

Establishing "Standards of Care" in Medicine - Part 2
A largely autobiographical journey down memory lane of my prematurely ended academic career.

In Part 1, I recounted my somewhat prolonged, arduous path into medical school and then through residency and fellowship training. In this post, I continue to glowingly :) trace my career to the present.
Anyway, after I completed my training, I took a position as a clinician-educator at the teaching hospital where I had done my subspecialty fellowship training in (Beth Israel Medical Center in lower Manhattan). It is always an honor when those who trained you.. end up hiring you as a partner. Picture of me when I joined the Pulmonary and Critical Care Division in 2008 :). Little slimmer it looks like.
Anyway, fast forwarding, the proudest achievements in my career as a “clinician-educator” was becoming one of the youngest Program Directors (PD) of a Pulmonary and Critical Care Fellowship Training Program in the country (I took over in my 4th year as an Attending (requirements are that you need at least 5 years for such positions). Although I was officially an “Associate” PD, I was literally the PD. Next were the winning of Departmental Teaching Awards at every academic medical center I worked for. However, what I am most proud of was helping pioneer two different, then novel fields of my specialty - the first was on the study and application of therapeutic hypothermia in post cardiac arrest patients and the other was in creating and teaching a novel diagnostic approach to critical illness using “point-of-care ultrasonography.”
My interest in therapeutic hypothermia developed early on, and stemmed from a case of a patient who had suffered cardiac arrest on one of the hospital wards. We successfully resuscitated and brought him back to the ICU but, as is typical, he remained in a dense coma with little detectable brain function. The downtime of the arrest was almost 30 minutes which is not good prognostically. My mentor, Paul Mayo, told me that we should “cool” him (to cool his brain). I asked why and he replied that he had seen some papers on it and that the Europeans were starting to do this to comatose post-arrest patients. So we cooled him, and three days later… he regained full consciousness. Moved by this clinical experience, I dove in and started researching everything that was known about the therapy.
This was actually when I was still a fellow still in training, and represents the first clinical initiative that I ever led. I created and instituted my hospitals first therapeutic hypothermia protocol and, as a result, I quickly became a regional and national expert in the therapy and started giving lectures everywhere. I was one of the expert panel members that helped develop NYC’s “Project Hypothermia,” where, when we started, my hospital was the only one out of the 46 NYC area hospitals that had a hypothermia protocol. Within a few years such protocols had been implemented at every NYC hospital and all ambulances and paramedics were equipped and trained to start cooling post-cardiac arrest patients. I did research studies trying to find which patients benefitted most or not at all, and on whether the speed or depth of cooling mattered etc (I was the first to do a controlled study on in-hospital cardiac arrest patients and I also published on rapidity of cooling using numerous techniques).
In the beginning, me and Paul Mayo thought that the faster we got patients temperatures down, better outcomes would result (although we knew it was safe, we later found out this was not true). But, at the time, thinking speed was critical to their survival, we adopted an aggressive, rapid-cooling protocol which we “borrowed” from techniques used to cool Muslim pilgrims suffering heat stroke during their annual pilgrimage to Mecca.
The pilgrims would be whisked into treatment units where they were disrobed, placed into hammocks, and exposed to high speed fans while being sprayed with warm water. Why warm water? Well, if you cover them with warm water under high speed fanning the water evaporates faster and this evaporative process sucks heat from the body much faster than if you used cold water (cold water causes the surface blood vessels to constrict, thus paradoxically trapping heat).
Paul had used the same technique to cool some construction worker that had suffered severe heat stroke the summer before, so we employed the same method to cool our cardiac arrest patients. Anytime we admitted a post-cardiac arrest patient, my entire ICU team would wheel in this huge industrial fan which we placed at the foot of the bed, then we would strip the patient naked and doctors would dip towels in lukewarm water and “paint” the patient with the wet towels under a super loud fan which emitted a terrific racket. At the same time, we would cool bags of saline fluids and infuse them under pressure through large IV catheters in the neck or groin, sometimes getting 2 liters of iced saline into them in ten minutes using a pressure bag. Lastly, we would have two doctors do iced gastric lavages by placing a nasogastric tube and, using a comically large syringe, they would push iced water down the tube into the stomach. We would install 500ml and then suck it out, then refill with iced saline, repeat. Using this “combination therapy” protocol, we achieved some of the fastest decreases in body temperature of any method known. It was wild. One problem is that it created a colossal mess with puddles of water all around the bed and folks slipping etc.
