

Hospitalized COVID-19 Patients are Systematically Dying from Under-Treatment with Corticosteroids - PART 2
US hospitals and their doctors almost never deviate far from the standard, anemic NIH recommended dose of 6mg of dexamethasone daily. Numerous studies support far higher doses far earlier in disease.

In Part I, I began assembling the building blocks to support my argument that hospitalized COVID patients around the world, nearly all of whom have entered the “pulmonary phase” of the disease, are dying due to being systematically underdosed with corticosteroids in what is a profoundly corticosteroid responsive disease. How this continues to happen almost 2 years into the pandemic is, like many many other pandemic realities, simply unforgivable. Let’s review where we left off:
This paper by founding FLCCC member Dr. Umberto Meduri, a world expert on the use of corticosteroids in critical illness and acute respiratory distress syndrome (ARDS), found that in the best ICU studies of prior viral pandemics, corticosteroids decreased mortality by 50%.
Note that in one of the main studies he referenced, they compared different doses of corticosteroids used in viral ARDS and found that 80mg of methylprednisone daily led to the largest improvements in survival, a dose far higher than the 6mg of dexamethasone the world uses now (that dose is approximately equivalent to 32mg of methylprednisone)
This paper by founding FLCCC member me, which compiled all the evidence that COVID pneumonia is actually a rare-ish diseae called “organizing pneumonia,” (OP) and the gold standard treatment of OP is corticosteroids , and in “fulminant” cases of OP, high, “pulse doses” (i.e. sometimes equaling 1,000mg daily of methylprednisone for 3 days) are recommended.
Note that these two papers were published or being reviewed by journals in the Spring of 2020, a period marked by a widespread prohibition against their use while inexplicably high mortality rates, with frequent prolonged durations of mechanical ventilation (MV) were being reported among multiple early studies of COVID-19-associated acute respiratory failure. These reports were emanating from centers expert in such supportive care strategies. Yet, many of these same centers were literally running out of ventilators and governmental agencies started scrambling and competing to purchase huge lots of them.
In critical care medicine, I am what is known as a “vent geek,” having long ago developed an obsession with setting pressures and flows, initiating weaning , and interpreting waveforms. Further, given I was the Medical Director of the Trauma and Life Support Center at the University of Wisconsin at the time, the State Health Department had me on daily calls helping them evaluate the strengths and weaknesses of the various, often older or more basic ventilators being offered to them by vendors in large numbers.
To get a sense of how bad critical care docs were failing at keeping people off ventilators or successfully liberating them once on, one major heath system in Manhattan went from having 95 ICU beds across their 6 hospitals to 345 ICU beds in the span of two weeks (personal communication with system critical care leadership). This was all occurring in the setting of a widespread “supportive care only” strategy; meaning simple Tylenol, hydration, nutrition, and oxygen. No specific therapies were tried.. which led one major center in the New York City area to publish an 88% mortality for those on ventilators (umm.. 30% ICU mortality is considered very high). But more and more evidence supporting corticosteroids was accumulating..while critical care systems were cratering;
This remarkable study matched the inflammatory gene expression patterns induced by SARS-CoV2 in human lung tissue tissue against a database of the expression of gene suppression changes triggered by over 5,000 FDA-approved drugs.. and found methylprednisolone to be the drug with the greatest potential to revert the changes induced by COVID-19, while other closely related corticosteroids, such as dexamethasone or prednisone, were not. Methylprednisone was #1 out of over 5,000 medications. Also note this type of search for and analysis of existing therapeutics mechanisms of action allows for the rapid identification of optimal therapeutics - a powerhouse approach in a pandemic situation (and avoids the years of delay and billions of dollar needed to develop novel, high-cost, patentable drugs such as the mutagenic molnupiravir that the system is trying to shove down our throats. Just sayin’.
Observational studies reporting large impacts of corticosteroids from Detroit and Italy started to appear on pre-print servers.. and were promptly ignored beause they were not gold-standard randomized controlled trials (fun fact: on average, randomized and observation controlled trials throughout the history of modern evidence based medicine..reach the same conclusions. A known fact proven over decades, yet suppressed and fought against by Pharma who instead prefer Science to rely solely on big Pharma conducted RCT’s to “prove” something works or doesn’t.
