

Establishing "Standards of Care" in Medicine - Part 1
A largely autobiographical journey down memory lane of my prematurely ended academic career.


This post originated from an early draft of a previous post (and Op-Ed on Foxnews.com) criticizing California’s new law which makes it essentially “illegal” for doctors there to freely express their opinion on vaccines or other medical matters if they differ from the supposed “consensus.”
In that initial post, I was trying to go deeper into the main language of the bill which was to “revoke the license of any physician who expresses an opinion contradicted by contemporary scientific consensus to the standard of care.”
Despite the fact that sentence is somewhat nonsensical, I ended up opining on the absurdity of determining the “standard of care” of a novel, rapidly evolving, insanely complex disease. I mean, how many “standards of care” in Covid have now been debunked or reversed? We know so little and need to know so much more, to pretend there could be such a thing as a “consensus” standard of care so early in a novel, bio-lab engineered disease was insane.
As a result of my Covid journey, it is now my belief that “standards of care” such as the ubiquitous infusion of Remdesivir into every hospitalized American’s arm has nothing to do with science. Instead, the “standard of care” in Western medicine is that it is a “care requirement established by Big Pharma via manipulated trials, captured medical journals, Health Agency proclamations, and financial incentives instituted through the passage of federal legislation.”
Science, which I always thought operated through methods such as “hypothesis, experimentation, discovery, innovation, debate, and free exchange” is no longer. Instead, these pre-determined, non-scientific care standards promoted by Big Pharma are enacted by servile bureaucrats intent on preserving their jobs, stature, and future employment (or grants or political campaign funding). I literally never could have imagined how controlled and corrupted the body of Medical science is, particularly around any therapeutic that either threatens or can explode Pharma’s profits.
Anyway, the point is, my first draft started exploring my own career experiences with innovating and setting standards in my own specialty. I went deep into my own history but then I scrapped it because it got too personal and too far away from the issue I was trying to explore. But I saved it. Thinking I would share it in a later, separate post. Here goes (another motivation to write the below is that I needed to add some personal history to my soon-to-be completed book called “The War on Ivermectin”).
My initial focus in that early draft post about the California law was on one of the core responsibilities of a physician, enshrined in the Hippocratic Oath, which is to add knowledge to the practice of medicine. I always took that part of the oath very seriously and essentially committed my career to it, not out of some moral or ethical imperative, but mostly because I loved teaching, clinical research, and clinical innovation. So I became what is called a “clinician educator,” i.e. someone who is heavily involved in both the care of patients and the teaching and researching of that knowledge and skill to physicians in training. What “outsiders” to Medicine may not know is that there are largely just three categories of doctors that take care of patients:
A clinician - these are doctors either in private practice or, if they work in academic institutions or health systems, their entire work week is seeing patients or performing operations (if a surgeon). Occasionally, they may be asked to mentor a medical student or oversee a teaching service of residents for a few weeks a year. They do little to no research and are not paid for time spent teaching or mentoring students, residents or fellows. Their teaching obligations are usually a requirement for having privileges to admit to and/or operate at a hospital.
Although some are brilliant and deeply read and are at the forefront of their field, most either have no incentives or time to keep up with the latest research, insights, or evolutions into care approaches and instead rely on the latest “guidelines” to be updated from their respective professional societies. Further, the lack of exposure to students and trainees that tend to ask a lot of challenging questions removes a motivation and incentive to stay on top of the latest literature or science (students and residents are often well-read up on emerging topics because they have the time and are eager to learn).
A clinician-educator. These docs (like me) are only found in teaching hospitals or academic (university) medical centers. Although we have outpatient practices and/or run inpatient care services either on medical wards or ICU’s, the care we deliver is via an “apprentice” model.
The apprentice model works as follows: our students and residents or fellows see our patients first and then they present to us the information they have gathered and the proposed care plan they have created. Then they observe us while we further evaluate and decide on the ultimate treatment approach of the patient. I talk to my patients and trainees at the same time - my trainees are listening and observing my patient interactions as I explain to both what I think the problem is and how I think we should further diagnose and/or treat. That is how they learn. It is how I learned (in my case, I was incredibly fortunate to have had the opportunity to observe absolute masters at the discipline). That is the apprenticeship model, and I had 15 years of apprentices under my belt. My days as a teaching physician in the ICU are best illustrated by the television show Dr. House - during patient care rounds, I was followed and listened to by a team of up to 12 trainees and/or ancillary specialties involved in the patient’s care like Pharmacy, Nutrition, Social Work, Respiratory, or Physical Therapy practitioners.