The sloppiness of the method was becoming a problem, plus it was massively labor intensive while trying to care for 16-20 critically ill patients a day. As the leader of the hypothermia program, my hospital asked me to choose a cooling device to purchase for use in patients that was a little less chaotic, labor intensive, and messy. There were a number of cooling devices on the market.. and I chose the one that was fastest. This was the device, called the “Thermosuit” which was literally an inflatable bathtub.

Basically, you unrolled this sheet of plastic on the bed, placed the patient in the middle, and then you inflated it. Once the bathtub was fully inflated, you put a plastic cover over them, attached the tub via hoses to a large reservoir of iced water, and a pump would propel the ice water into the bathtub via tiny holes in the top sheet which sprayed the entire body almost like a fine sprinkler.

Problem: it was glitchy. We would have different “failures” in the process every few times we used it. My fellows were starting to complain when they had to cool a patient because it was rarely a turn-key process. And then one day an incident occurred after which we never used it again. A code brown (which is different than a code blue as you will learn). And it was a big code brown. If you don’t know what I am talking about, basically, while cooling this one comatose patient, their physiologic response was to have a massive, very watery bowel movement. In the tub. Then, while trying to transfer the patient out of the tub, apparently the tub partly deflated and a river of brown spilled over the sides of the bed and all over the floor (and some of the staff). I was not there at the time.. but the fellow and nurses that were on that night never let me forget about it.
Fun Fact: Joe Varon, one of the other founders of the FLCCC, was an even earlier “hypothermiac” in our specialty. I didn’t know him then, but I came across this picture early on in my career and I used to have a slide with it in my lectures. It was of Joe. Check out his method. Not as elegant as mine for sure. Go FLCCC!

After the infamous “code brown” incident, I very quickly petitioned for purchase of a more practical, easy to use device (plus by this time, I had learned that speed of cooling was less important than duration). So we very quickly purchased cooling pads like the ones below, never again using the Thermosuit. See? We evolve with data and clinical experience, setting new “standards of care” along the way :).

Ultimately, as more and more studies were done, my interests and expertise in therapeutic hypothermia waned as I discovered that it was largely beneficial mostly in witnessed out-of-hospital cardiac arrest patients of primary cardiac causes and not in my general ICU patients. Then studies showed that cooling such patients was less important than simply preventing rises in temperature, so now cooling approaches are more reactive than pro-active and essentially target normothermia. However, it was a great early experience in my career.
The next major contribution of my career was when I became one of the world experts that helped pioneer the development and teaching of “point-of-care ultrasonography” (POCUS). POCUS is the use of ultrasound by physicians at the bedside (at the “point-of-care”) to image internal organs in real time so as to make rapid, accurate, and often life-saving diagnoses in patients, with its greatest impacts in the critically ill. The reason why the impacts were greatest in critically ill patients is because.. the timeliness of both diagnosis and treatment in those patients are absolutely critical to their survival. An accurate diagnosis arrived at in a delayed fashion makes it too late to impact their clinical trajectory. A wrong diagnosis and treatment early on could seal their fate.
With the advent of POCUS, no longer did we have to wait for all of the following to be done after entering an order for an ultrasound exam:
Wait for an ultrasonographer to come and perform the study
Wait for the ultrasonographer to painstakingly acquire images using an imaging protocol which assessed numerous variables that were irrelevant to the clinical questions important to saving the life of the patient (but allowed for maximal reimbursement). These “comprehensive” exams took way more time than the “focused” exams we later created.
Wait for the ultrasonographer to send the images to a radiologist
Wait for the radiologist to put the study on their worklist of images to interpret
Wait for the radiologist to, in not-due time, interpret and write a formal report which would then, in not-due time, be sent to us, the ordering physician, many hours later.