Physicians on social media.. started to make noise. Hospitalists and intensivists started posting, largely anonymously, compelling observations and experiences, essentially crying out for doctors to start using corticosteroids at the first sign of low oxygen in COVID patients. Some memorable posts read as follows:
“We floundered for two weeks. Lots of codes, intubations and death. Maybe 15 discharges. We started steroids and discharged 250 patients. Less intubations, less codes. And the ones that ended up on vent, not as serious. CXR/CT Changes = steroids. Hypoxia on admission = steroids. Ambulatory hypoxia = steroids. Completely changed our trajectory Steroids are a game changer.” Hospitalist, SE Michigan - our group is taking care of 700 plus COVID+ patients
“I'm here in New Orleans, since we started using steroids, we were able to free ventilators and get elderly patients out of the hospital without needing a ventilator. Patients that were obviously crashing quickly, who we had to have end of life talk with were able to walk out of the hospital. At no point did any of our patient’s worsen because of steroids. These patients shed viruses 4 weeks later, with or without steroids. The virus doesn't kill anybody, it’s the inflammation that does. Let the virus replicate however slow down the inflammation”
Since this info emanated from social media and was not approved by the agencies or the journals, it pretty much met the definition of what would later be attacked as.. medical misinformation. Or were they instead valuable “reports from the front lines?” Yet the authorities continued on with their damn “supportive care only” approaches. ICU bed numbers continued to swell.. and people died. A lot. Often after weeks of being in hospital or ICU, lonely, not able to see family. Unforgettable.
I/we in the FLCCC got lucky when I was invited to testify in the U.S Senate by the Senator from Wisconsin, Ron Johnson, who chaired the Senate Committee on Homeland Security & Governmental Affairs. He decided to hold hearings as to why, in my words (and likely his too) “the doctors were not doctoring” and U.S citizens were effectively being denied treatments or attempts at treatment. Spot on really. I got the invitation because he had found the FLCCC website and protocols and noticed that one of the founders was from Wisconsin so I immediately received a phone call and invitation. Watching it again, a year and half later, I was struck about how much we knew back then about how to treat the disease and how strongly we made the argument for corticosteroids. Months before all the randomized trials (RCT). Furhter, I must point out that I every element of our protocols was incorporated many months before later having been proven in an RCT. With corticosteroids, it was not until late June 2020, when a press release announced from across the pond, that Oxford University’s RECOVERY trial, testing 6mg of dexamethasone daily, had found a small, but statistically significant reduction in mortality when used in patients on oxygen and an even larger one in patients on mechanical ventilation.
The only question that remains is.. what else have we learned about corticosteroid type, dose, or duration since the Oxford study in June of 2020? Turns out.. a lot. Check out this table I made below, and look at the column “number needed to treat (NNT)" to save a life.” The NNT is one of the most valuable measures in medicine as it indicates the potency or impact of a medicine on a certain outcome. Note that the lower the number, the higher the impact. And you can see, that higher doses, especially of methylprednisone (shocker) are FAR superior than using 6mg of dexamethasone. Over and over, by comparing studies side by side, or head to head (bottom rows), methylprednisone, at higher doses, consistently leads to many more lives saved. Especially when started early in the hospital.