Physician-Scientist - these doctors are only found in large, academic research institutions where their time is split between writing grant proposals for research funding, doing research, and publishing papers while also having either or both patient care and administrative responsibilities (such doctors often rise to various administrative leadership positions in these centers).
Generally, in my experience, these doctors arrogantly considered themselves more valuable and/or expert than the others. I would agree that they are the most valued doctors by the academic institutions they work for, but I maintain they were far less valued by their patients. Why? Because they are “scientists” first - i.e. they have “labs” and they spend lots of time writing research grant funding proposals to major institutions like the NIH. When they win research funding, the institutions they work for receive a lot of money in those grants to pay overhead and other costs, and so they are heavily recruited by “the top academic medical centers” because they are, in mafia language, “earners.”
Side note: this is also how the Federal government essentially controls all of academic medicine. Good luck trying to get funding to research a subject or a medicine that Godfather Fauci and his paymaster Big Pharma does not want studied. Also good luck if you are the Dean of one of these academic centers and decide to publicly express an opinion which contradicts Fuhrer Fauci. Hundreds of millions of funding could be jeopardized. And that is why this pandemic should also be remembered for “the Silence of the Deans” as their cardiac and stroke units and cancer and hospital wards filled with ever younger patients presenting with catastrophic illnesses that they had never presented with before. They remained silent. All of them.
Anyway, “physician-scientists” also spend a lot of time trying to publish as this brings further funds, stature and recognition. If you can win large grant funding for a research institution, you are almost an untouchable. Now, I have no problem with what they do, except if I were their patient. They were.. not the best at patient care as they were often derisively called “lab rats” by the pure clinicians, as in “Who is covering the ICU next week? Say it isn’t one of the lab rats!”
And that was because you simply don’t want someone taking care of you who takes care of patients only 6 weeks a year while spending the other 46 weeks doing experiments, writing grants and publishing papers. For instance, when I was recruited by the University of Wisconsin, up to that point in my career, I had been doing 20-26 weeks of inpatient clinical services a year (along with daily/weekly outpatient clinic and other responsibilities). I was shocked to discover that some of the “physician-scientists” at UW were assigned to patient care services only 6 weeks a year. The rest of the time they were in their labs and/or writing grants or teaching or administrating. What is funny is they proudly considered themselves “triple threats”, i.e. “superstars” in research, education and patient care.
The vast majority were nowhere close to mastering all three, and their deficits were typically in patient care (I knew only a handful of masterful exceptions in my career). Although often highly intelligent and I presume excellent in designing and running experiments in their labs and writing grants, I found that most were average at best in terms of patient care. They tended towards rote administration of standard treatments while robotically citing the major studies or guidelines to support their decisions. Boy were they expert at guidelines. Which would work out great if patients were standard or if the published literature literally represented the “best” approaches to treatment but in a significant proportion of patient situations, it just doesn’t work out that way. Predictably, they were often resistant to data or arguments which I put forth that suggested the “guideline” approach may not be optimal. Hearing them cite those guidelines back to me while I was arguing for different approaches left me with PTSD and is one of the reasons why, soon after I left UW in April 2020 to fight Covid on the front lines in New York City, I remember telling the clinician colleagues that I reunited with that I felt like “I had left a cult.” I believe that even more now.
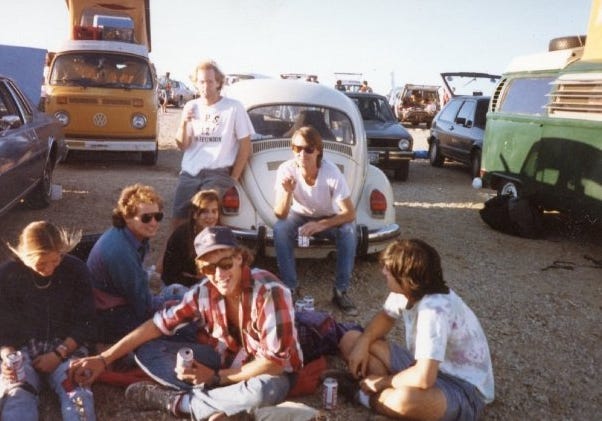
Picture of my ICU team on the roof of the hospital during a break after ICU rounds. New York City, April 2020, a week after resigning from the University of Wisconsin.