The “old way” was a painstaking process that would occur while the treating physician would be sweating it out at the bedside, trying to figure out what to do next because our patients were often deteriorating to the point of near death of a suspected but not truly known cause.
Know this: physical exam findings - palpation and auscultation using hands and the stethoscope (invented in 1811) are extremely limited in determining the proximate cause of a life-threatening illness. As a doctor of the dying, you need to know the real time functioning of the most critical organs sustaining life, i.e. the heart, lung, liver, kidneys, intestines, and large blood vessels. Blood tests are sometimes revealing of the abnormality but not necessarily of the cause. Physical examination will give you clues but rarely the definitive answer.
With an ultrasound probe in your hand, you could literally image the entire contours and function of all those organs and the information gained could lead you to initiate targeted therapies to reverse the respective organ failure detected.
Just ask Winaka the orangutan (recall her from this post):

Anyway, instead of trying to send an unstable patient to a CT scanner or attempt to order multiple different organ ultrasound exams at the same time (which could and never would be done at the same time, or even on the same day, largely because each type of exam would require an ultrasonographer from a different service, (i.e. a lower leg exam for a clot, an echo (heart) exam, lung exam, and abdominal exam). Now, within minutes, I could do rapid surveys of the function of multiple organs, with immediate interpretation and application of findings. At two in the morning in some corner room of the hospital where a patient was deteriorating before my eyes.
Here is one example of the heart ultrasound of a patient I was called to see on the medical ward who was suddenly breathless and in shock (low blood pressure, cool and clammy extremities).
What you are looking at is the heart apex at the top of the screen, however the “black area” surrounding the heart represents a large amount of fluid within the pericardial sac such that it was compressing the right side of the heart (left side of screen) so little blood was getting pumped out. We rushed him to the ICU and put a drainage catheter through his ribs (using ultrasound).. and he instantly felt better. I have tons of cool cases like this but will leave off for now.
POCUS was absolutely magical in the type and amount and speed of information that it gave you. I discovered this “magic” early on in my career.. and could not believe that the entire country and world of ICU doctors were not utilizing this technology in directing the care of their patients. I had tons of colleagues who, after relying on traditional methods of observation and intuition and reasoning (which were highly variable), would sign out their service to me on a Sunday night (ICU docs typically run the ICU for a week a time and would switch on Monday mornings). I would then come in on Monday and discover abnormalities they had not been aware of. It was absolutely frightening, knowing that the average doctor was relying on imperfect information while I had access to highly accurate, real-time and often treatment-changing information. Little did I know then, but for the next 15 years, I would devote my career to teaching doctors across the country and world in how to use ultrasound in the care of the critically ill patient.
But, when I began, I knew very little obviously. I had to make myself expert in the skills of “image acquisition” and “image interpretation.” Meaning, I had to gain the skills of both an ultrasonographer and a radiologist. In the U.S and many other countries, this skill is never taught to non-radiologists, so I was forced to learn the skill largely on my own. An auto-didact if you will. Because, aside from my mentor Dr. Paul Mayo, there were so few ICU medicine practitioners who knew how to create ultrasound images in real time and interpret them accurately.
So Paul Mayo taught me everything he knew about ultrasound before he left to take a position at a different hospital, first showing me the basics of acquiring and interpreting images of normal and diseased organs. But get this, he himself learned ultrasound from a German intern. In Germany, ultrasound image acquisition and interpretation was a standard part of a doctor’s medical training, starting in medical school. Although the average level of skill among the young doctors was quite low, the concept was highly valued (but not yet in the U.S).
I do not think anyone outside of Medicine can understand the uniqueness of what Paul did with ultrasound. Paul was a Professor and the Director of an ICU in a major metropolitan center while an intern trained in Germany started telling him that if you learned to use ultrasound you could quickly find out a lot of things about a patient. If their lungs were dry or wet, if their gallbladder was inflamed, if their heart was functioning, and if not, which part of their heart was not functioning, if they had blood clots in their veins etc. The amount of detailed and specific information you could acquire within seconds to minutes was incredible. And the specificity of the information blew away the often in-accuracy or non-specificity of chest x-rays.
