-1/2 year since his last acute episode. He says it is low level baseline daily, and then it will get higher for a week, sometimes longer, and has lasted weeks and months, and then will go back to the baseline low level again. We have looked for clear patterns but haven’t seen any, although a few coincidences have made me wonder, as I will explain. My son’s girlfriend received a Covid booster shot and got quite sick with fever, aches, etc. Within 1-2 days of that Michaels’ chest pain really spiked and stayed that way for awhile. Recently Michaels’ friend and roommate had Covid. My son did not get Covid, however, he noticed his chest pain spiked. (Please note that Michaels’ cardiologist tests for troponin during these high level chest pain spikes, but they come back normal except, of course, for the two acute episodes). So, again, doctors just don’t know why the chest pain continues and goes up and down. They said, at this point, any pain caused due to remodeling of the heart from the scarring doesn’t make sense.)
I apologize for the length of this email. I can only imagine how many you receive. My son is a hard-working student who was set to row at a major University program starting the fall of 2021; his life has now completely changed. He has adjusted well and never complains, but I know the continued chest pain takes a mental toll on him. It’s not the pain itself that is wearing, but the unknown of why it’s happening and when he needs to worry that it might be another acute episode of myopericarditis. I am looking for a doctor who will look at and consider EVERYTHING, not just what he/she is ‘allowed’ to consider by the medical establishment. I am also hoping that any observational studies/similarities you may have seen in your practice might bring some answers for my son.Me:
In addition, his mother notes that since he first fell ill he has developed neuropathic symptoms in his feet. His chest pain is described as left parasternal, was constant, now comes and goes and is sharp in character. The severity of the pain has fluctuated from 2-3/10 to 7-8/10. It is present every day and is unrelated to exertion or position.Further, at the time he fell ill, he was working many shifts in a restaurant and since his illness, although he remains socially active with friends and roommates he no longer participates in any athletics. His one and a half year relationship with his girlfriend ended several months ago. He is overall better now than he has been in the past but is still consistently symptomatic.
In terms of treatments trialed for the chest pain, he was given gabapentin to no effect. His mother has wanted him to take other supplements (anti-oxidant, anti-inflammatory) but he has not been consistently adherent.
OK folks, sorry but I am putting my diagnosis as to cause behind a paywall (for a week only) because I want to give an opportunity for my subscribers to provide their own insights first. I think this may be an easy case for some and a more difficult one for others. If you need any more history or testing data, feel free to submit a question and I will try to answer.