So, how did I end up being a clinician-educator? Well, growing up, the big question to answer was “what do you want to do in life?” and/or “what are you going to be?” Especially before and during my college years. Problem: I was an unfocused, uncommitted, hedonistic young man, erratic and with the typical undeveloped forebrain of a late adolescent/young male American adult. I definitely looked the part in High School (if you look really close, you can see a gold chain, yikes):

Although I was smart enough to crush standardized exams without a worry, I didn’t know who I was or what I wanted to be really. But I did discover a couple of things in college: I hated business, sales, and a sole focus on making money. I loved literature but couldn’t write at the time, I was not interested in politics or any field that was not directly and immediately or broadly impactful to present societal circumstances. So I decided that I wanted to become either a doctor (like my father) or a teacher (like my mother). I thought those were impactful pursuits and fit with what I liked (math and sciences) and was good at (discussing, teaching, and learning with others).
Since I was really good at math and calculus I ended up obtaining a degree in mathematics from the University of Colorado in Boulder. Problem: Boulder, like every other U.S College it seems, was a massive “party school” and I was a highly “social being” (ah hem). I managed to graduate but with a declining GPA over my college career, so much so that I graduated with a 2.67 GPA, and two years later than expected. Although not proud of this feat, I think it is near impossible to find a U.S doctor who had a 2.67 GPA in college.
A picture of me as an undergraduate. Sums up everything about that time really.
I was a bit of a mess when I left college. No direction, no discipline, and no real commitment to a goal. I was often unemployed and although I tried to find, and even started some random jobs like selling life insurance or doing data entry, I couldn’t stick with them. I started to get depressed. But I really wanted to become a responsible and productive member of society. I also felt it was time (23 years old) to make a living so that I could become an independant adult, a “grown-up” as it were (I was jealous of friends who had made it out of their parents house).
I knew waiters could make a decent living, and the work seemed impactful in a certain way, so I bullshitted my way into the restaurant business, applying for a job as a waiter (I had never waited) in a high-end restaurant. I had no idea that restaurant would change my life in the way that it did. Most importantly, it was owned by someone who would later become my best friend and mentor (John Durkin of Trattoria Diane’s and the long-time mayor of Roslyn, NY). Although he was 18 years older than me at the time, he had been just like me at my age so he understood me. We first connected on topics like music and literature (he is one of the most widely read people I have met as well as one of the most deeply intelligent). Later, we became closer and I started to seek out and follow his guidance on a number of matters in my personal life that he himself had successfully navigated when he was my age.
He essentially mentored me in how to become a mature and responsible man and member of society. But when he initially hired me, I was lost. He actually came very close to firing me in the first 6 months for showing up late, hung over, unfocused etc. But, little by slowly, at the age of 23, I changed my life by withdrawing from the “social” scene I was devoting too much time too and I instead started to focus on activities that would help me reach my now established life goal of becoming a doctor.
I made a practice of staying home and reading a lot, heck I even started meditating. By changing my behaviors and activities, my life started to improve. I was given more and more responsibility in the restaurant and quickly began to earn enough money to rent a place of my own.
In order to “erase” the 2.67 GPA in college, I went to graduate school to study health administration, thinking that getting good grades in grad school might help my chances of getting into medical school. I did that full time while working in the restaurant business full time. My first (but not the last) period of overwork in my life! I recall that with the stress and intensity of two full-time pursuits involving a lot of commuting around NYC, I began to develop severe teeth grinding along with massive dandruff. So much so that one night as I was going to bed, I remember passing a mirror while wearing the dandruff medicine shower cap with my teeth grinding protector in my mouth. I looked at myself and was like, what the hell are you doing to yourself man?
But I didn’t care as I was happy in a novel way - I discovered how satisfying it was to make positive contributions, both at work and at school and at home, and for being valued for those contributions. I remember feeling highly motivated, focused, and committed in a way I had never been able to previously. In my first year of grad school I was hired by one of my Professors to manage one of her research projects. Not-so-fun fact: that research project was CDC funded and was focused on studying various financial and other incentives to physicians on how to improve immunization coverage rates in the inner city. Holy shit. Lets forget about that for now. Most importantly, I ended up getting my Masters degree after having gotten straight A’s, something I hadn’t done since the 11th grade :).
Anyway, after years in the restaurant business and after getting my Masters, I started applying to medical schools in the U.S. However, despite strong medical school admission test scores, I will just say that the U.S schools didn’t like my academic background, especially my 2.67 college GPA. Rejection, rejection, rejection. Ugh.