To his historic credit, Paul Mayo listened to this intern. He started an “ultrasound club” where he would take an afternoon each week to practice image acquisition with the intern and any others that were interested. After learning what he could from that intern, Paul then reached out to his Cardiology colleagues and started going down to the Echo lab reading room to interpret cardiology exams with the experts. He even got them to teach him trans-esophageal cardiac echo (much more complex and invasive). Then Paul and his senior fellow at the time, Adolfo Kaplan, became one of the nations first non-cardiologists to pass the National Board of Echocardiography exam in the year 2000, one of the hardest exams among all specialty exams (65% passing rate even amongst cardiologists!). I later joined that elite group when I too passed the exam by one question in 2008.
Paul then became colleagues with the true pioneers in the field which were the French. Fun fact as to why: in the U.S, almost all intensivists are pulmonologists, in much of Europe most intensivists are anesthesiologists, but in France, most of them are cardiologists. Cardiologists knew how to use ultrasound because that is the primary imaging modality of the heart. So, in the ICU, they started using their ultrasound machines to look at other organs and thus they literally invented the field. Through Paul Mayo, I was able to interact and learn from them on a regular basis. Another fun fact: in France, they call ICU doctors “re-animators,” i.e. the act of bringing life back to the lifeless.
Now, the true pioneer and world-expert leader of POCUS among the french intensivists was Dr. Daniel Lichtenstein, a savant in the deepest sense of the word. Paul ended up becoming close friends and colleagues with Daniel. I read his seminal textbook maybe 6 times, ingesting every word. One early honor in my career was when, as a fellow still in training, I gave a lecture at a conference right before his keynote lecture.
Some of the the most memorable care experiences were when I was faced with a patient dying of either multi-organ or single organ failure, and I did not know why. It is really humbling when you are the most senior doctor in the ICU and the entire team of trainees, nurses, consulting physicians (and families!) are looking to you to provide the diagnosis and guide an effective treatment plan and you don’t know what is wrong or what exactly to do.
I hate saying this, but many doctors in such situations start barking orders.. as if they knew exactly what they were doing. They literally embody the adage of “don’t just stand there, do something.” The appearance of doing something made it seem like they knew what they were doing. No-one asked the doctor why they wanted to order this test or this medication, as everyone just assumed they had a reason and they knew what they were doing. But I could see that sometimes they were lost and essentially flailing to find some solid data to guide them as to what to do next. I get it, been there.
I found that as I gained experience in critical care, when I was in those situations, I started doing the opposite. I became quiet and allowed my mind to race through the numerous diagnostic possibilities until I arrived at what I thought the best approach was, and yes, sometimes it included barking orders for testing/labs but it was mostly about absorbing the information available to you, asking for further details as to history, and then allowing your intuition and pattern recognition to guide your next actions. Many times the answer/diagnosis would come to me in this way only to be later validated by the testing and/or response to my treatment choice. What is fascinating about these situations is that they are unique to critical care - we were often immersed in medical emergencies which are defined by chaos, urgency, and the need to act on incomplete and sometimes unknowable information.
After I became expert in POCUS, these situations were greatly reduced in complexity and stress because, in many of those cases, within minutes, I would know exactly what was wrong and could turn patients around because I could quickly identify a blown right or left ventricle, a massive pulmonary embolus, an occult pneumonia or excessive fluid in the lungs or a lung collapse, among many other critical diagnoses. It was exhilarating, not only to me, but to my trainees, but most importantly, to the welfare of the patient.
After witnessing some of the more dramatically impactful cases that I managed, my trainees also became inspired to learn this skill set. So I taught while continuously learning, at times from my trainees themselves. We were all learning and teaching this new field together and it was exhilarating. Similar to what me and the FLCCC did when faced with the novel Covid-19 disease. Just sayin.
Anyway, when I finished training, although I was not on a par with Paul Mayo, nationally I was one of the leading experts. So he and I, along with the amazing Seth Koenig, Mangala Narasimhan, and Robert Arntfield (still love you guys even though you haven’t called me in a long time), learned and taught and published together for years. We put together the first local, then regional, then national, then international courses in critical care ultrasonography. We travelled the country and world for years teaching, researching, publishing. It was exhausting but exhilarating. But it was new. And we were setting the standard for the practice of POCUS.