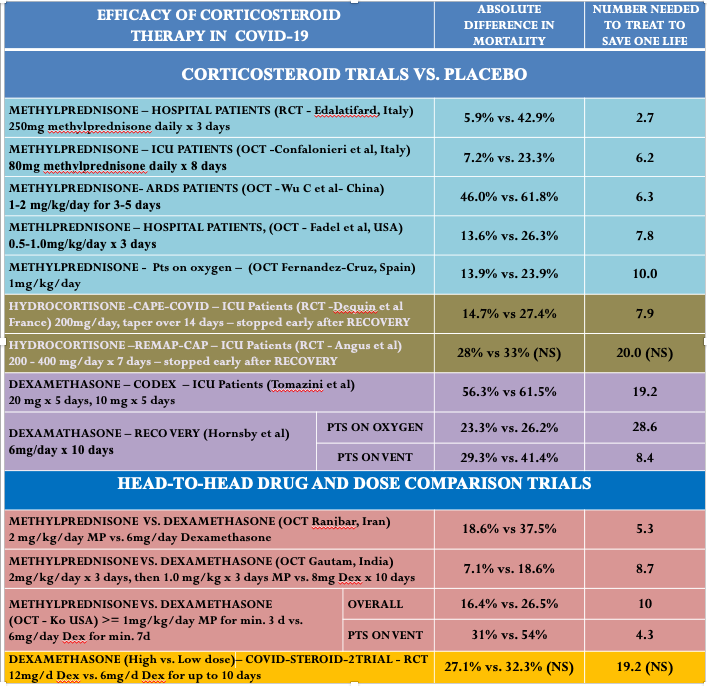
The trial from Iran by Edalitifard (first row) is by far the most impressive. They gave 250mg of methylprednisone for three days to patients in the “early pulmonary phase,” before they required intubation and mechanical ventilation. They reported a massive mortality benefit with an NNT of 2.7. Meaning that for every three patients you treated with that dose and drug, one life would be saved compared to if you had not done so. This is a massive effect in medicine. Of note, when you perform electrical defibrillation of a patient dying from a malignant arrhythmia like ventricular fibrillation, that has an NNT to save a life of… 2.5. So, giving a COVID patient early “pulses” of 250 mg of methylprednisone is akin to defibrillating someone out of a life-threatening ventricular arrhythmia? Wow. Yet the world continues giving 6mg of dexamethasone daily.. which has an NNT somewhere between 8-29.
As an intensivist who has known this data for over a year, has worked in ICU’s in 5 different hospitals around the country, has repeatedly begged my hospitalist colleagues (the docs caring for the patients before they crash into ICU’s) to be more aggressive with corticosteroids so as to avoid deterioration and needless death, I have rarely succeeded in getting my colleagues to change their corticosteroid dosing practices (they are seemingly all waiting for this recommendation to be incorporated into a guideline handed down from the “gods of science and knowledge” in Washington). Unreal..except it’s not. I have been watching needless death all around for so long… I am almost used to it. Almost.
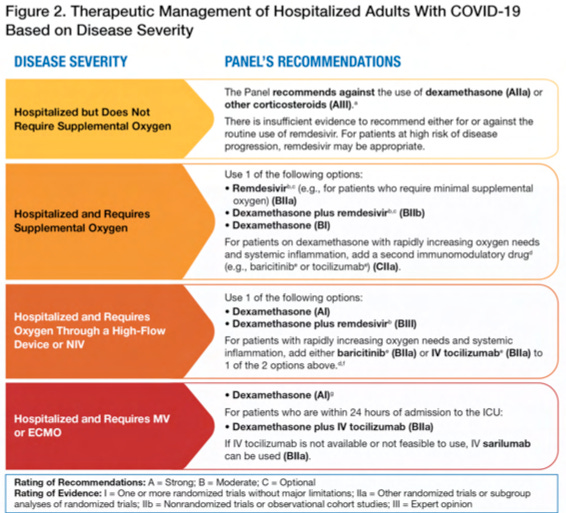
You want to know what is even worse about all this insanity? It’s that I truly believe the hand of Pharma influenced the design of Oxford’s RECOVERY trial. I am now convinced they purposely used a low dose of corticosteroid, knowing that the massive efficacy of higher doses would obviate the need for more expensive, on-patent anti-inflammatory therapeutics, i.e the “ibs and abs” that they pair the anemic dose of dexamethasone with (i.e. tocilizumab, baricitinib, and sarilumab). Too cynical? Me? Never. Like Bret Weinstein said to me a while back, “every time I think I am being too cynical, it invariably turns out I am being naive.” The United States National Institutes of Health COVID-19 treatment guidelines are below. Read ‘em and weep. But like, really weep. Weep like all the American families have over their lost loved ones, all fucking 800,000 of ‘em.
Excellent presentation! I love the analogy of high dose “shock” steroids to defibrillating v-fib! The NIH COVID treatment guidelines is evidence of crimes against humanity as far as I’m concerned. See you in DC!
Took my husband to ER twice day 9 and 11 of covid. O2 fluctuating 89-92%. 54 yrs old good health. They refused to treat him until consistently under 90% and they told me "gasping" Criminal in my opinion. I took him to a town an hour away where I heard of a group of doctors treating patients for covid. They started IV steroid and zpak. He was better next day. Finished tapering dose of pred and zpak. This was in Oregon. I don't understand why they wouldn't treat him at hospital. We are not vaccinated and I want to believe that wasn't why but I don't know.