So, I ended up, at the age of 28, making an appointment with an undergraduate college career adviser, looking for some practical advice on how to improve my chances of getting into medical school. Short answer: he advised that I should seek medical training overseas. Brilliant! I literally had never really considered it. He told me about a Professor who taught part-time at one of the overseas schools who had written a booklet with tons of information about off-shore medical training opportunities. I sent the Professor a check for $20 and he sent me his photocopied pamphlet (bound at Kinkos). I read and re-read his pamphlet, and then did further research on the varied strengths and weaknesses of the schools that accepted American medical students like the most known ones in Dublin, Israel, Grenada, Guadelajara etc.
Ultimately I chose St. George’s University School of Medicine in Grenada, West Indies. Here is one, just one reason why:

Another reason was that I have been a life-long obsessive windsurfer later turned kitesurfer. I literally windsurfed most days in Grenada while studying well into the night. This sets up a perfect chance for me to show off some of the non-medical skills I acquired during medical school:
I ended up starting medical school there at the age of 29 (nearly all of my fellow students were much younger at 22 or 23). My experiences over the next 4 years could fill a book, but I deeply appreciated learning medicine in such drastically different health systems, like in Grenada, St. Vincent’s, Barbados, and the United Kingdom. I graduated at 32 and landed an internal medicine residency spot at St. Luke’s-Roosevelt in NYC (Upper West Side and West Harlem) and then a fellowship training spot at Beth Israel Medical Center in the lower east-side of Manhattan. I ended up finishing my training with three Board certifications - Internal Medicine, Pulmonary, and Critical Care (and a Testamur status in adult echocardiography from the National Board of Echocardiography).
I was 38, living in NYC, married with two daughters, $150 dollars in my bank account and not one dollar in a retirement fund for me or college funds for my daughters. Plus me and my wife had student loans. Gotta start somewhere. At the risk of foreshadowing, the academic career that I embarked on at 38 years old.. ended in Covid at the age of 50. 12 years only. Paul and Umberto and Joe and Jose of the FLCCC are are literally 30-40+ years in their careers which makes me the wet-behind-the-ears newborn of the group.
Looking back on my choice of specialty, I chose a doozy. When physician specialties are ranked according to an index of earnings vs. quality of life, the top four are what we intensivists derisively called the “ROAD” scholars, meaning Radiology, Opthalmology, Anesthesia, and Dermatology. The word play refers to the fact they were the most desired and competitive specialties because of the amount they earned vs. the stress and amount of hours they needed to work. These were also highly sought because of less burdensome “on call” responsibilities, i.e. covering hospital units and acutely ill patients off hours, overnight and weekends.
The “ROAD scholars” generally had the most manageable work hours while being the most highly paid. Conversely, at the bottom of the 50 specialties on this scale sit three: critical care doctors, family medicine doctors and pediatricians. We have the worst “quality of life” compared to our earnings apparently. But to be fair, of the three at the bottom, ICU doctors make the most so don’t bring out the violins. In fact, ICU doctors, compared to most specialties, do very well in terms of income, but when you factor in the hours and stress, it drags us to the bottom of the most desirable specialties. I know this from coming home after a “normal” day in the ICU, trying to sleep while thinking and perseverating over what I may have missed in a patient dying under my care. It was insanely stressful, especially in my early career when you were often unsure about a lot that was going on with a patient. In fact, I would say that the first two years of my career as an Attending in the CU were the hardest and most stressful. I would wake up, immediately thinking of the patient I was most worried about. Taking the train into work I would think research and google about my hypothesized reasons for their illness and trajectories which always precluding me from working on a paper or reading the news.
Not sure what my point is here, except to maybe have reconsidered my choice of specialty. Not really a choice because I loved ICU medicine. The reason why I became an ICU doctor is because during my general medicine training I felt that the ICU docs were the “baddest of the badasses.” I was intimidated and admiring of their broad knowledge base and diversity of clinical skills. I also admired that staff from any area of the hospital, whether it be Labor and Delivery, clinics, rehab, hospital wards etc, immediately called for an ICU doc when a patient suddenly “really didn’t look well.” The ICU docs were expert at the widest variety of illnesses, and especially in their most severe forms, i.e. cardiac failure, lung failure, endocrine failure, liver failure, kidney failure, brain failure. They would come stabilize and treat the “sickest of the sick.”
And that is what inspired me, wanting to be like the intesivists who could so calmly and expertly navigate those stressful clinical situations. I recall being quite intimidated when I made that decision because I didn’t think I had what it took. What is interesting is that my wife was an intensivist by that time so she was able to help reassure and encourage me to follow in her footsteps.