The four of us spent years traveling around the country (and world - Spain and China and Saudi Arabia etc) creating and teaching courses for the American College of Chest Physicians. I did research projects in the field with my residents and fellows year after year. We created and administered the first “certification” exams. We, in collaboration with the Europeans literally set the “standard of care” and “consensus opinions.” The point is that it was us front-line doctors that set the standard of care, not some supposed health care leader or bureaucrat.
I would say that my proudest achievement in POCUS was when I became the senior editor and co-author of the now best-selling textbook in the field, currently in it’s 2nd edition and translated into 7 languages. It even won the British Medical Association Presidents Award for best textbook the year it came out.
But pioneering in medicine is NOT easy. My early years learning and practicing the skill were also spent fighting the specialties of Radiology and Cardiology who were trying to “protect their turf” of using (and billing for) ultrasound to look at the heart and other organs. They said we could never become sufficiently competent and that we would hurt patients instead by making “wrong diagnoses.” I said fine, then come and do your comprehensive heart exam at three in the morning while someone is deteriorating in front of me. That was hard for them to argue that point.
Their obstructionism was driven largely, in my mind, by fear that we would order less “official” and “billable” ultrasound exams. It took us a long time, but we eventually proved them wrong in regards to “making errors.” I will say we certainly may have missed subtleties on those exams.. but.. subtle findings are almost never immediately life threatening. However, I will say that their fears of losing reimbursements were real because I definitely ordered a lot less “formal” ultrasound exams after I developed the imaging skills myself.
Also, I can’t forget the fights with hospital administration, trying to get them to open the pocketbook and buy us ultrasound machines for use in the ICU. This is very hard to do if you also say you wont be billing for the exams you perform (sometimes we falsely promised we would bill but then didn’t - writing formal reports and billing took too long during a busy ICU day).
So how then did we succeed in equipping every ICU in the country with an ultrasound machine as the standard of care? We argued that it was for patient safety and based that argument on the fact that many of the procedures we do in the ICU were made much much safer with the aid of ultrasound guidance. Hospitals don’t like lawsuits or patients injured. Ultrasound drastically reduced procedural catastrophes and lawsuits. Although rare occurrences, they were almost completely avoidable under ultrasound guidance in trained hands. Without that argument, the field would likely still be in its infancy. Fun fact: I always remember the ads posted in the NYC subway cars for law firms with this copy; “Have you been injured in a vascular procedure? Call Jacobi and Meyer!” The explosion of POCUS in ICU definitely reduced their business.
My point is that the POCUS standard of care and consensus was created and driven by true “experts,” which to me, were the doctors or researchers on the front lines. That is why we called ourselves the Front Line Covid-19 Critical Care Alliance in Covid. Not the rear-guard, bureaucratic, Pharma-controlled, pocket-protector, desk-doctor alliance (i.e. the NIH, PFDA, CDC).
The doctors at the forefront of a new disease or practice in medicine will always know more and earlier than the "prevailing” consensus. Whatever the current consensus is, by definition, it will lag behind those of the front-line experts. But in California now, if a doctor forms an opinion based on their experiences diagnosing and treating this novel disease, they will not be able to teach those insights to others (“publicly express our opinions”) if it does not comport with the edicts emanating from behind the concrete edifices of our federal or state health agencies. Even if the doctors sole aim is to save lives or to warn a patient from incorrect or toxic treatments, they could lose their license. Beyond absurd. Hippocrates is rolling in his grave right now.
I mean look at the last two and half years. First it was masks don’t work, they they do work, even on a beach in 40 mile-an-hour winds (Clownifornia). Hydroxychloroquine can be used, then it can’t. Lets skip ivermectin here. Then vaccines are 100% effective, then they found they don’t prevent transmission. They are safe, even in pregnancy, then the UK finally admits they have no data assuring safety in pregnancy just before birth rates around the world suddenly start to plummet 9 months after early peak rollout. But now California’s doctors need to shut up and withhold their professional opinion from patients even when they have knowledge of the mountains and myriad sources of data on the toxicity and lethality of the vaccines or the absurd ineffectiveness of Remdesivir, Paxlovid or molnupiravir.