Super fun fact: one of my greatest achievements in life was asking out my wife. Why you ask? Because I did so as a 4th year medical student wearing a short white coat. My wife at the time was a senior resident at the end of her training and thus had earned the right to wear a beautiful long white coat.. and she was intimidatingly beautiful. If you are not in Medicine, I don’t think you can understand the challenge of a medical student in a short white coat asking out a senior resident physician. Like my best man John (highly successful restaurant owner and chef) said at our wedding, “I always wondered why Pierre was so nervous to ask out Amy, but I finally got it. In my business it would be like the dishwasher asking out the chef!” Exactly.
So, I was three years behind her in training and she was one of the best doctors I knew. I saw what she did and how she did it and wanted to be like her. Problem: after we started dating, I was forced to listen to her wake up in the middle of the night for years, taking histories and dictating treatment plans to young residents and fellows across four major NYC hospitals while I was in a barely arousable coma. I thought what she did was insane. Up all night managing patients on the phone at four different New York City hospitals, only to get up and put in a full day in the ICU. What was I getting myself into? But, again, I thought she was a badass. And I wanted to be like her. So I decided to follow in her footsteps. Little did I know that raising three girls with a wife who was also an ICU doctor in poorly resourced and uber expensive New York city would eventually lead me to burn out to a point where I allowed myself to be recruited by the University of Wisconsin (where my wife is from). A life-long New Yorker decided to move his family.. to Wisconsin. What the hell was I thinking? A picture of my wife (we had her model for the cover of the brochure of the annual POCUS course I gave at the University of Wisconsin)
The rest of my hagiographic recounting of my academic career and the standards of care that I helped set are in Part 2 here.
I just want to say thanks to all my subscribers, especially the paid ones! Your support is greatly appreciated as it allows me to devote what is often large amounts of time I spend researching and writing my posts, so again, thanks.
P.S. I opened a tele-health clinic providing care not only in the prevention and treatment of acute COVID, but with a specialized focus on the study and treatment of both Long-Haul and Post-Vaccination injury syndromes. If anyone needs our help, feel free to visit our website at www.drpierrekory.com.
P.P.S. I am writing a book about what I have personally witnessed and learned during Pharma’s historic Disinformation war on ivermectin. Pre-order here for:
Few key points:
•A primary why reason “standard of care” matters is because the bar for malpractice can only be met if amongst other things it is proven that the physician deviated from the “standard or care.” This is a major reason why physicians are so hesitant to question guidelines, and was a legal precedent I suspect was deliberately instituted so physicians would be forced to practice pharmaceutical based medicine.
•Breaking medical practices down into standardized algorithms is excellent for training AI systems to replace doctors.
•Anytime a system fails, people will try to “improve” it by reducing it to what caters to the lowest common denominator. Because there is so much variability in what people (especially complex patients need) this essentially synopsizes why the standard medical care fails for so many patients.
•I love to read medical journals from earlier eras, because at that time the physicians experimented without IRB approval, went with their best guess and had a lot of very useful insights I’ve been able to adopt into my modern medical practices (e.g., what was documented during the 1918 influenza helped me come up with many of my initial COVID-19 protocols).
•Patients really, really, appreciate when you educate them, but the way most doctors “educate” their patients is by telling them to copy/do some standard guideline without explaining why…which in my view is not teaching them.
•My best mentors were clinicians who felt an obligation to pass on their knowledge to me and were not locked into the academic/medical system. Because of what I own to them, I give a lot of energy to training younger doctors without receiving compensation for doing so.
•The physician scientists (also known as key opinion leaders) are routinely targeted for pharmaceutical bribes since they provide the best return on investment for promoting pharmaceutical drugs. The archetype of this archetype is Fauci, who has directed tho treatment of COVID-19 despite having almost no experience working with patients for decades.
•Totally makes sense that you went to UC Boulder. A lot of people who have jumped on this new political wave are hippies who realized the current political structure no longer supports many of the fundamental progressive values.
•I feel like almost every public health project revolves around increasing the coverage of standard medical interventions.
•“I would wake up, immediately thinking of the patient I was most worried about. Taking the train into work I would think research and google about my hypothesized reasons for their illness and trajectories which always precluding me from working on a paper or reading the news.”
This is probably why you ended up becoming a good CCU doctor. In my case, a lot of my knowledge has come from forcing myself to engage really challenging situations and learning from them.
Dr Kory, Thank you so much for sharing your personal story I knew immediately after watching your first Homeland Security testimony (at the behest of Sen. Ron Johnson), that you would be the Dr I would want treating any of my beloved family members. I shared the FLCCC MATH protocol with hospital staff in May of 2020 As my elderly Mom was being treated for a UTI. Your story makes you exactly who I thought you were and I hope others are willing to read it. Never, Never, Never give up!