Although many are aware of our achievements in the FLCCC, I am also proud of contributions I made in Covid with non-FLCCC front-line colleagues. For instance, me and Paul Mayo recognized early on that the predominant form of transmission of SARS-Co-V2 was via tiny virus-laden droplets floating in the air and then inhaled by others when in the same indoor space. This was the reason why the illness spread so easily and in such massive numbers. We tried to alert the country to this fact by writing an Op-Ed which was initially accepted by the New York Times in April 2020. Unfortunately for us, the NY Times dropped our Op-Ed after half the Op-Ed board got fired when they published the controversial Senator Tom Cotton editorial that called for the military to quell the BLM protests. Later we were able to publish it in USA Today. But get this: we called airborne transmission at a time when the CDC and the WHO said it was not occurring. It was not for another year that the CDC admitted it, and even longer for the WHO. If I had been licensed in California and this law was operational at the time, that Op-Ed would have ended my career?

Another little-known contribution was when I wrote the first paper identifying the pulmonary phase of Covid, not as a viral pneumonia (which it largely isn’t), but as an “organizing pneumonia” (a non-specific inflammatory response of the lung to injury) and whose mainstay of treatment is corticosteroids. My co-author was one of the top chest radiologists in the world (he led the U.S task force which did the initial review of all the chest CT scans that came out of Wuhan). The paper literally resulted from a discussion of the clinical and radiographic observations we were making… on the front lines.
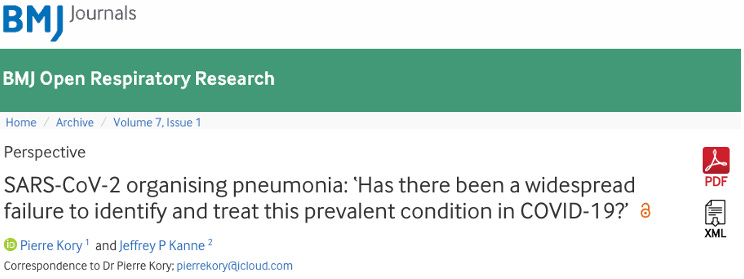
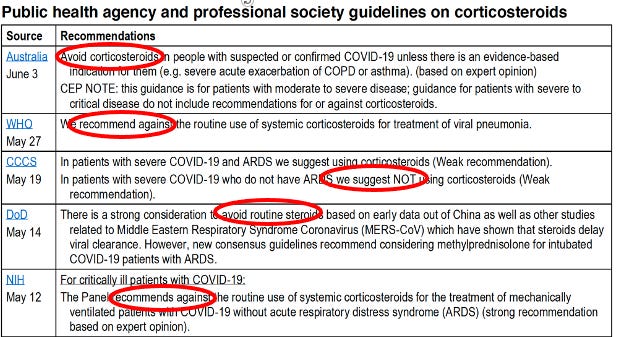
In that paper, I argued for widespread corticosteroid use at a time when all the national and international health care agencies were recommending against use.
We submitted the paper to 6 journals before it was finally published 4 months later. By then corticosteroids had become the standard of care worldwide. Again, I wonder what would happen to me if I had done that under this law in California.
Now, my license could be revoked if I recommend against Remdesivir, a joke of a drug in the hospital phase of this illness. Because if I do, that would be going against the “standard of care” in this country. This requires ignoring the fact that much of the world does not recommend its use in hospital. If my scientific opinion on the vaccine is like Denmark’s, which doesn’t vaccinate children against Covid and doesn’t recommend vaccination for low risk folks under 50, I will lose my license.
So, to wrap up, you can see that I might have some “issues” with that California law. Someday I will tell you how I really feel about it :).
I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amounts of time I spend researching and writing my posts, so again, thanks.
P.S. I opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.S. I am writing a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for:
I enjoyed this immensely. Thank you so much for sharing your life experience. You are a remarkable person and we are so thankful for your gifts and advocacy. 🙏🏻
Wow wow wow. You mean to tell me you practiced medicine and then adjusted your standard of care based on new data?? Truly mind blowing 🤯🤯🤯